%20ball.jpg)
|
|
|
|
|
|
|
|
|
|
Why Not Guided Surgery?
M
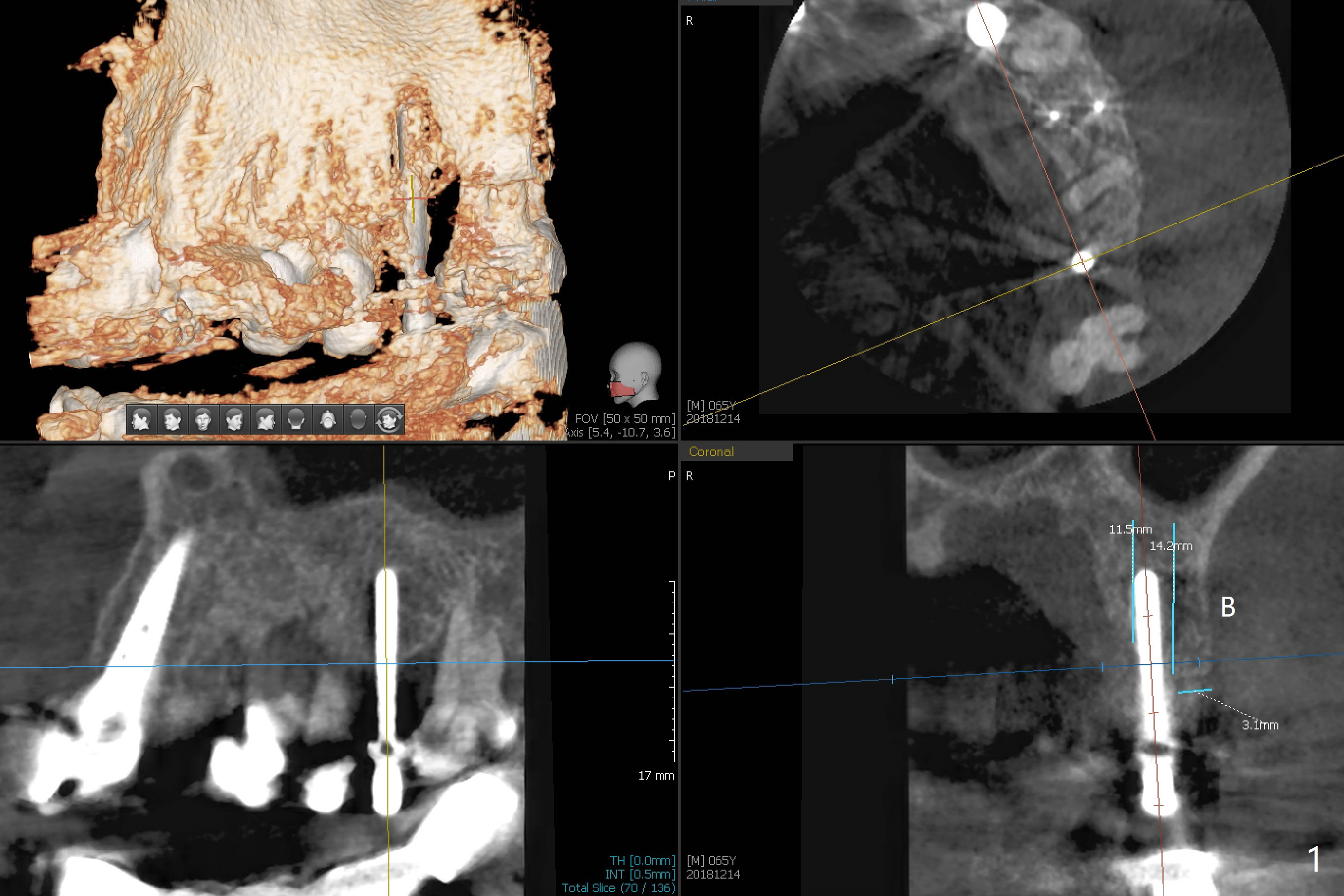
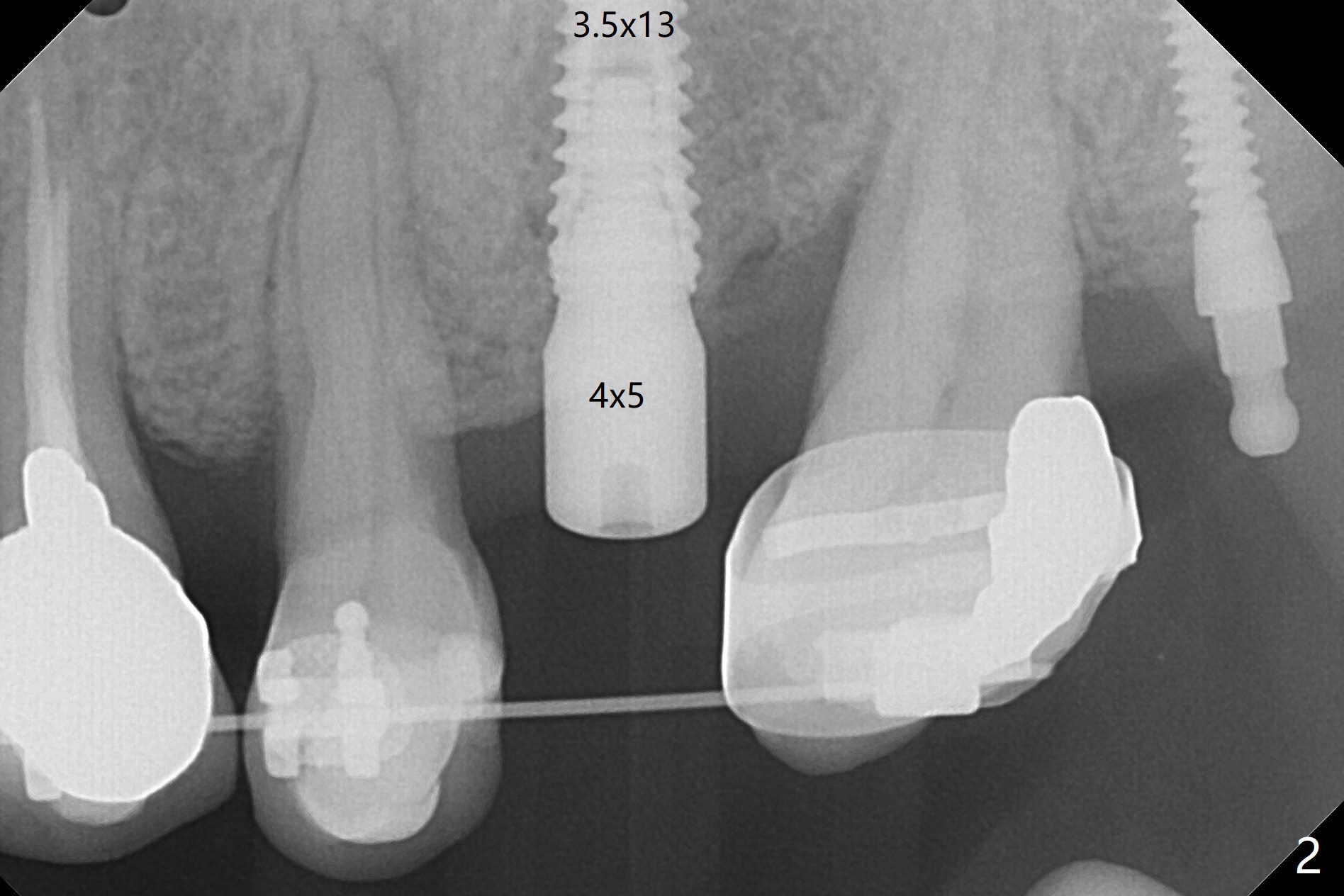
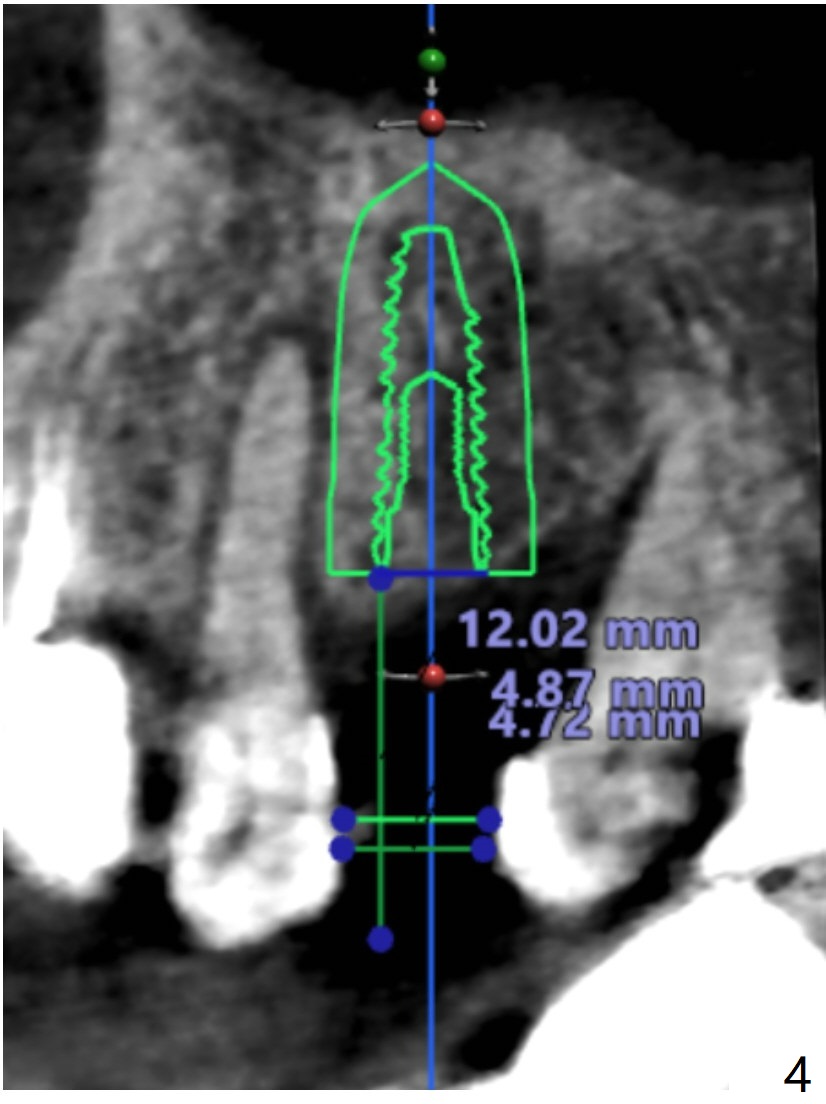
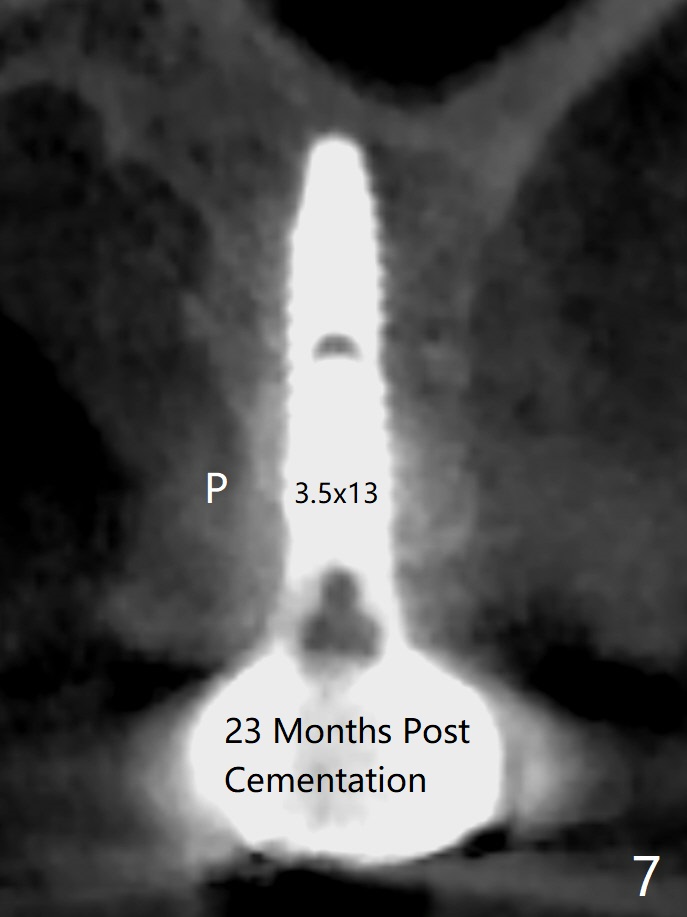
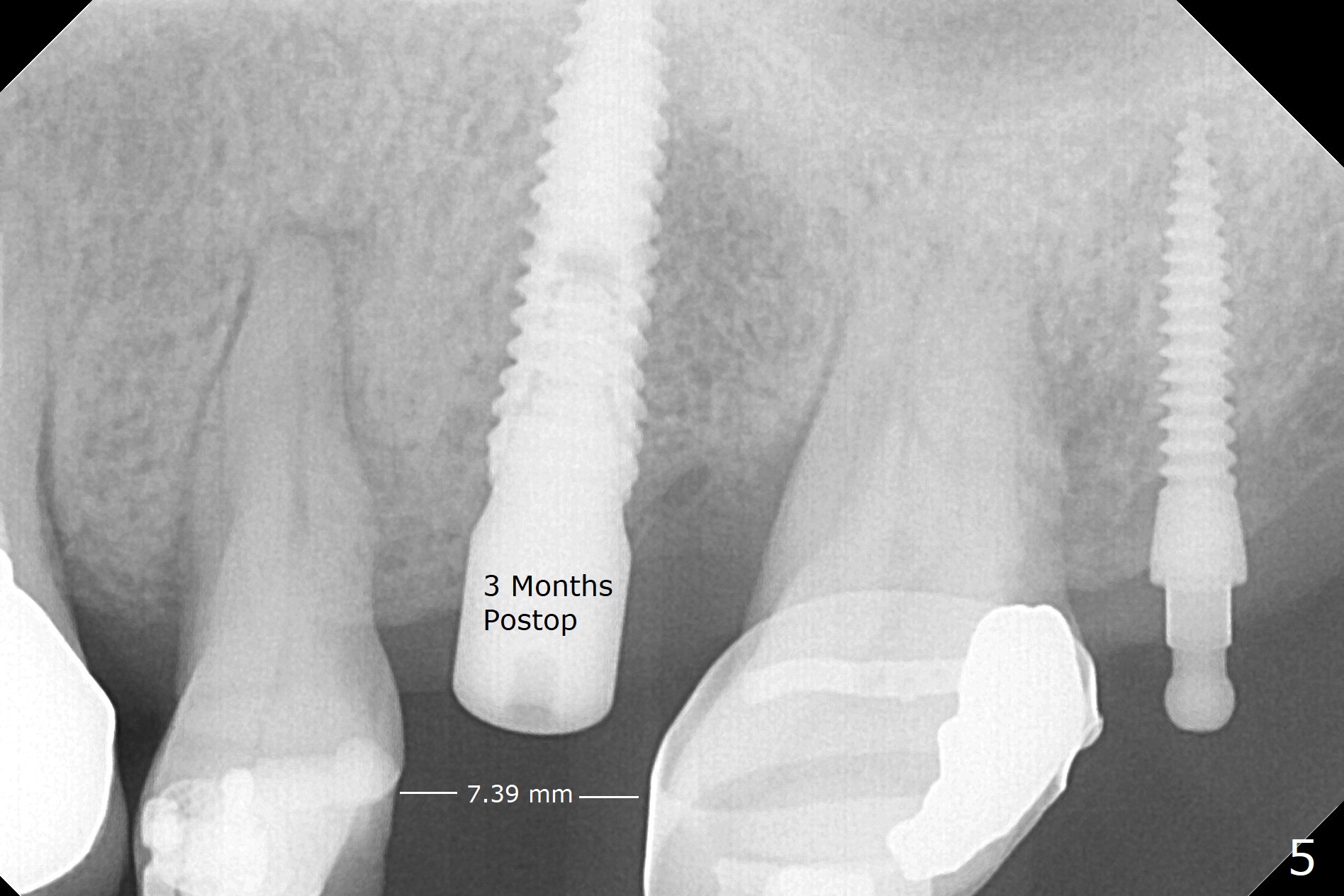
