
.jpg)



|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
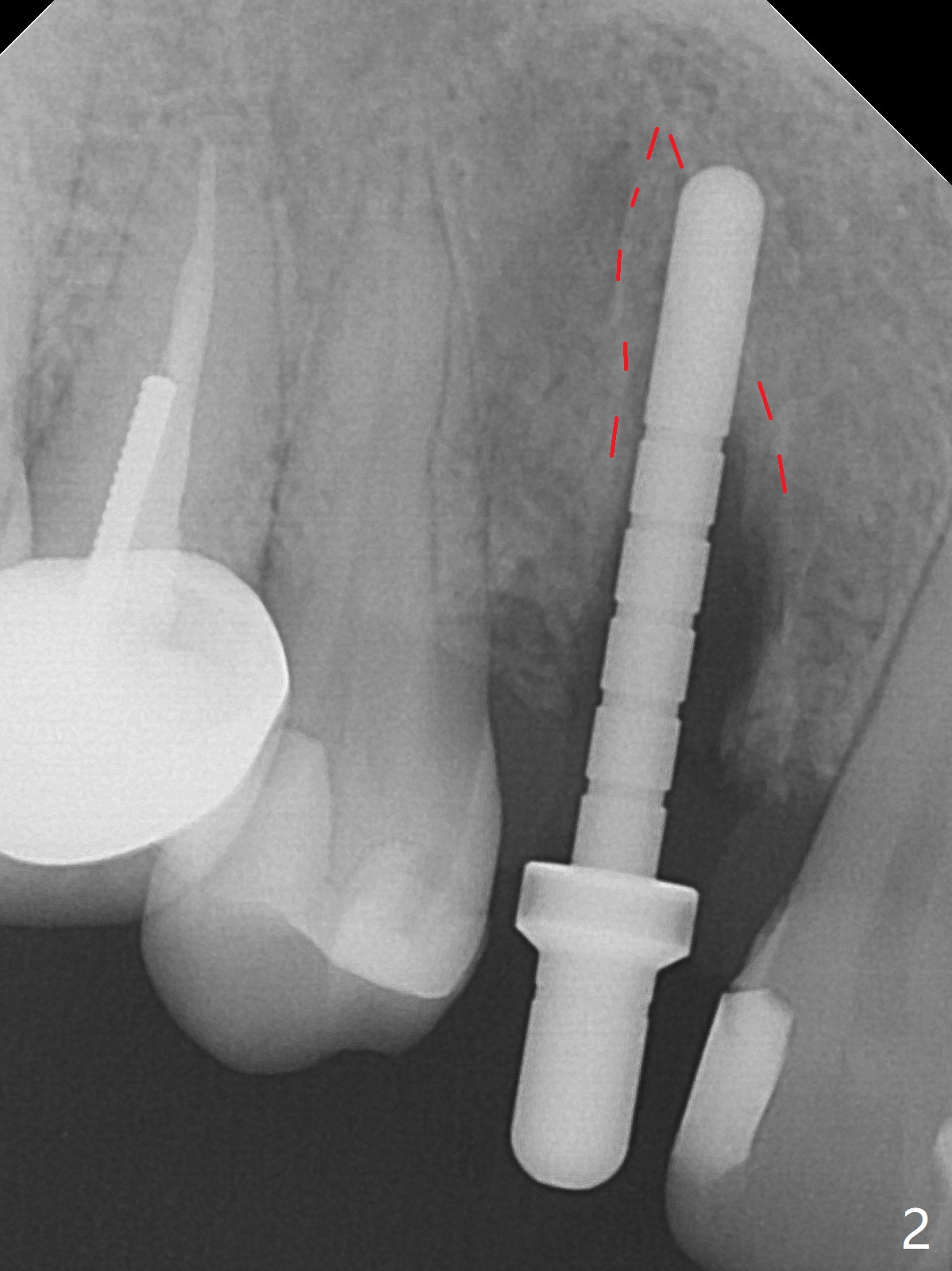
Thin Buccal Plate
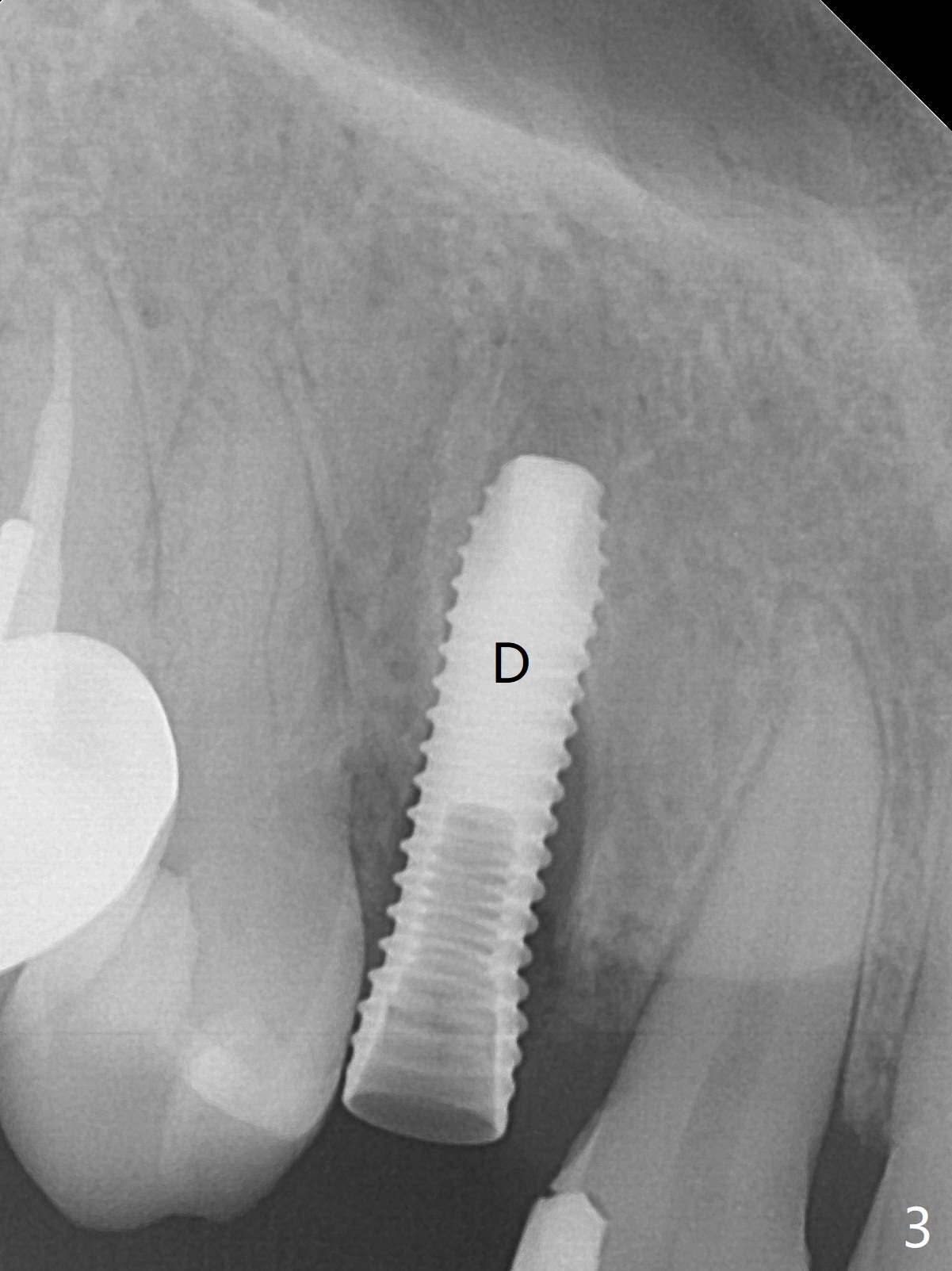
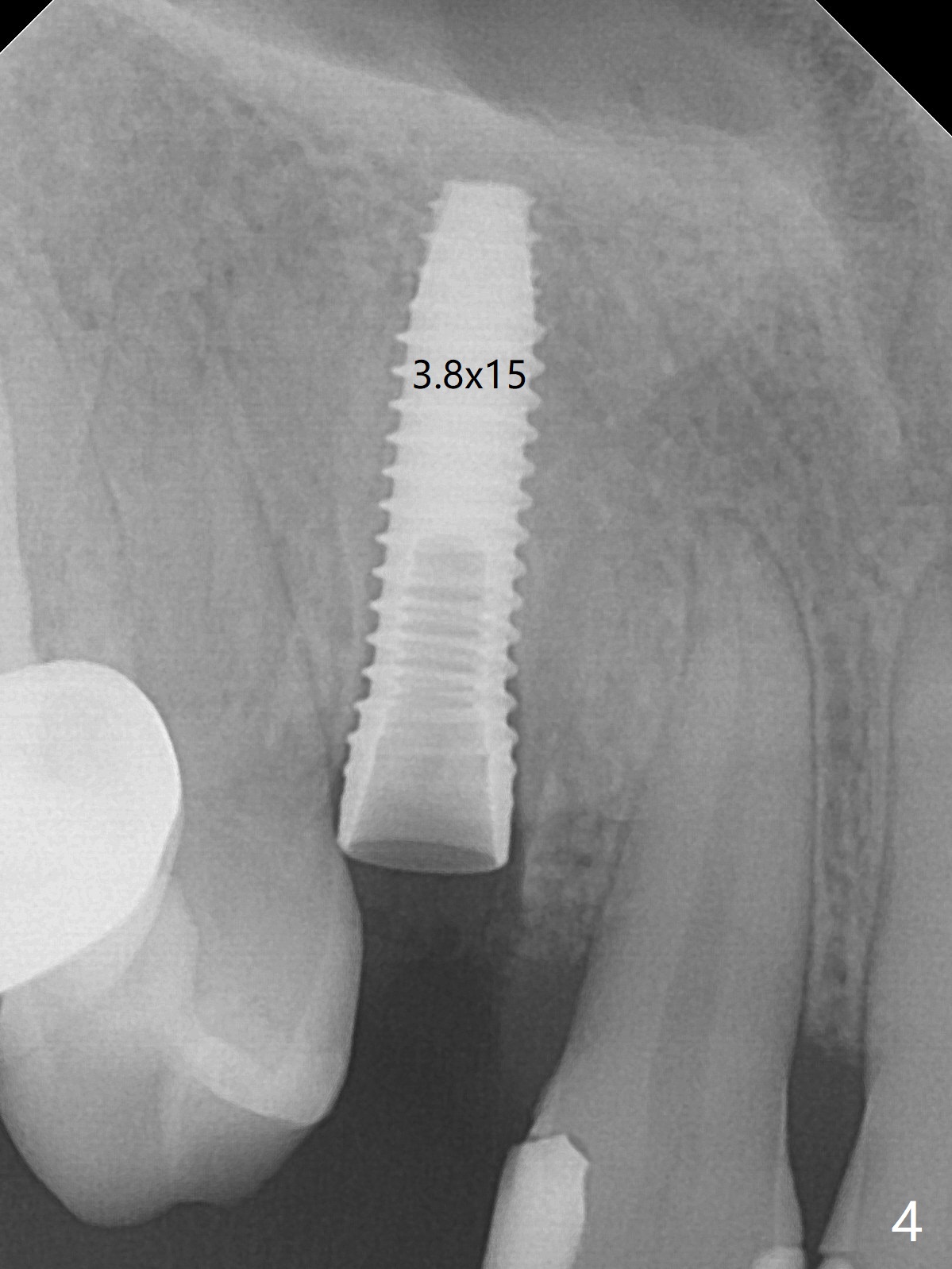
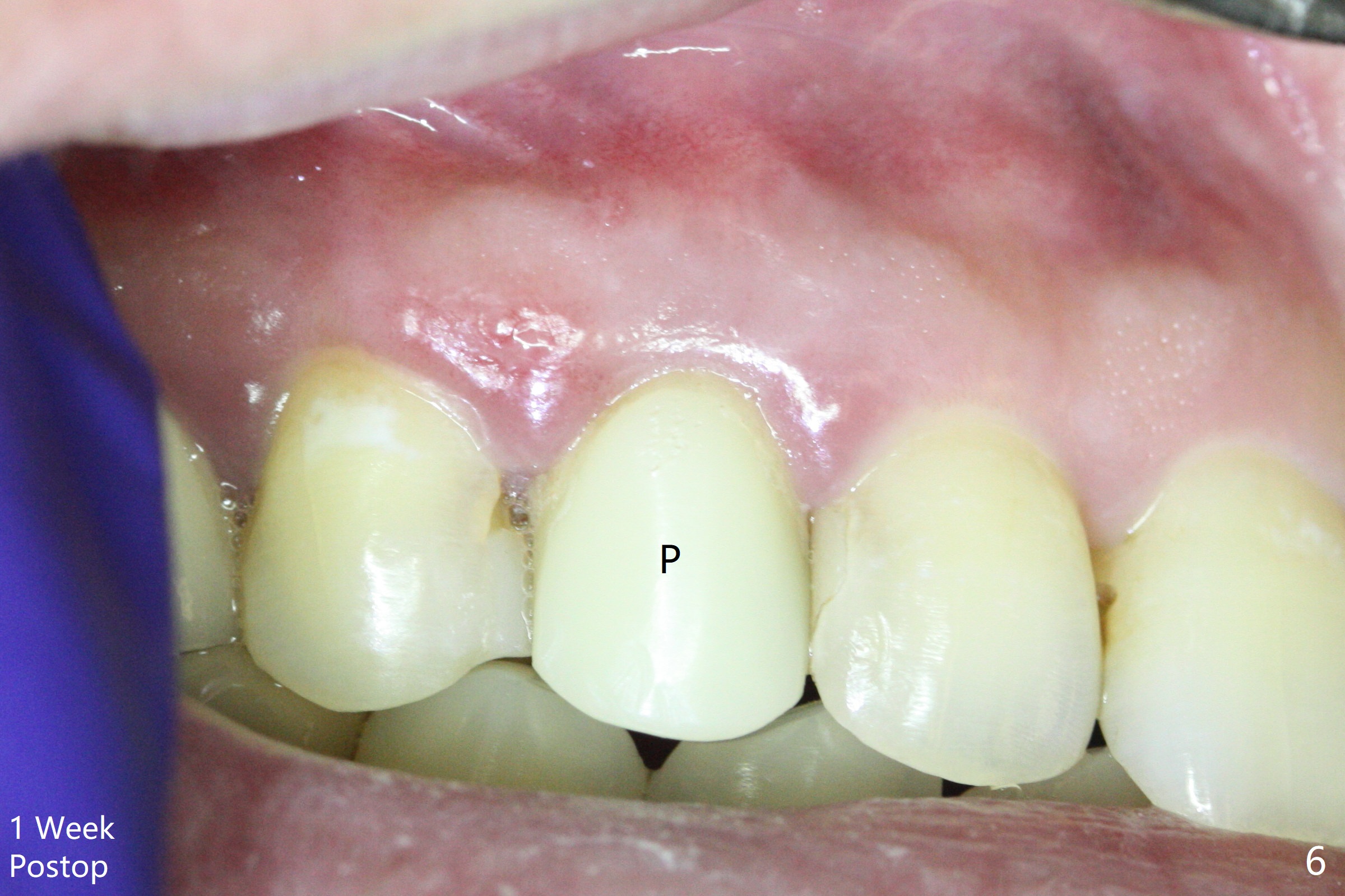
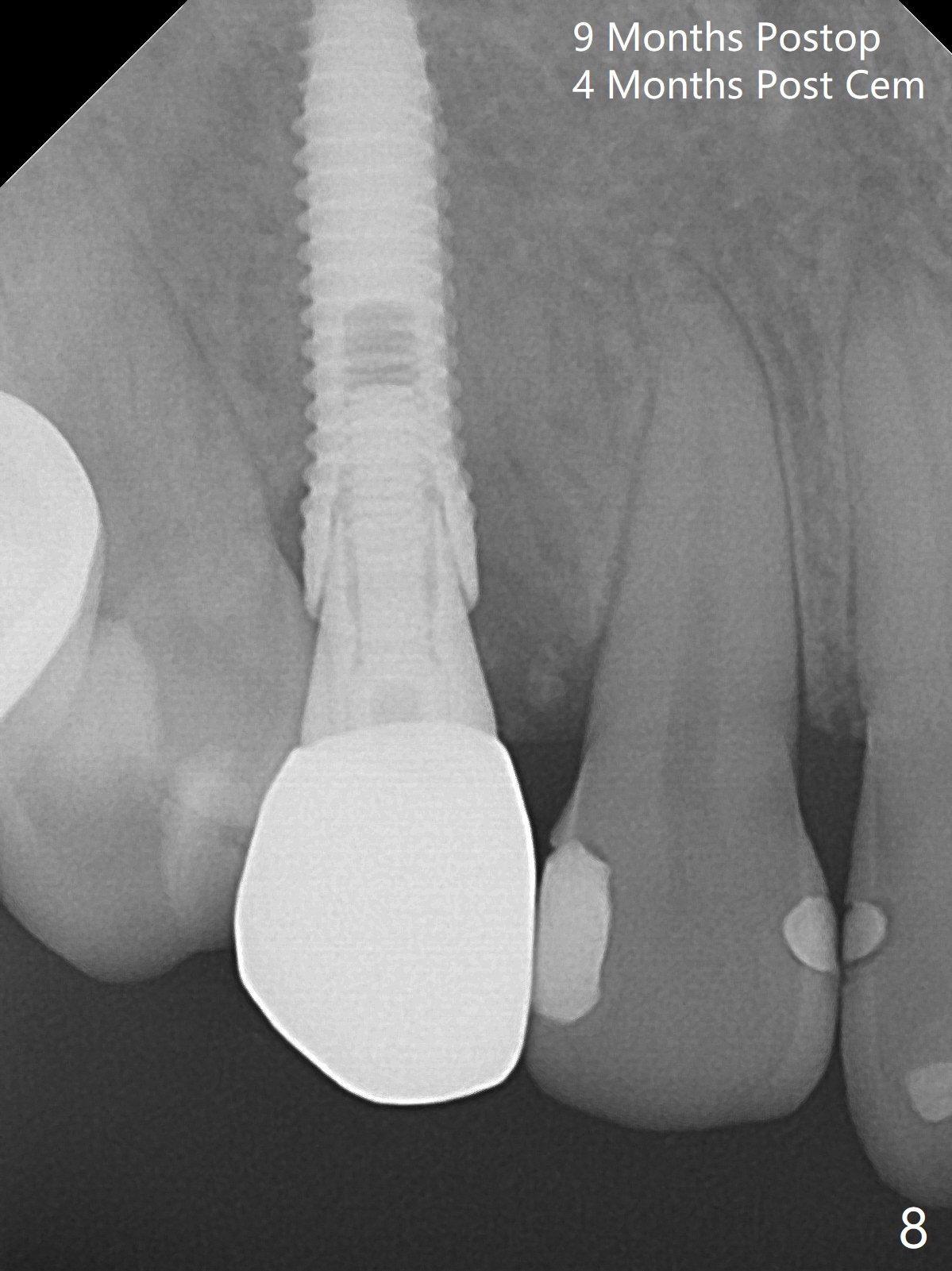
