




|
|
|
|
|
||
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
||
Temporary Abutment
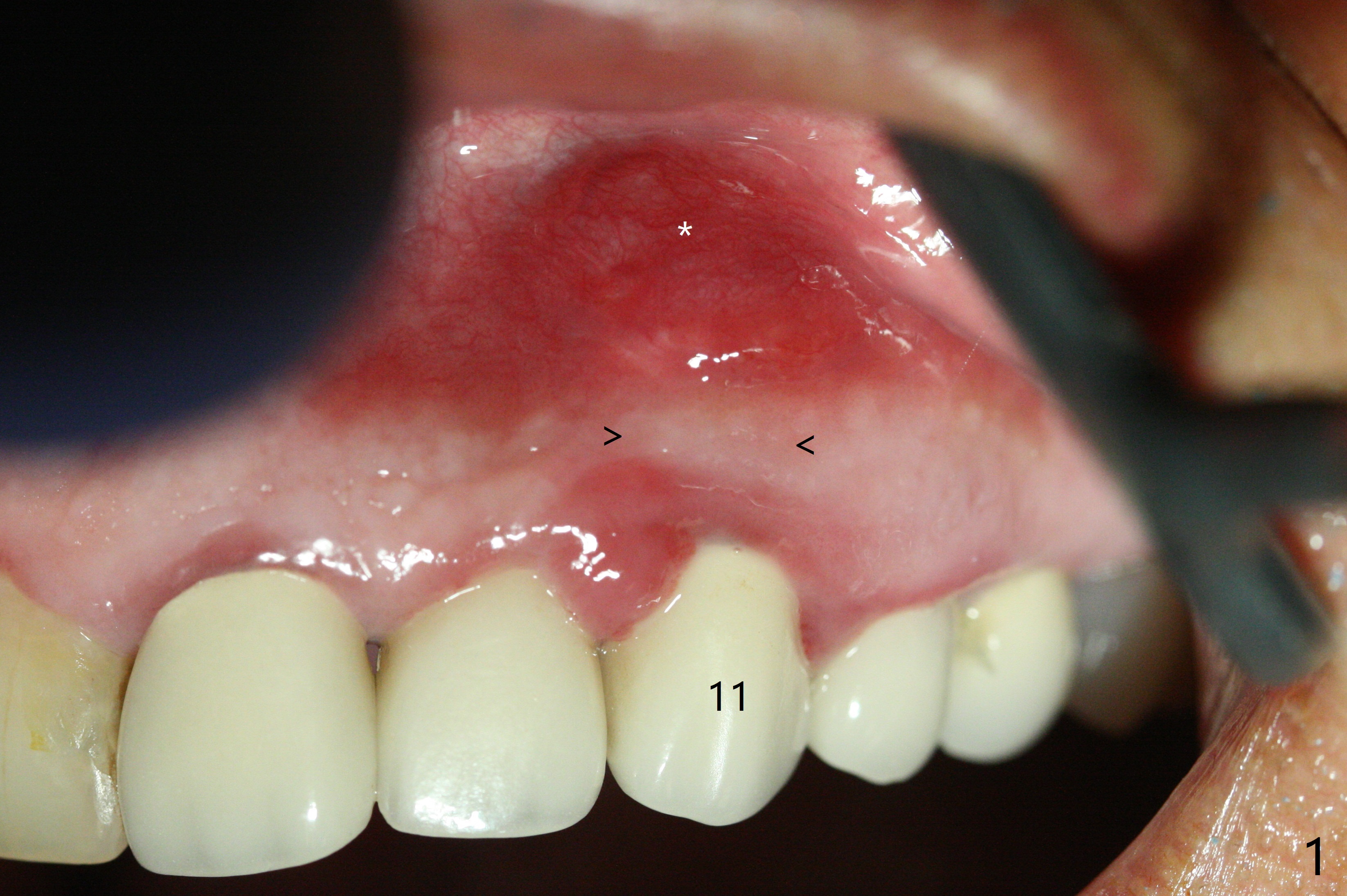
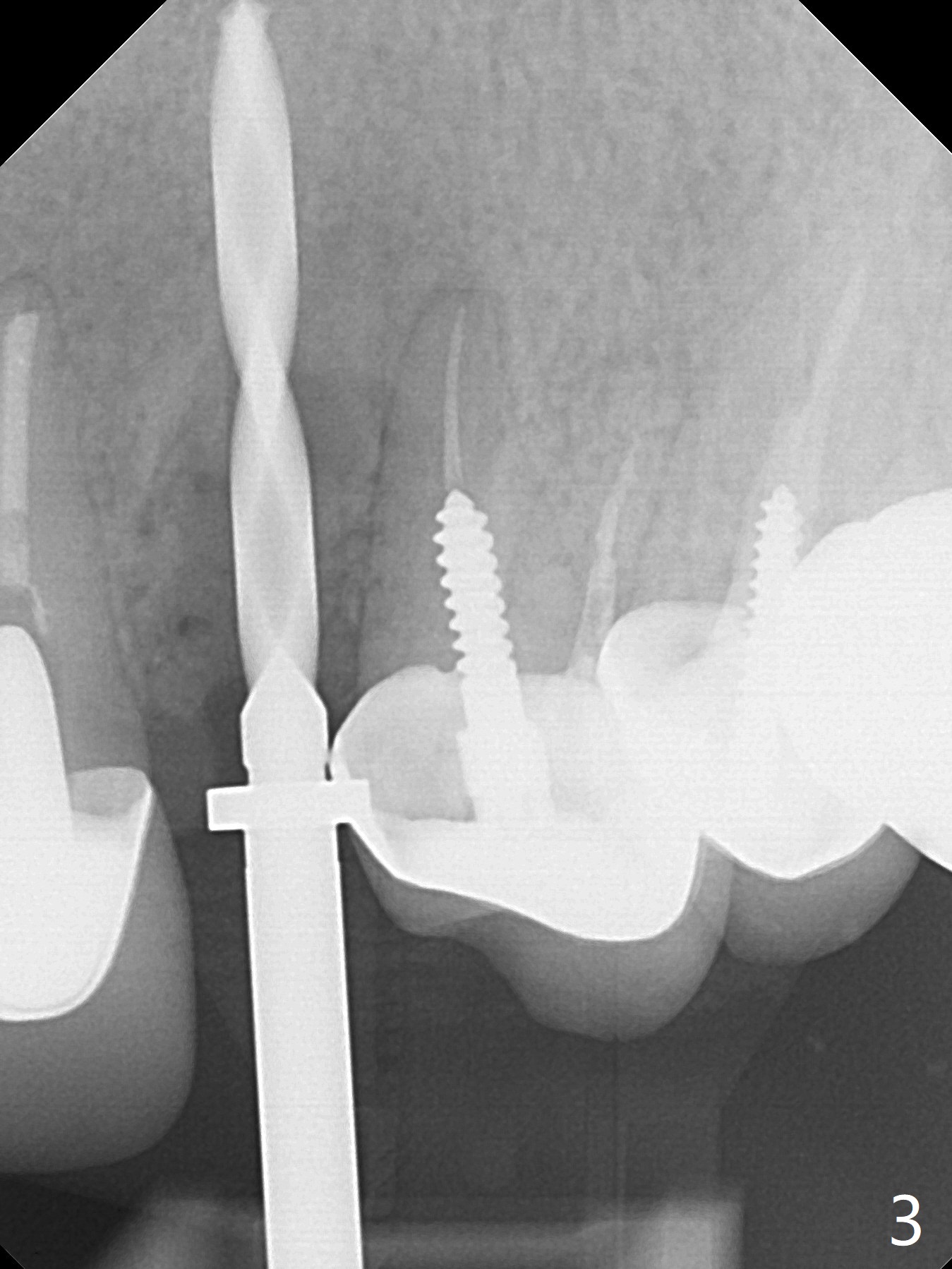
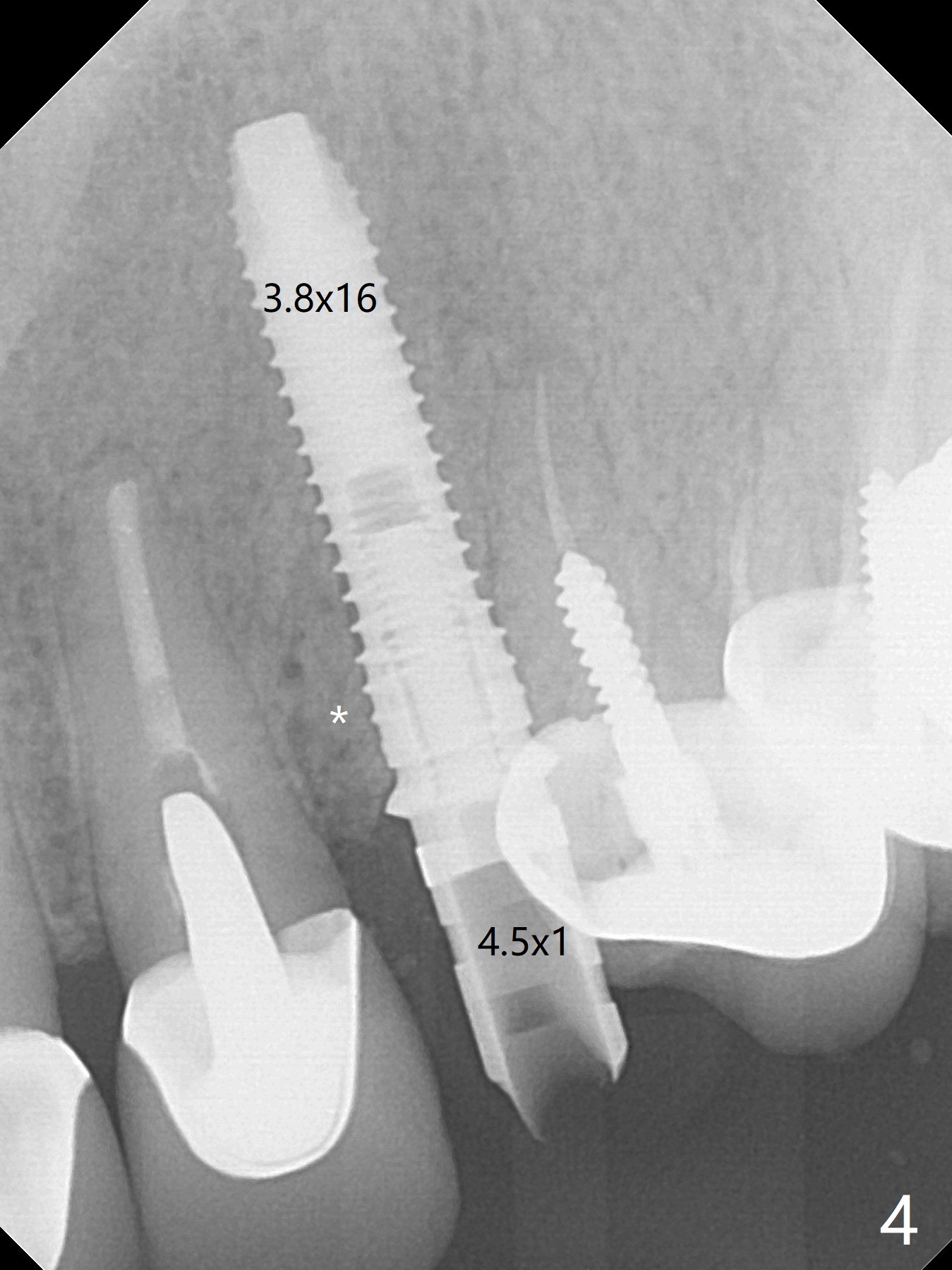
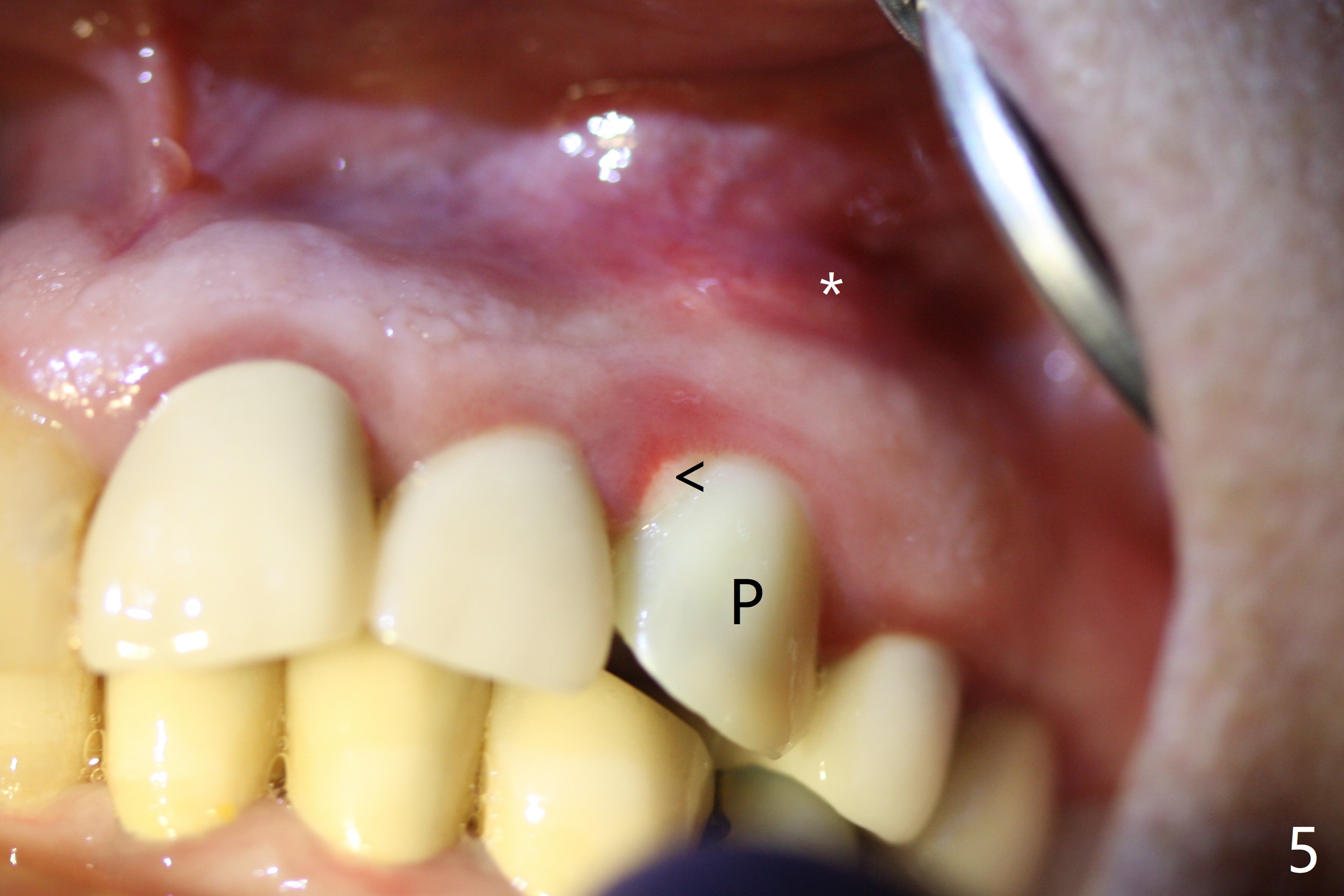
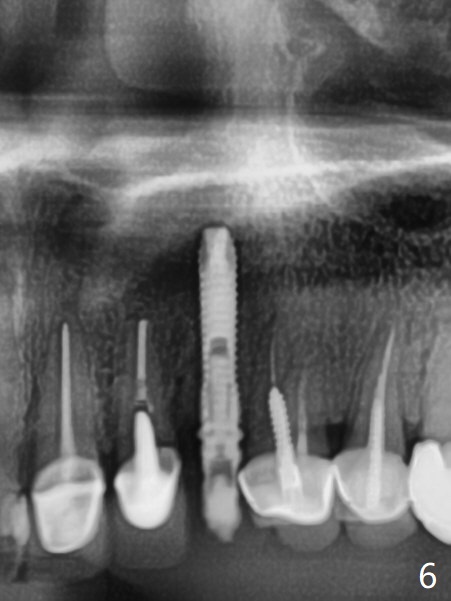
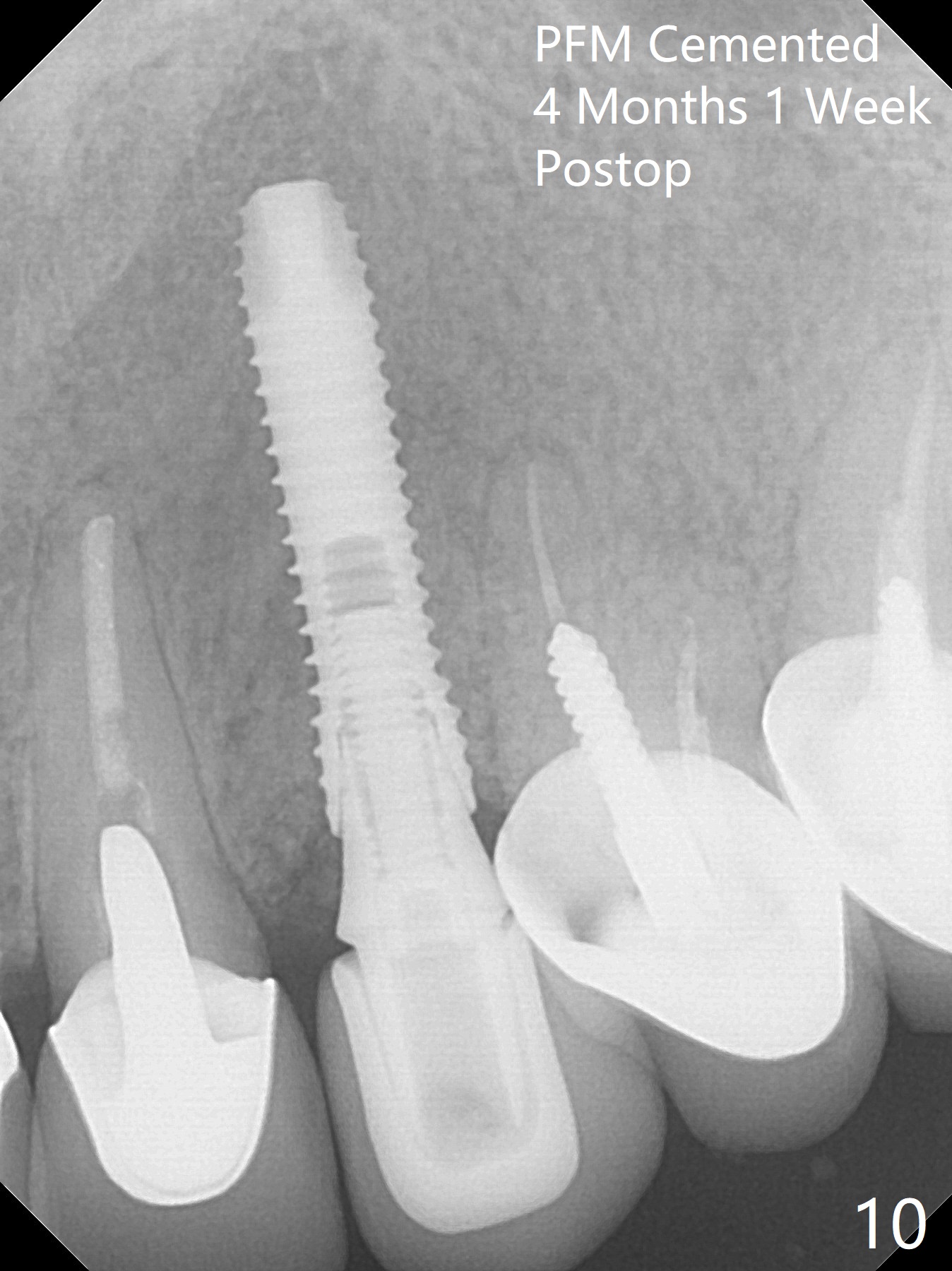
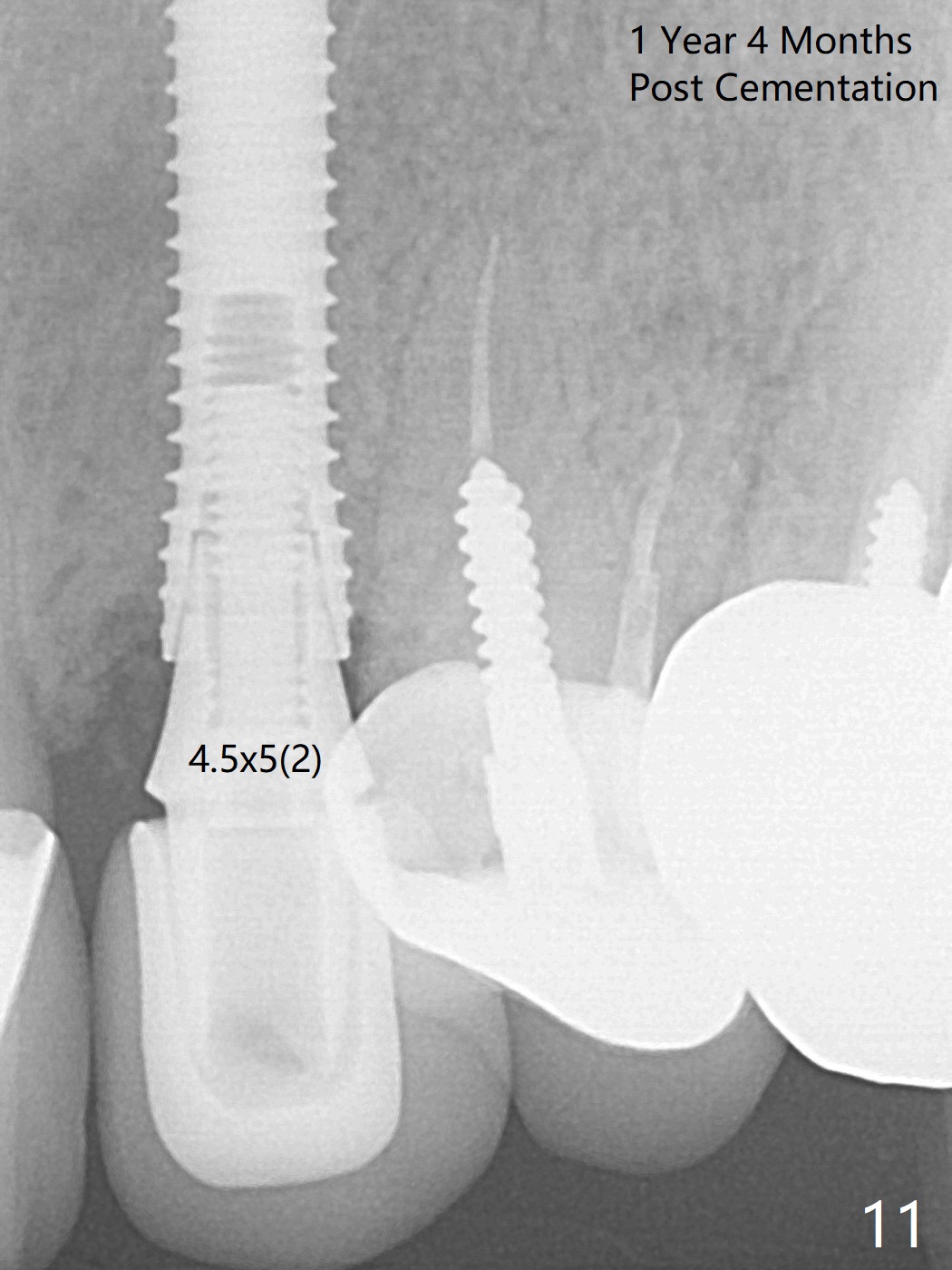
