
|
|
|
|
|
|
|
|
Buccal Deviation M
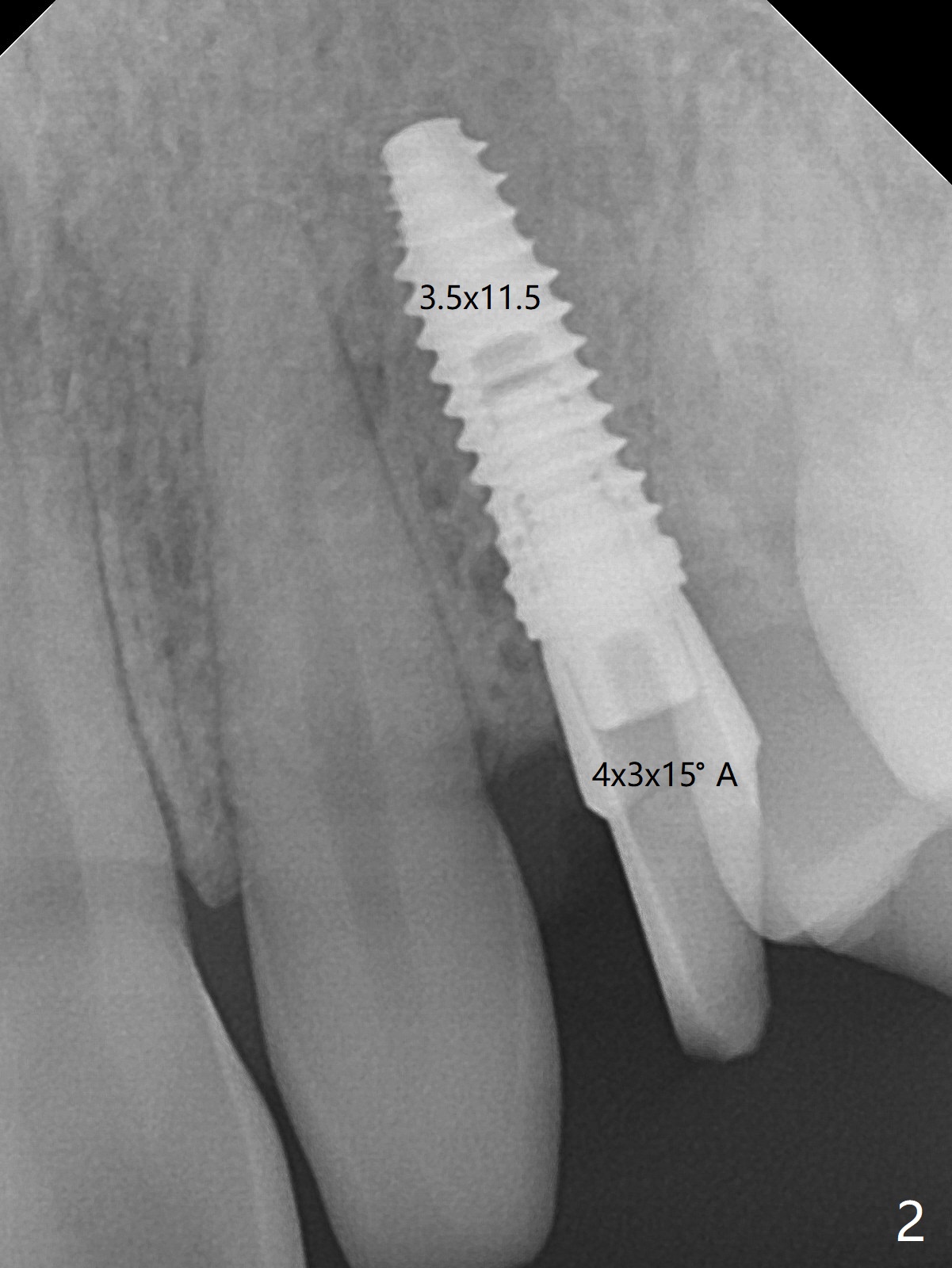
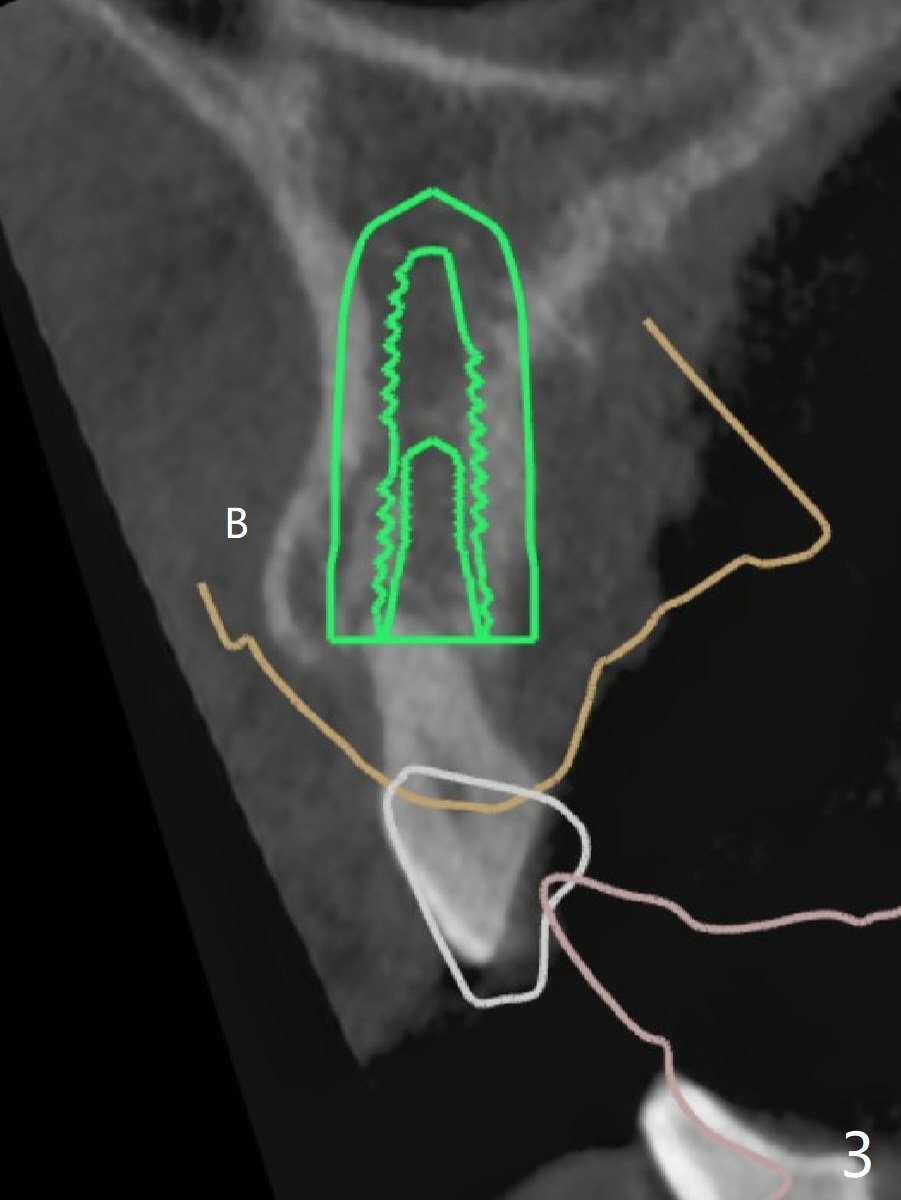
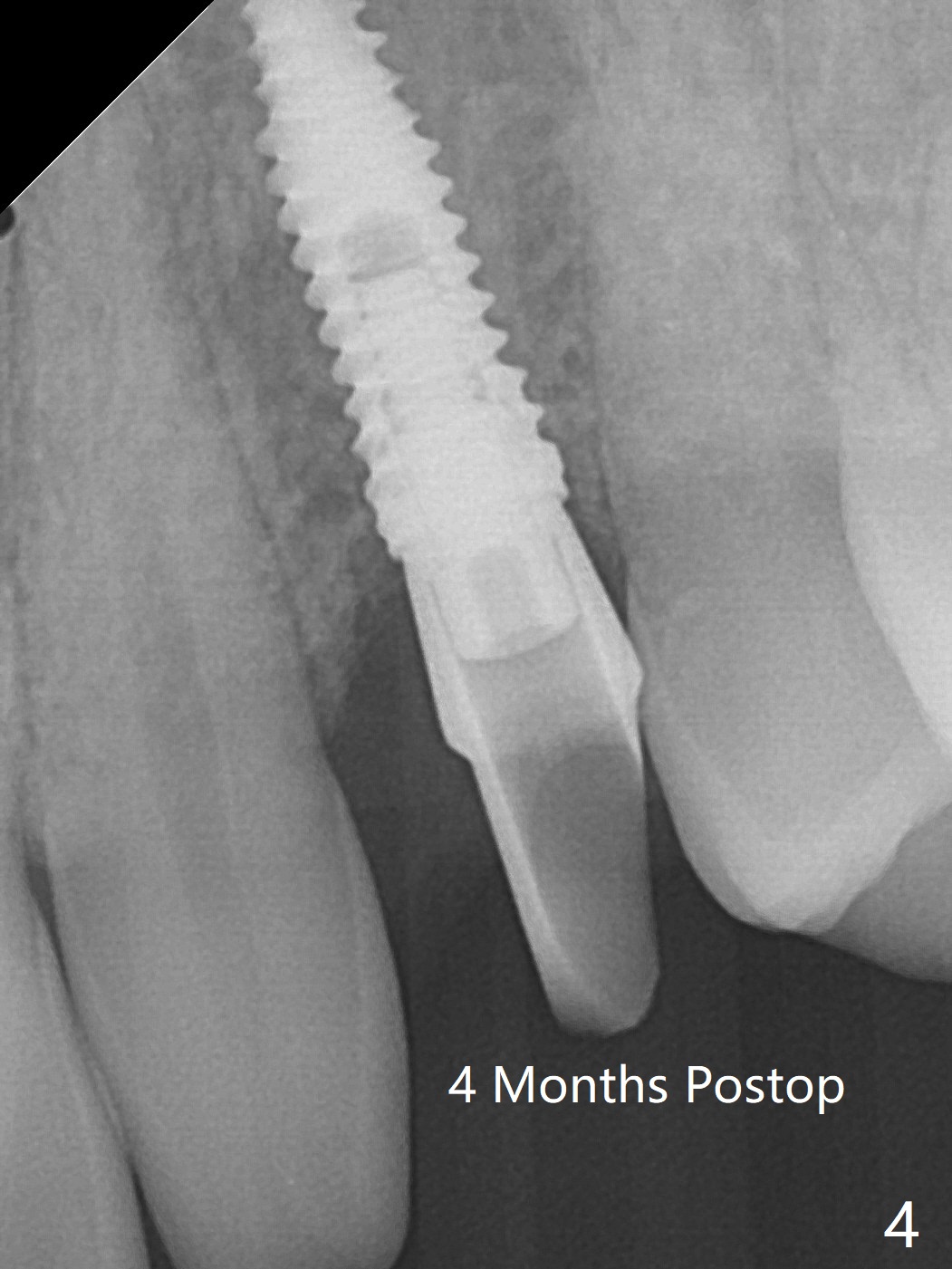
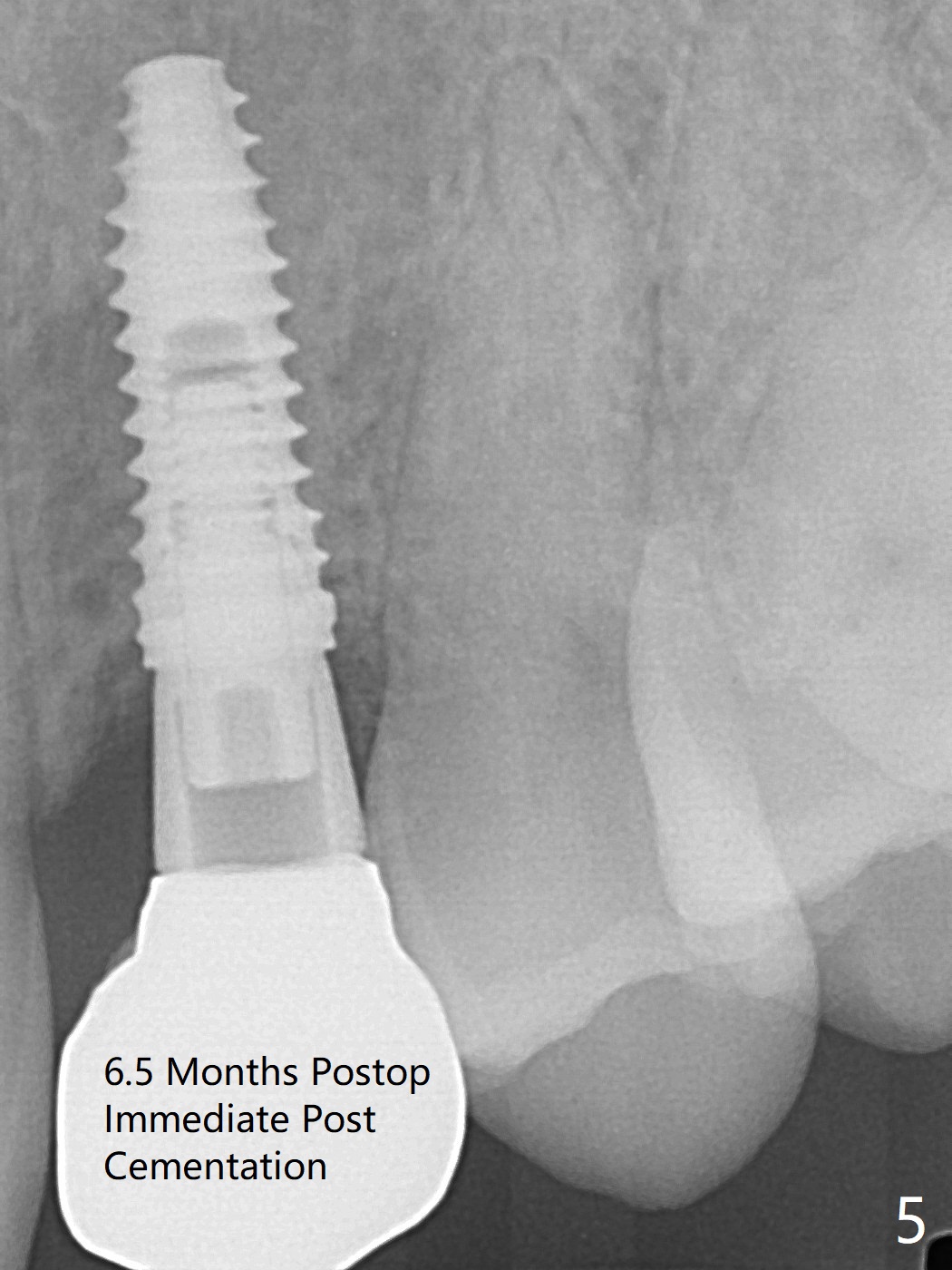
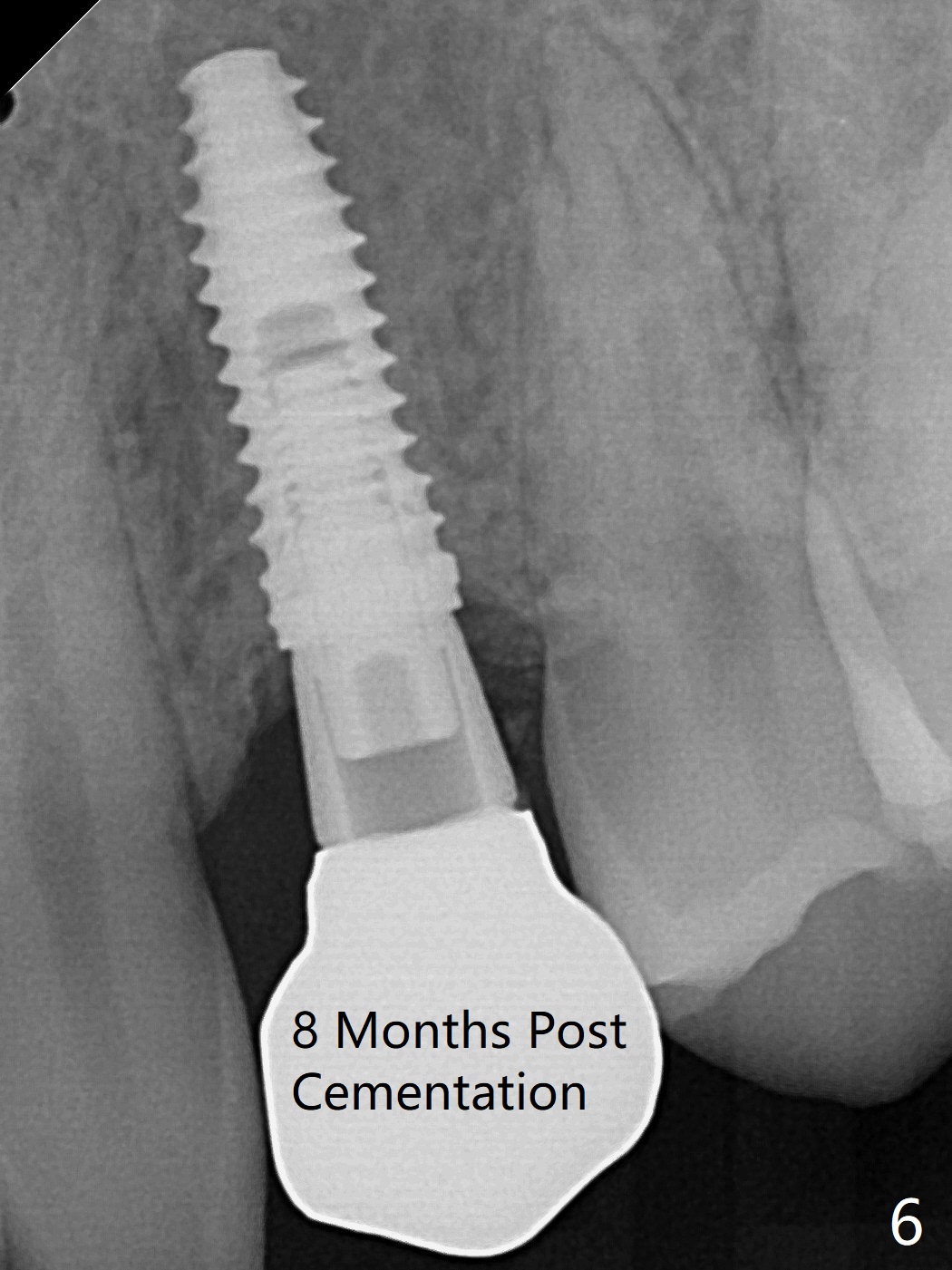
When the guide with 10.5 mm offset is seated at #11 after extraction, it looks buccal. Pointed drill creates an