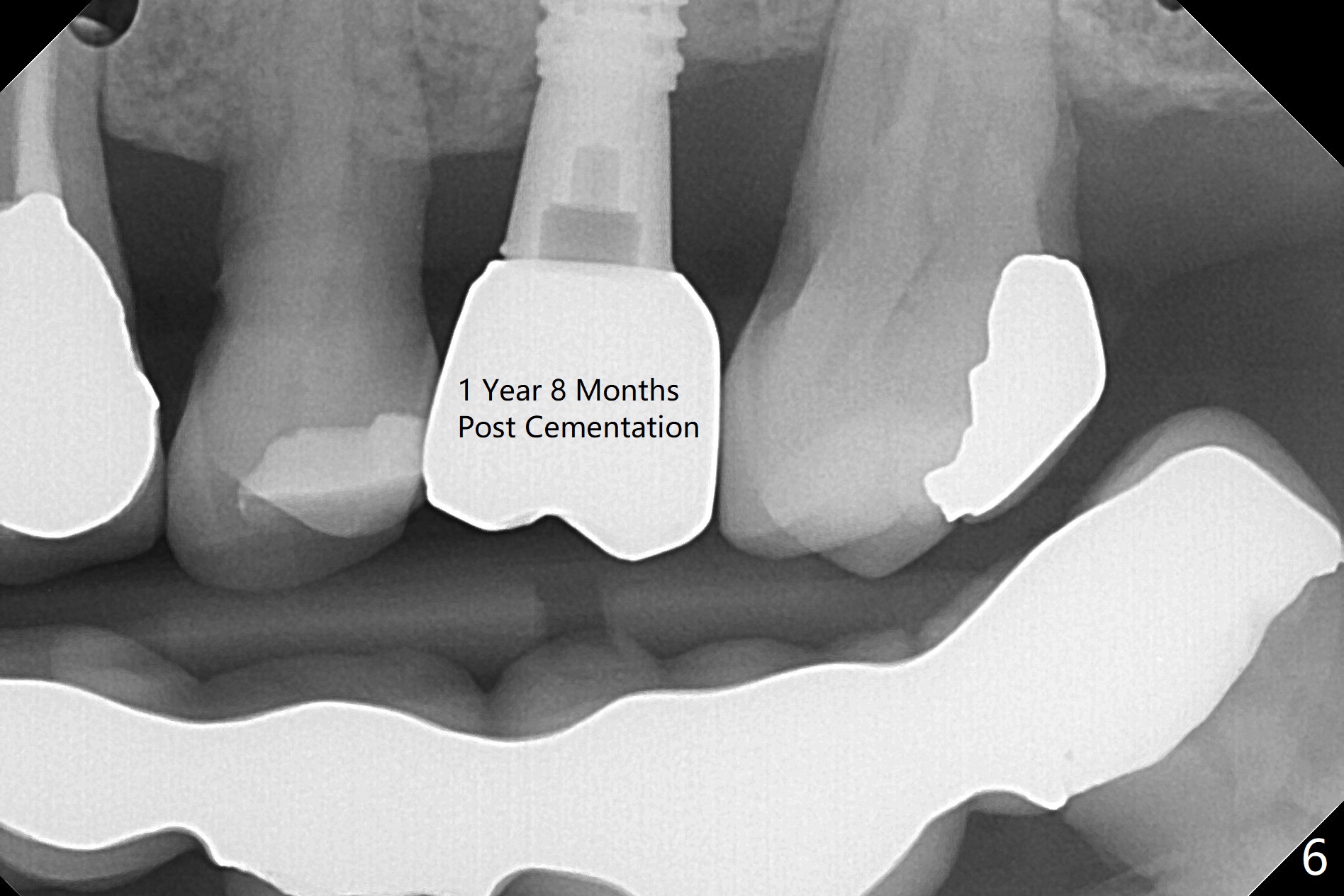
Eight-month limited ortho including use of a 1-piece implant (Fig.3 P (ball type)) as a distal anchor increases the mesiodistal space of #14 from <4 mm to 6 mm (near premolar width). Guided surgery is not indicated because of presence of brackets and band and the narrow space. Also due to the latter, incision is difficult to make. In stead a 3.5 mm tissue punch is applied. After 2.2 mm drill, a parallel pin is placed; it appears that the initial osteotomy is palatal (Fig.1). Lindamann bur is adopted to move the osteotomy buccal. The last drill (3 mm for 3.5 mm implant) has no resistance when it enters the buccalized osteotomy. A longer implant than designed is placed (3.5x13 mm, Fig.2,3, close to the sinus floor (dashed yellow line) with 50 Ncm. When the implant osteointegrates, it will be used a mesial anchor to distalize the 2nd molar.
Return to Upper Molar Immediate Implant Trajectory 矫正,糖尿病,种植水平 右上桥基牙根裂 植牙,导板与正畸 DIO 2,3 Xin Wei, DDS, PhD, MS 1st edition 12/14/2018, last revision 04/19/2021