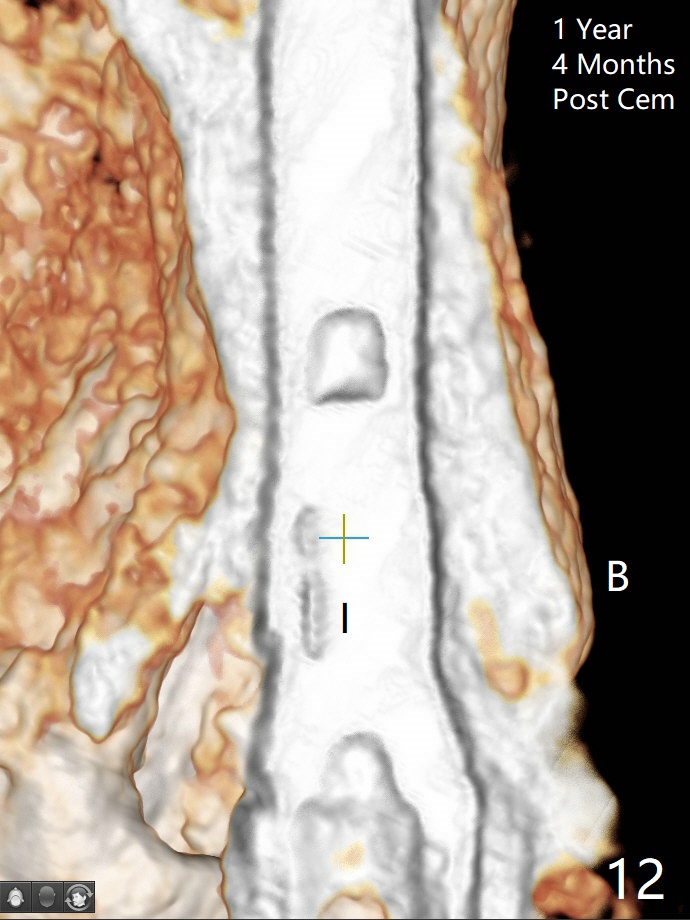
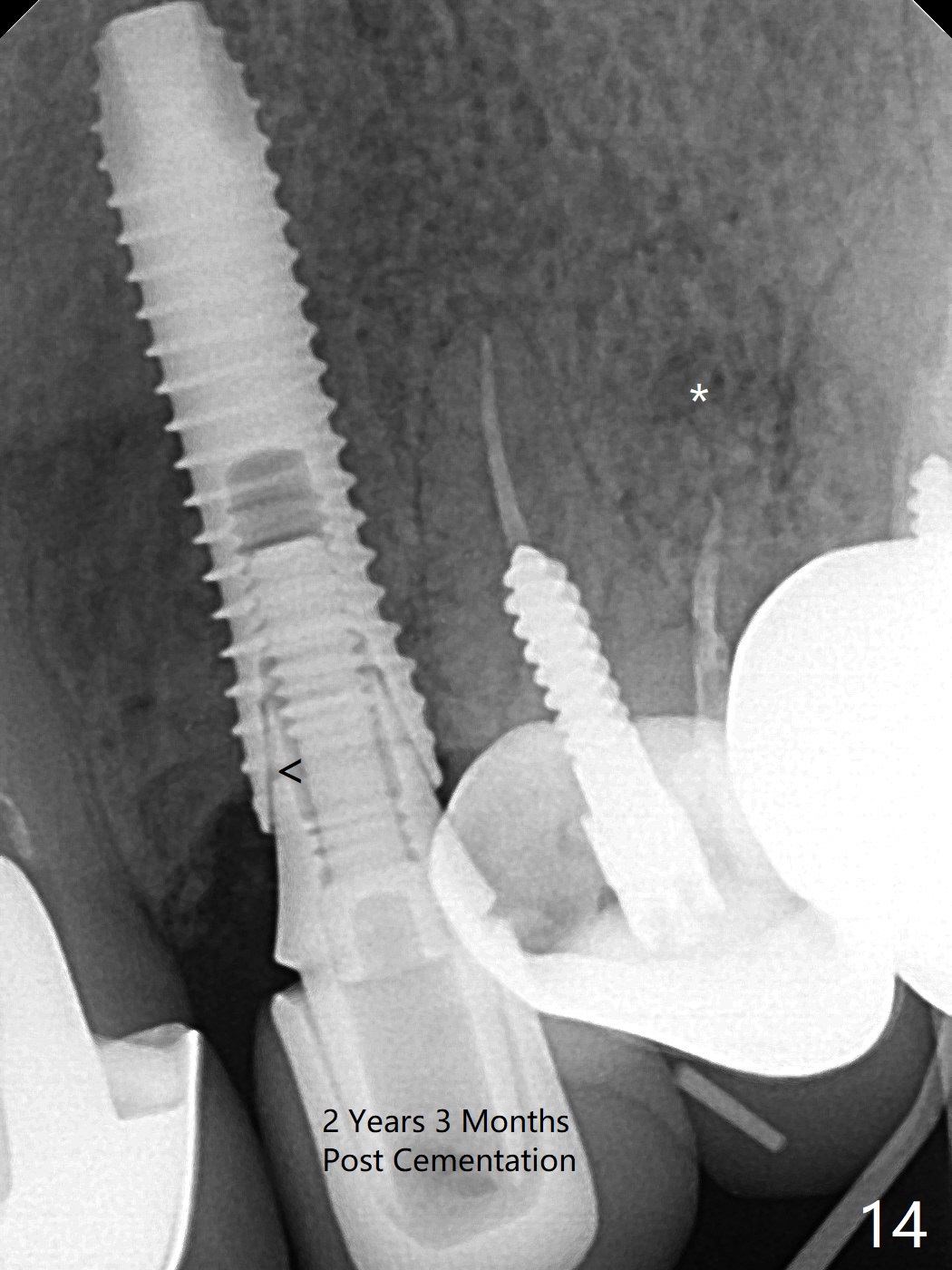
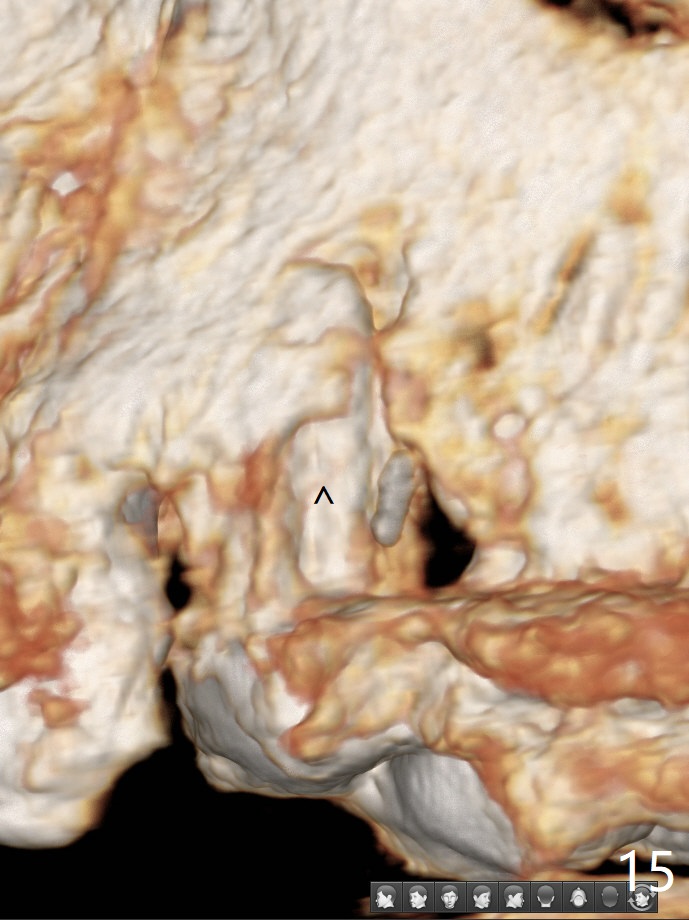
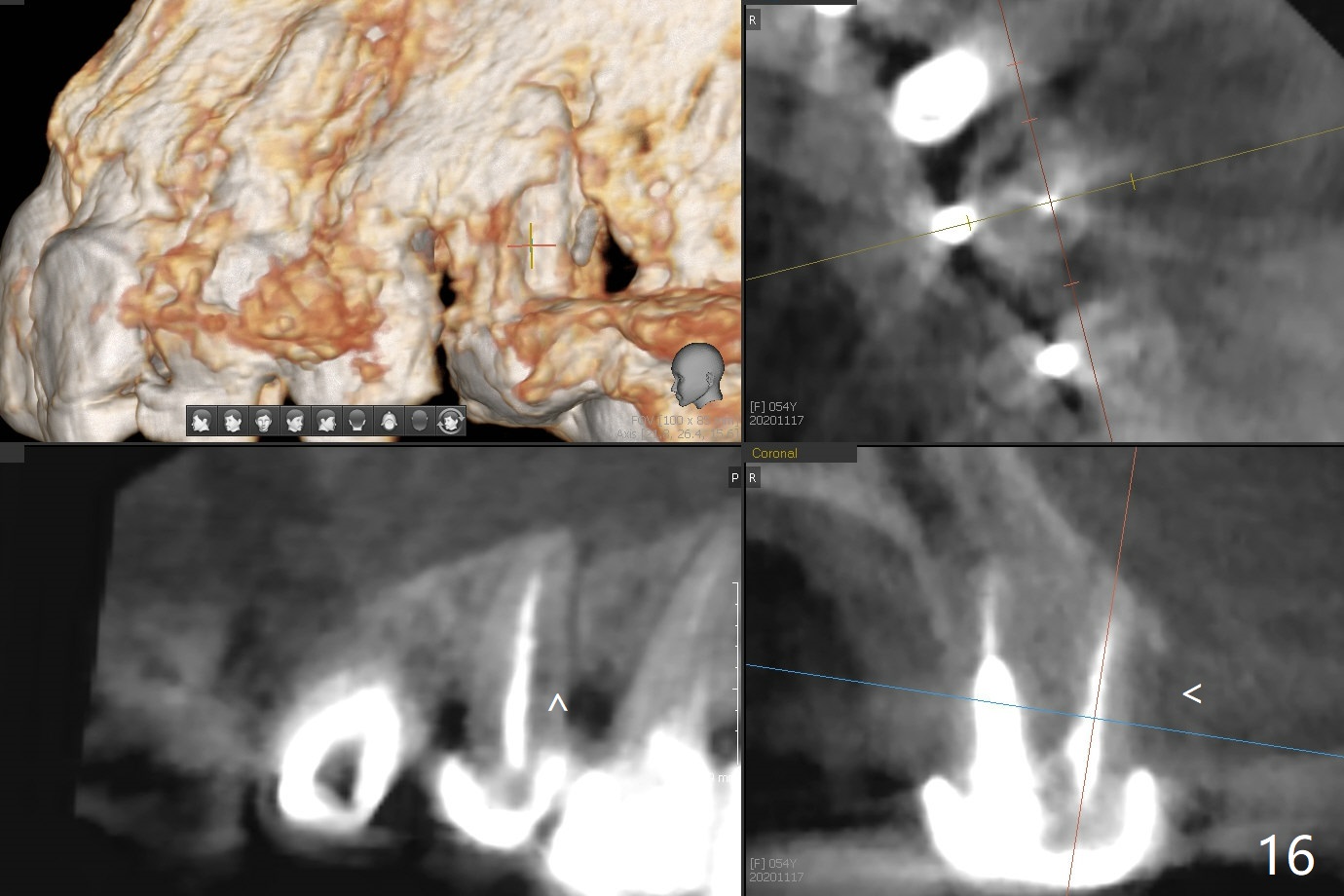
In spite of severe apical infection (Fig1,2 *), a thin narrow strip of the buccal plate (arrowheads, corresponding to the keratinized gingiva) is present when the tooth #11 is extracted. The