


|
|
|
|
|
|
|
|
|
|
||
Implant Bisects Bone Plate Discrepancy
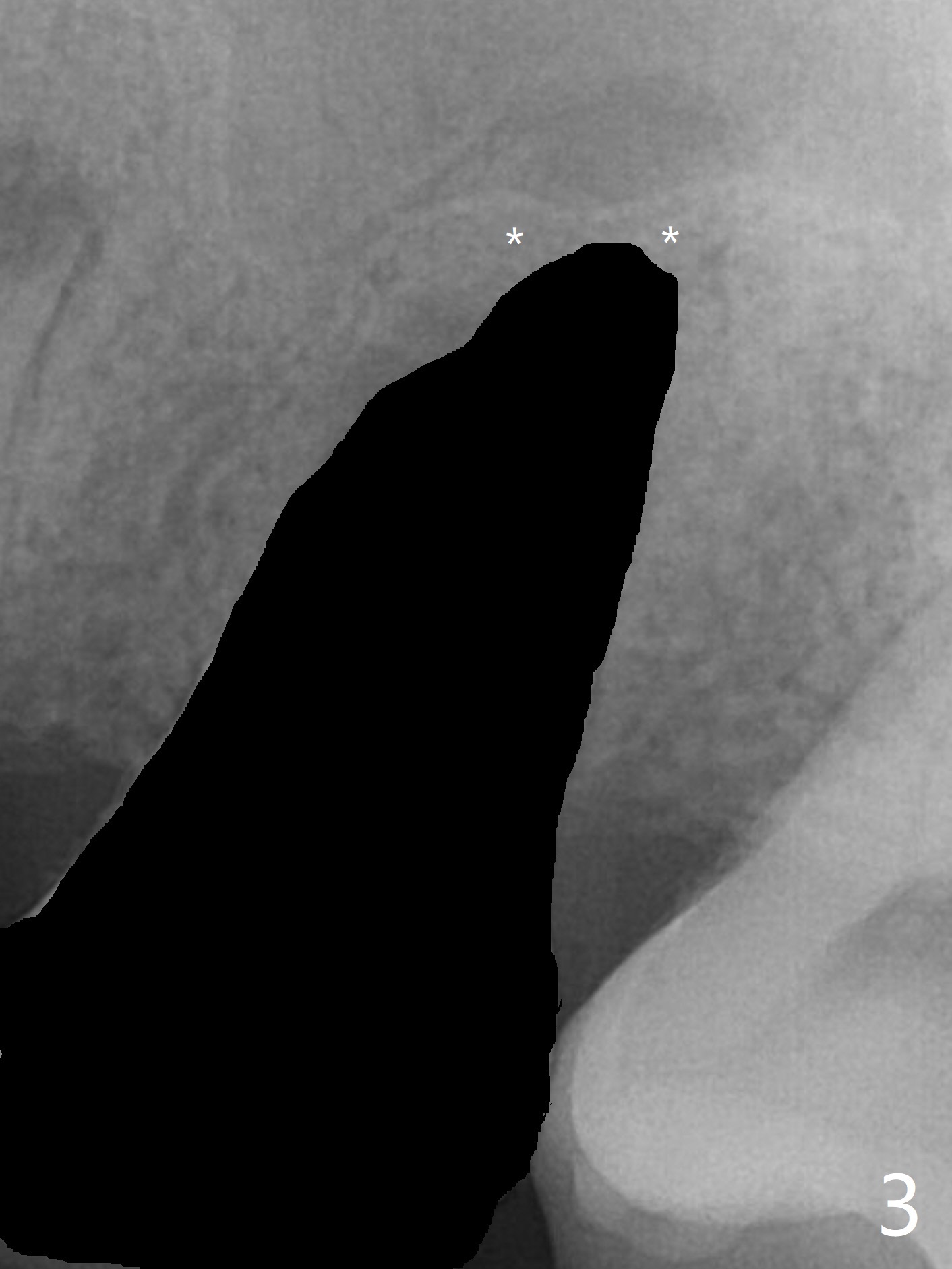
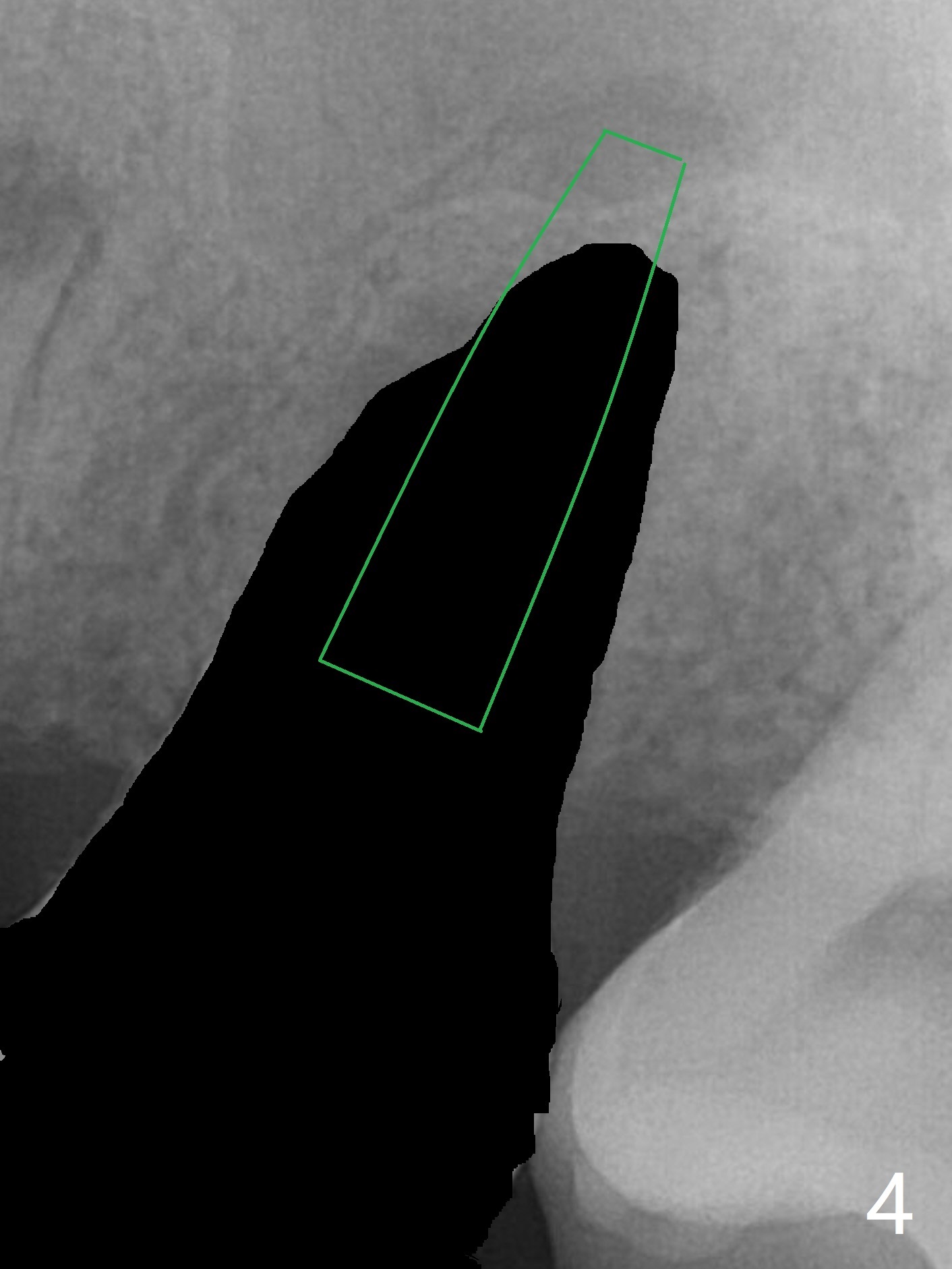
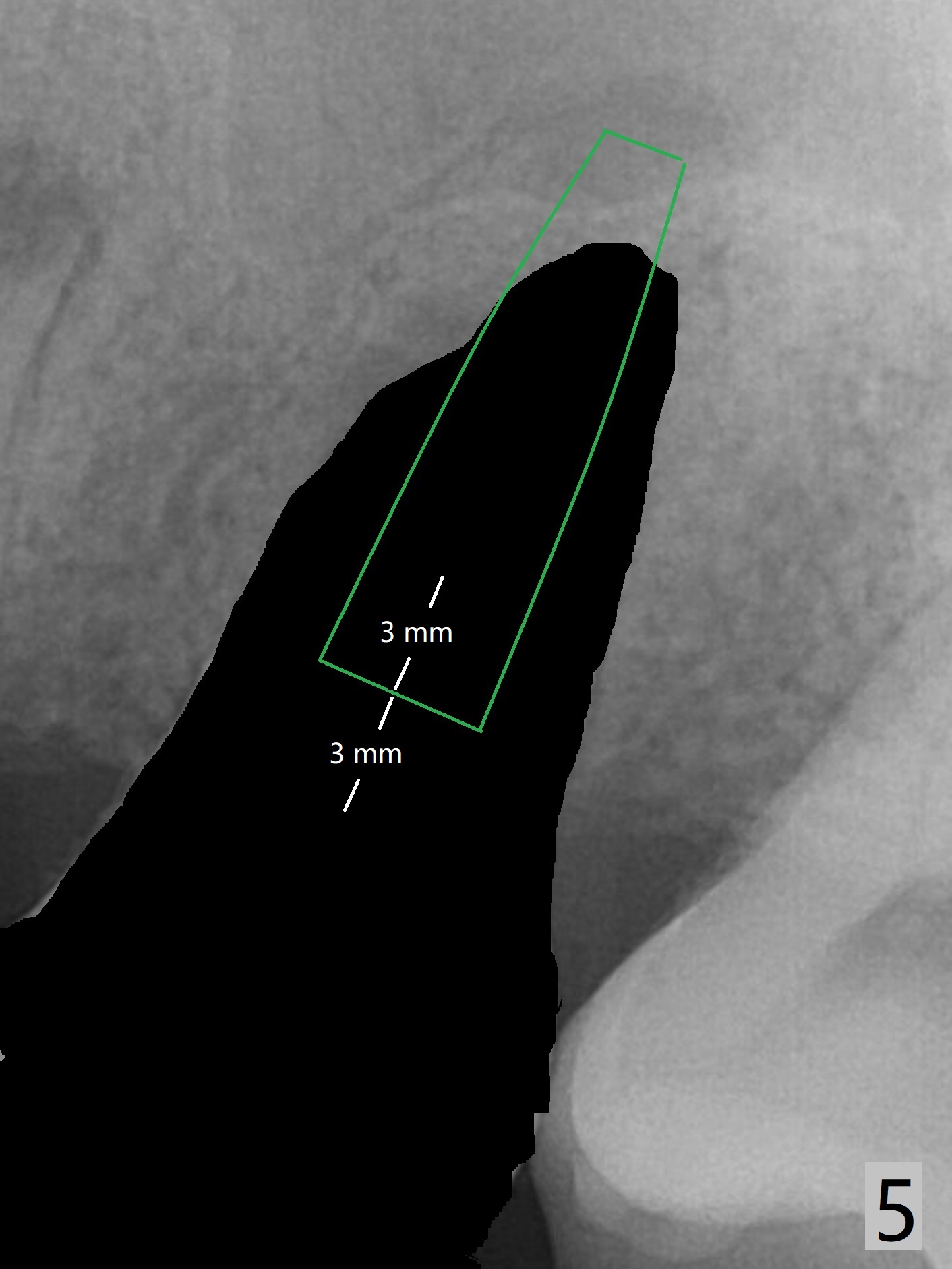
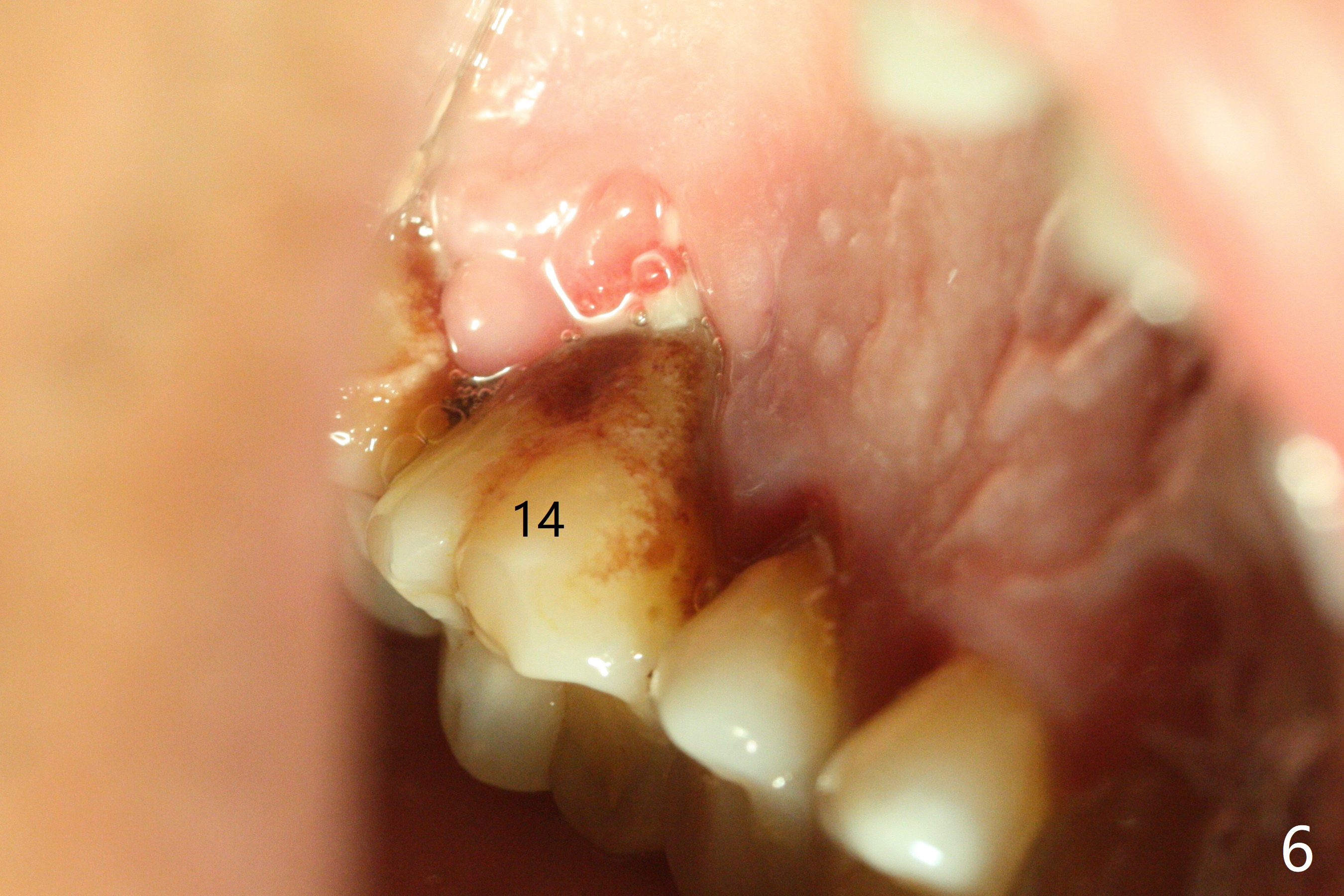
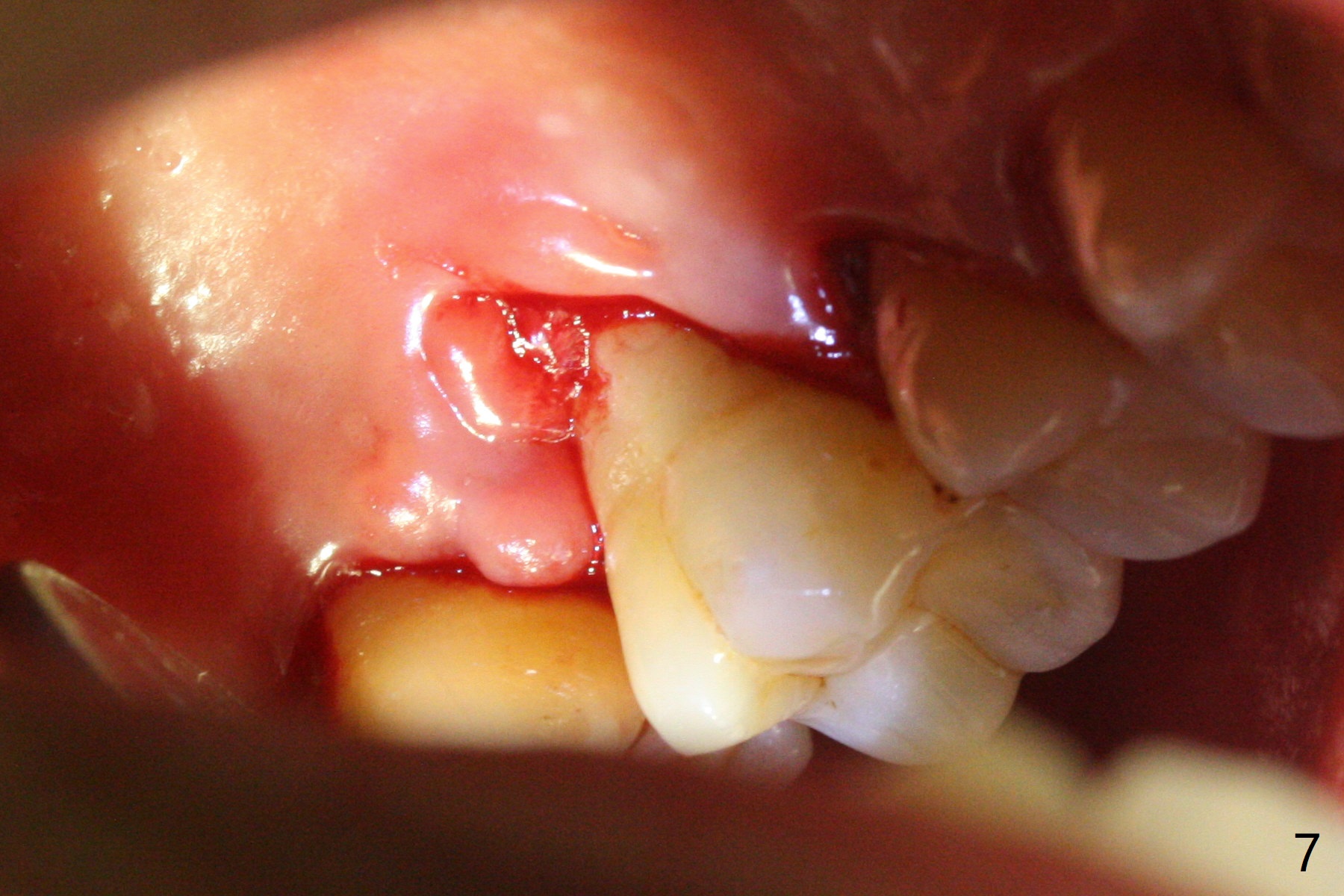
A 45-year-old man has chronic generalized moderate localized severe periodontitis; gingival recession is severe lingual of the tooth #14 with mobility II (Fig.1). The low bone density outline (Fig.1 white dashed line) is larger than the roots, suggesting lingual bone loss/low lingual crest. Although the bone height seems to be 11 mm (Fig.2), the bone responsible for primary stability of an implant will be apical (Fig.3 *,4). The implant platform will be ~3 mm subcrestal buccal, while ~3 mm supragingival lingual (Fig.5). The diameter of the implant will not be too large, 4.5 mm (dummy). There will be not biologic width issue. The large perimplant gap will be closed with sticky bone. Severe palatal gingival recession is shown pre- (Fig.6) and post- (Fig.7) SRP. #30 Gutta Percha inserted palatal reaches the highest point of the low bone density lesion (Fig.8). Pulpal test and CT will determine that endodontic treatment can regrow bone or that socket preservation is needed with Cytoplast.
Return to Upper Molar Immediate Implant, Prevent Molar Periimplantitis (Protocols, Table) Trajectory II Metronidazole Shield Xin Wei, DDS, PhD, MS 1st edition 11/03/2019, last revision 11/04/2019