


|
|
|
|
|
|
|
|
|
|
|
Implant Failure Due to Shallow Placement M
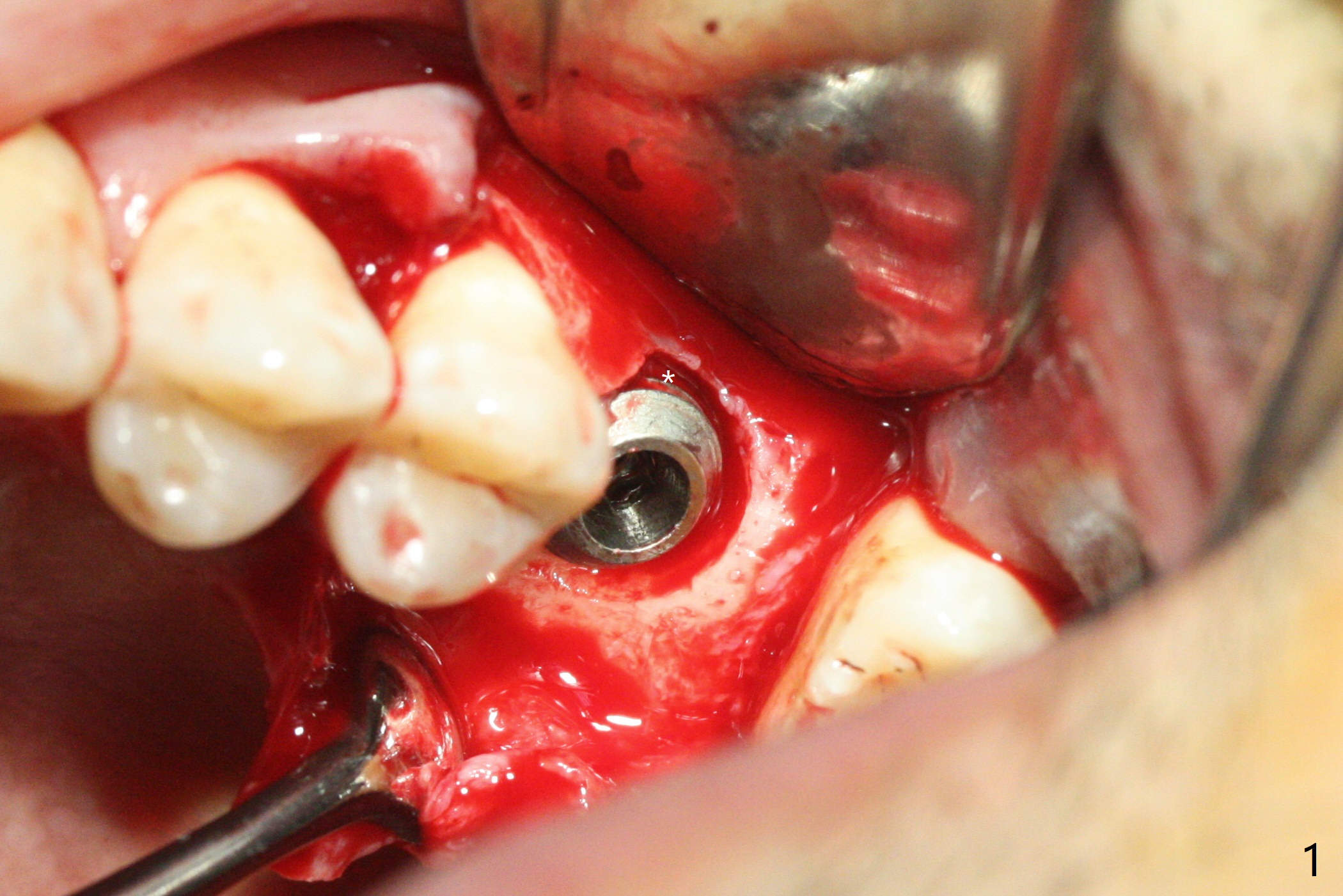
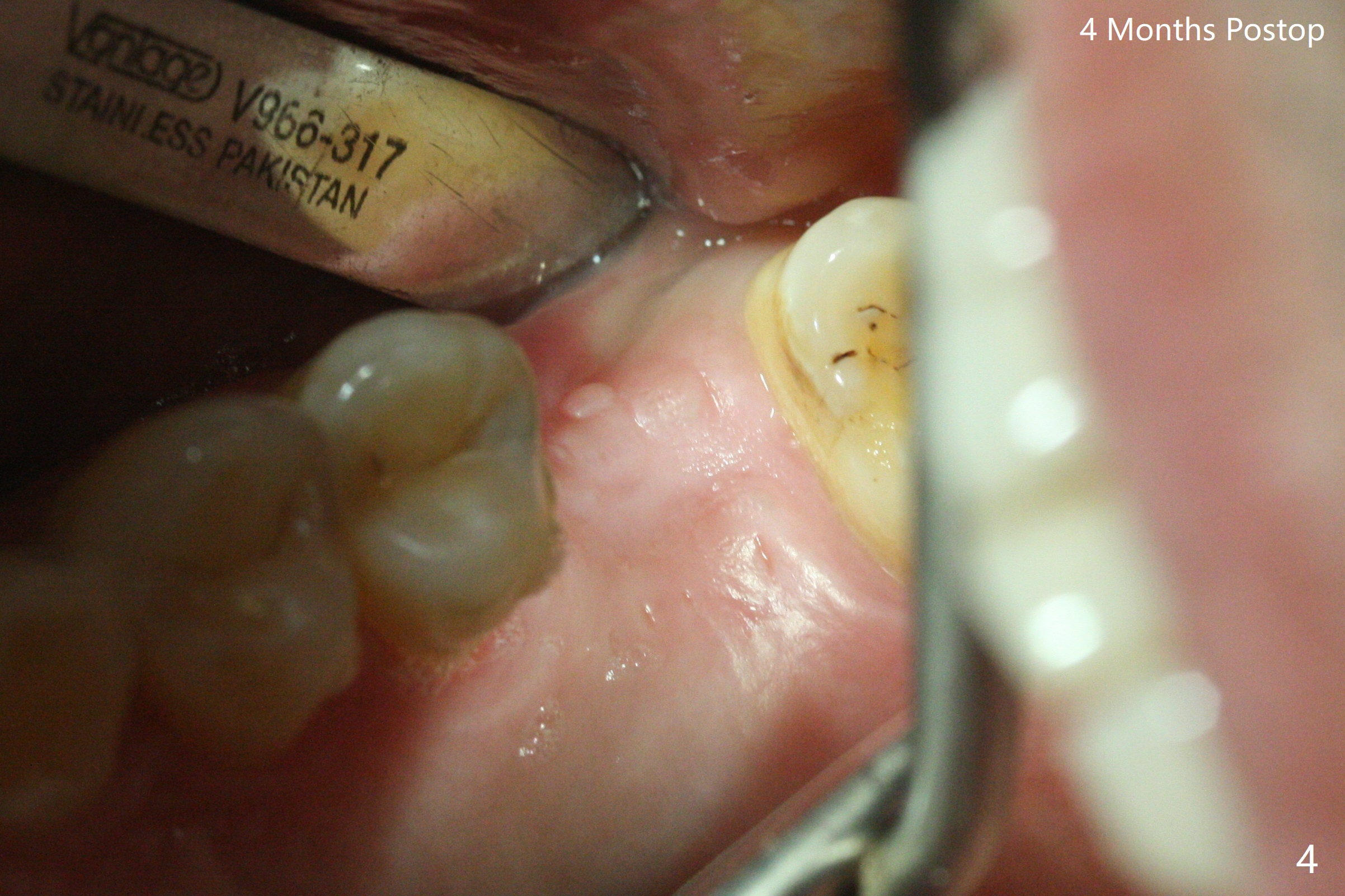
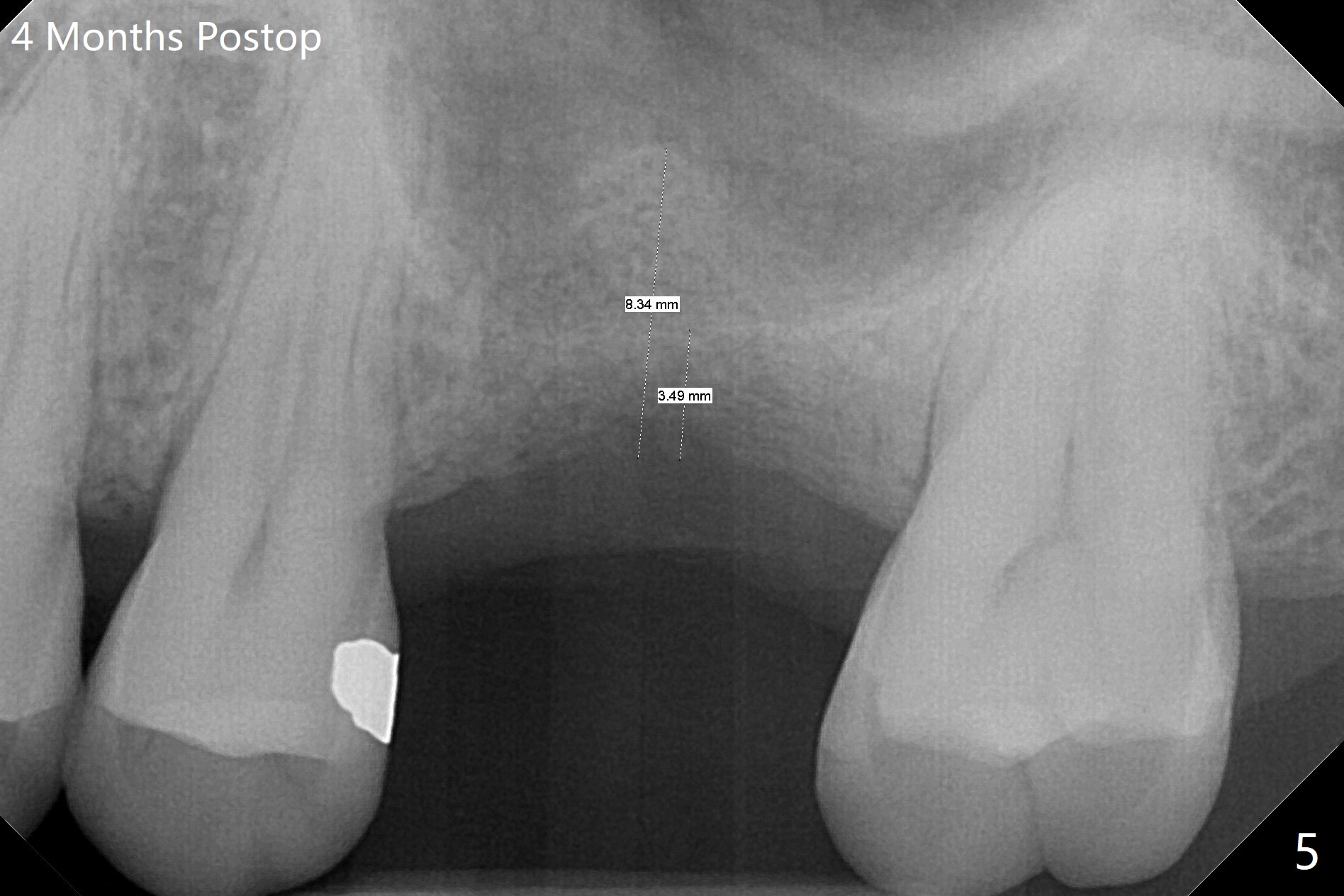
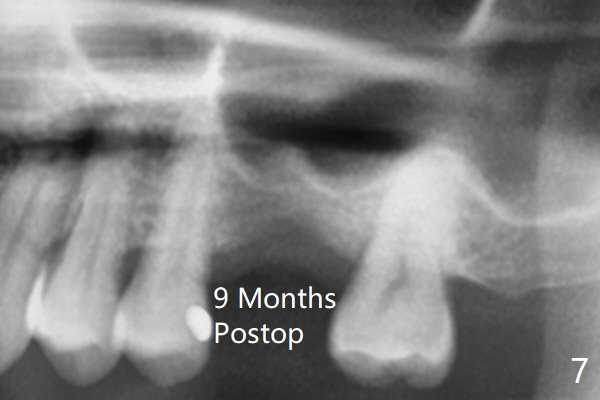
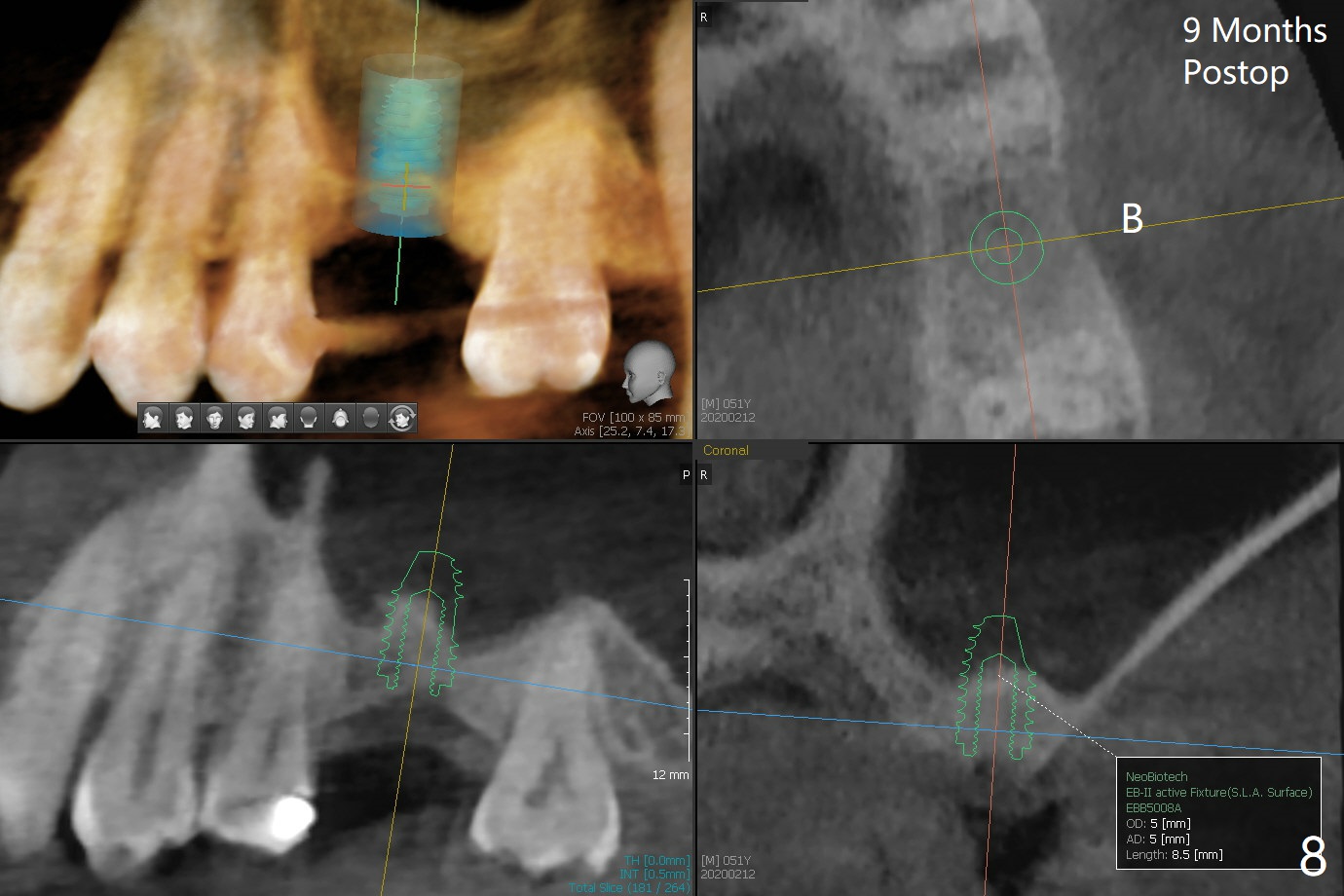
When the crown and abutment at #14 are removed, the implant is found to be shallowly placed. Upon incision, the implant threads are exposed circumferentially and coronal to the buccal crest (Fig.1 *). It seems to be difficult