thin bone keeps the bulging alveolus, i.e., reservoir for bone graft (Vanilla/Osteogen Fig.4 *) after placement of a 3.8x16 mm implant (Fig.3,4). A 4.5x1 mm temporary abutment, placed and trimmed for an immediate provisional, seems to be short in cuff. When an implant is placed deep to prevent periimplantitis, the cuff should be longer, i.e., 3 mm. X-ray should be taken for the depth confirmation after temporary abutment placement. Eight days postop, the mesial gingiva erythema has subsided (Fig.5 < (P: provisional)), while the apical swelling is no longer tender and most likely due to packed bone graft (*). Panoramic X-ray taken 2 weeks postop shows the clearance from the nasal cavity or the maxillary sinus (Fig.6). While the hard tissue around the implant seems to be healthy 5 months postop (Fig.7), the soft tissue is not (Fig.8). The temporary abutment is changed to a cemented one (4.5x5(2) mm) for impression (Fig.8). Since the neighboring crowns are PFM (Fig.6), the new crown will be made of the same material for shade match. Indeed PFM helps shade match in this case as well (Fig.9,10). Switching abutments (from temporary to cemented) makes it difficult to seat the crown. Post cementation X-ray leaves record for future contact loosening. The buccal gingiva remains erythematous associated with open margin (Fig.11 >) 1 year 4 months post cementation. There is no obvious bone loss 1 year 4 months post cementation (Fig.12). It appears that the crown and abutment need to be changed. Although the gingival margin remains erythematous, the gingival hemorrhage is basically lacking due to better oral hygiene during Shelter at Home (1 year 9 months post cementation, Fig.13). Change in abutment and crown will be conducted post coronavirus pandemic. In fact the abutment is incompletely seated (Fig.14 <). In addition, the tooth #12 is symptomatic with PARL associated with the buccal root (*). CBCT indicates possible buccal root fracture (Fig.15,16 ^) and loss of the buccal plate (Fig.16 <).
Return to Upper Canine Immediate Implant, Armaments No Caries #3 19 Guide Ridge Split Clindamycin
Xin Wei, DDS, PhD, MS 1st edition 04/13/2018, last revision 11/24/2020