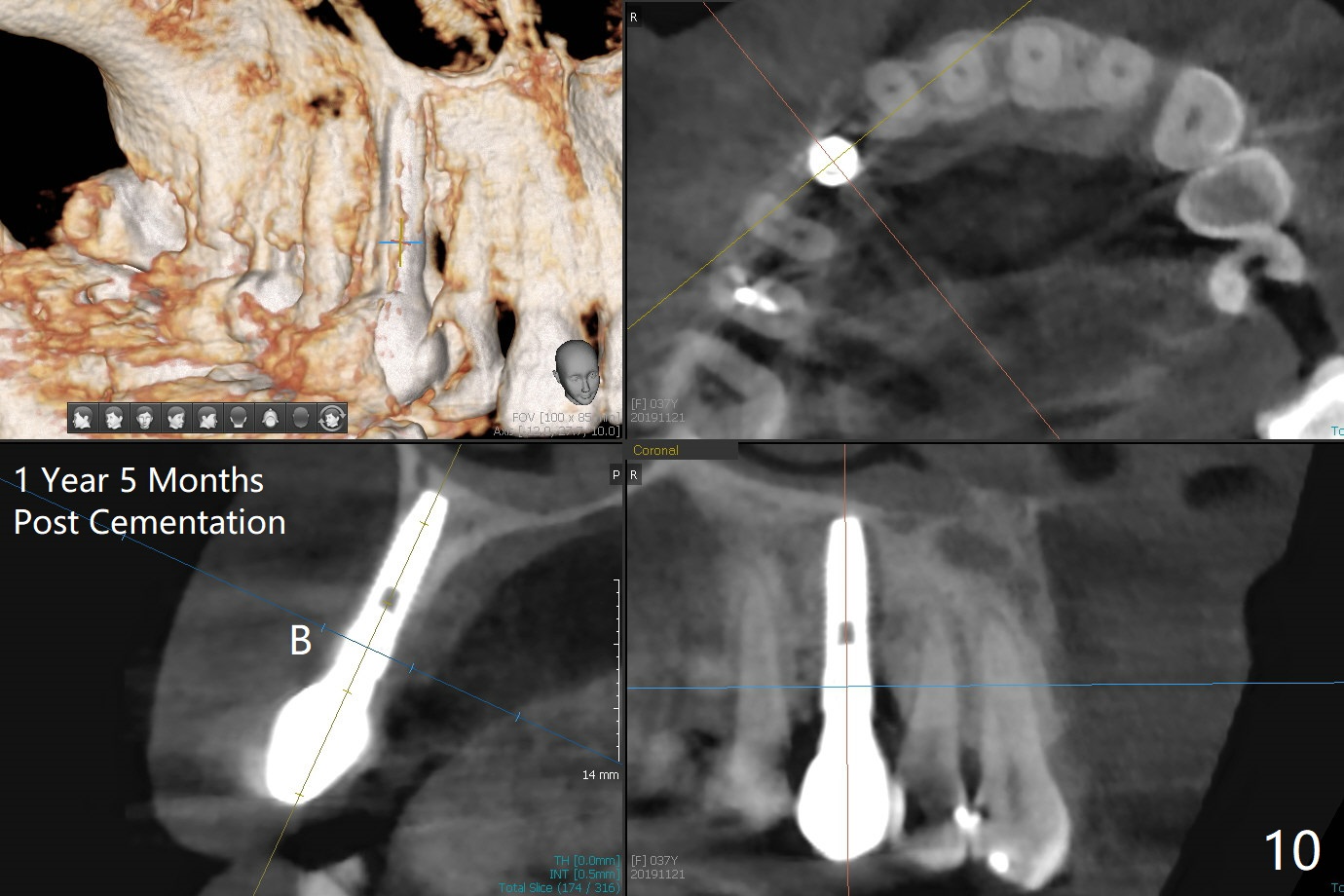
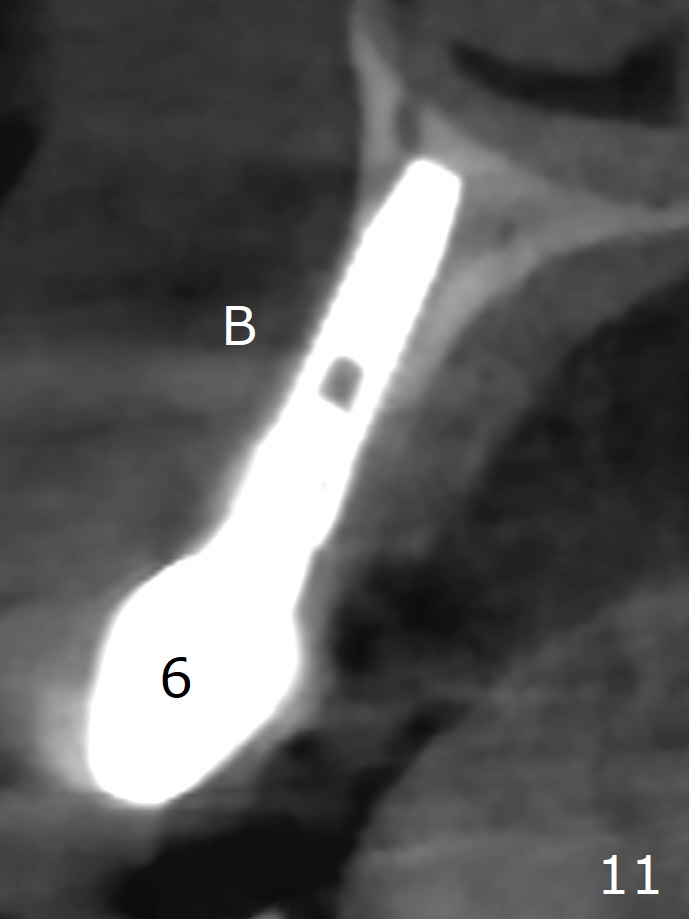
When the tooth #6 with loose crown and post (Fig.1) is extracted, there is no granulation tissue in the socket with the thin intact buccal plate. As planned, osteotomy is initiated