entry point in the mesial portion of the socket. PA, taken following 2.2x11.5 mm drill, shows acceptable mesiodistal trajectory (Fig.1). When a 3.5x11.5 mm implant is placed, it is difficult to withdraw the driver from the metal tube (Fig.1 *). There is no buccal gap with plenty of the lingual gap. A 4x3 mm x15 degree A-type angled abutment is placed (Fig.2). It appears that the dense palatal plate deviates the osteotomy and implant placement (as compared to the design, Fig.3). In fact osteotomy should have been prepared until 4 mm in diameter before increase in depth with 2.2 and 3 mm drills to eliminate buccal deviation. The ideal drill sequence would be point drill, 2.2x8.5 mm drill, 3x8.5, 3.5x8.5, 2.2x10, 2.2x11.5, PA to confirm trajectory, 3x10, 3x11.5 and 3x13. Torque associated with implant placement is pure, not derived from friction between the driver and the metal tube. There is mesial crestal bone loss 4 months postop (Fig.4, as compared to immediate postop in Fig.2 (*)). Crestal bone loss does not get worse between 4 and 6.5 months postop (Fig.4,5). The bone density seems to increase 8 months post cementation (Fig.6). With improved oral hygiene, the gingiva around the implant is healthy 1 year post cementation when oral scanning and CT are done for #20 implant.
Return to
Upper
Canine Immediate Implant,
Trajectory II
Xin Wei, DDS, PhD, MS 1st edition
12/19/2019, last revision
07/31/2021