to expect bone regeneration post bone graft. The implant (6.4x6 mm) is removed with a 7/8 mm trephine bur, followed by sticky allograft (Fig.2 *), PRF membrane and 6-month membrane. In spite of the setback, the bone height increases from 3.9 mm to 11 mm due to sinus lift associated with the previous implant placement (Fig.2 L). The depth of the 2nd placement will be controlled by surgical guide. When the periodontal dressing dislodges 11 days postop, the 6-month membrane is lost as well as part of the bone graft. If there is remaining apical native bone, an immediate implant should be placed so that bone graft can be kept in place more securely with an immediate abutment and provisional! The seemingly conservative approach is actually not safe. The wound heals 1 month postop (following dislodgement of the 2nd periodontal dressing, Fig.3). Three months later, consider using bone expanders to do sinus lift and place a SM implant subcrestal. Take PA after 1st expander to the depth. The wound heals 4 months postop (Fig.4), but the bone height (Fig.5) and width (Fig.6) decreases. The latter continues to decrease 9 months postop (Fig.7,8), but bone density is high, average 1360 units. Preparation includes guide, incision, sinus lift, implant placement (possibly tissue-level (9) or FC if the sinus membrane perforates), bone graft, and suture.
Return to Upper Molar Immediate Implant, Trajectory Surgery
Xin Wei, DDS, PhD, MS 1st edition 05/21/2019, last revision 06/05/2020