in the mesio-palatal slope of the socket (Fig.2 red dashed line). After osteotomy for 3x20 mm (gingival level), a 3.8x15 mm dummy implant is placed partially (Fig.3 D). A final implant with the same dimension is placed with > 50 Ncm (Fig.4). Before and after placement of a 4.5x5(3) mm abutment, Vera graft is placed in the remaining socket space (mainly buccal, Fig.5 *). As routine, an immediate provisional is fabricated with occlusal clearance. The gingiva looks healthy around the provisional 1 week postop (Fig.6 P). Adjust and polish the mesioocclusal composite at #5 if necessary before impression. The bone graft appears to remain in place 4.5 months postop (Fig.7). A bevel buccal subgingival margin is placed prior to impression. The bone density around the coronal portion of the implant increases 9 months postop (4 months post cementation, Fig.8). There is no gingival erythema or edema around the implant crown at #6 ten months post cementation (Fig.6, as compared to preop condition and that of the neighboring crown (*)). Both the buccal and palatal plates are thin or absent 1 year 5 months post cementation (Fig.10,11, as compared to Fig.12 for the tooth #11 (thin buccal bone)). Socket shield should be done with a smaller implant.
Return to Upper Canine Immediate Implant, Armaments 18 Xin Wei, DDS, PhD, MS 1st edition 01/26/2018, last revision 04/13/2020