
,%207%20m%20postop.jpg)
|
|
|
|
|
|
|
|
|
|
Thickened Sinus Membrane Helps Lift M
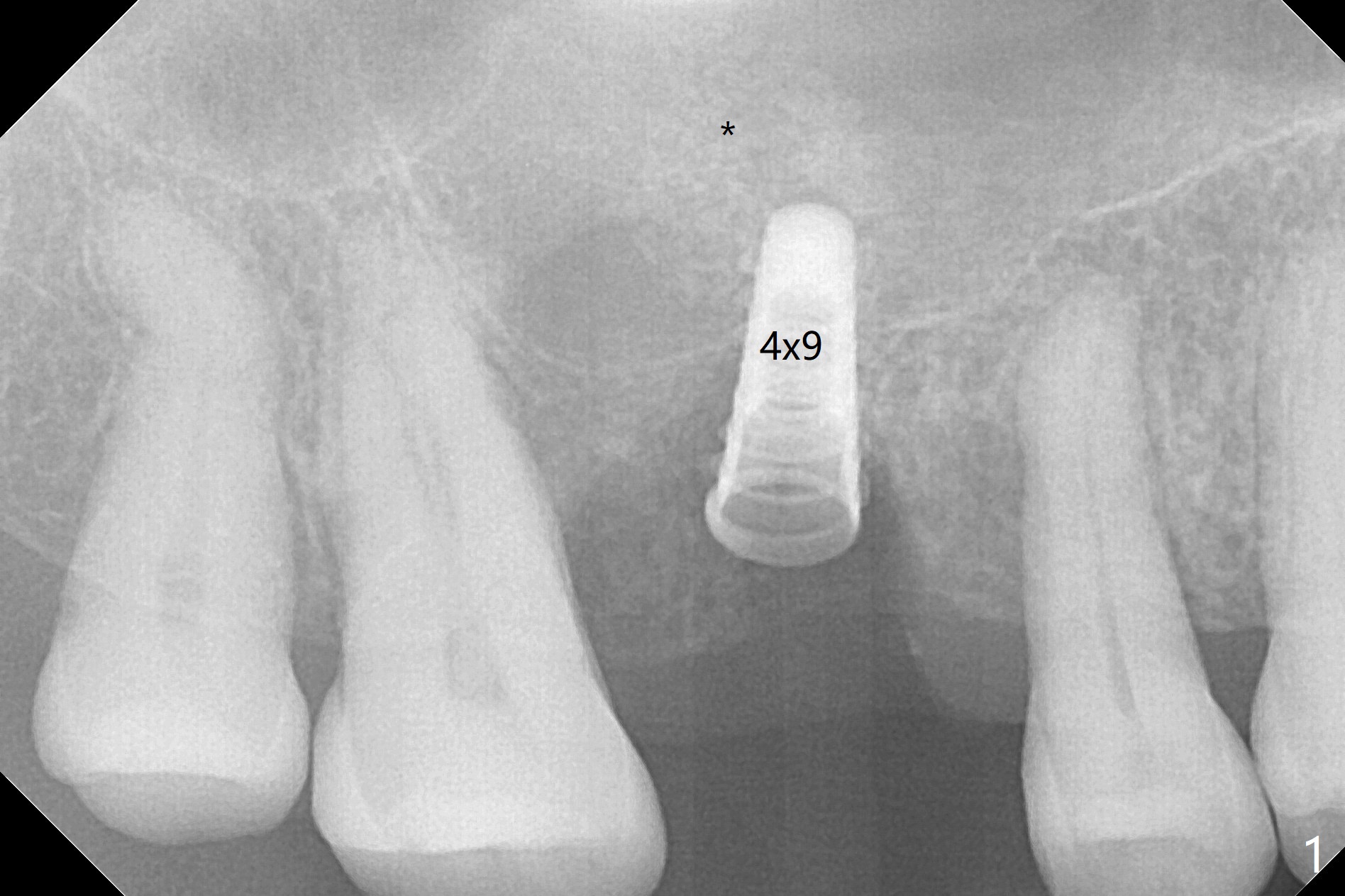
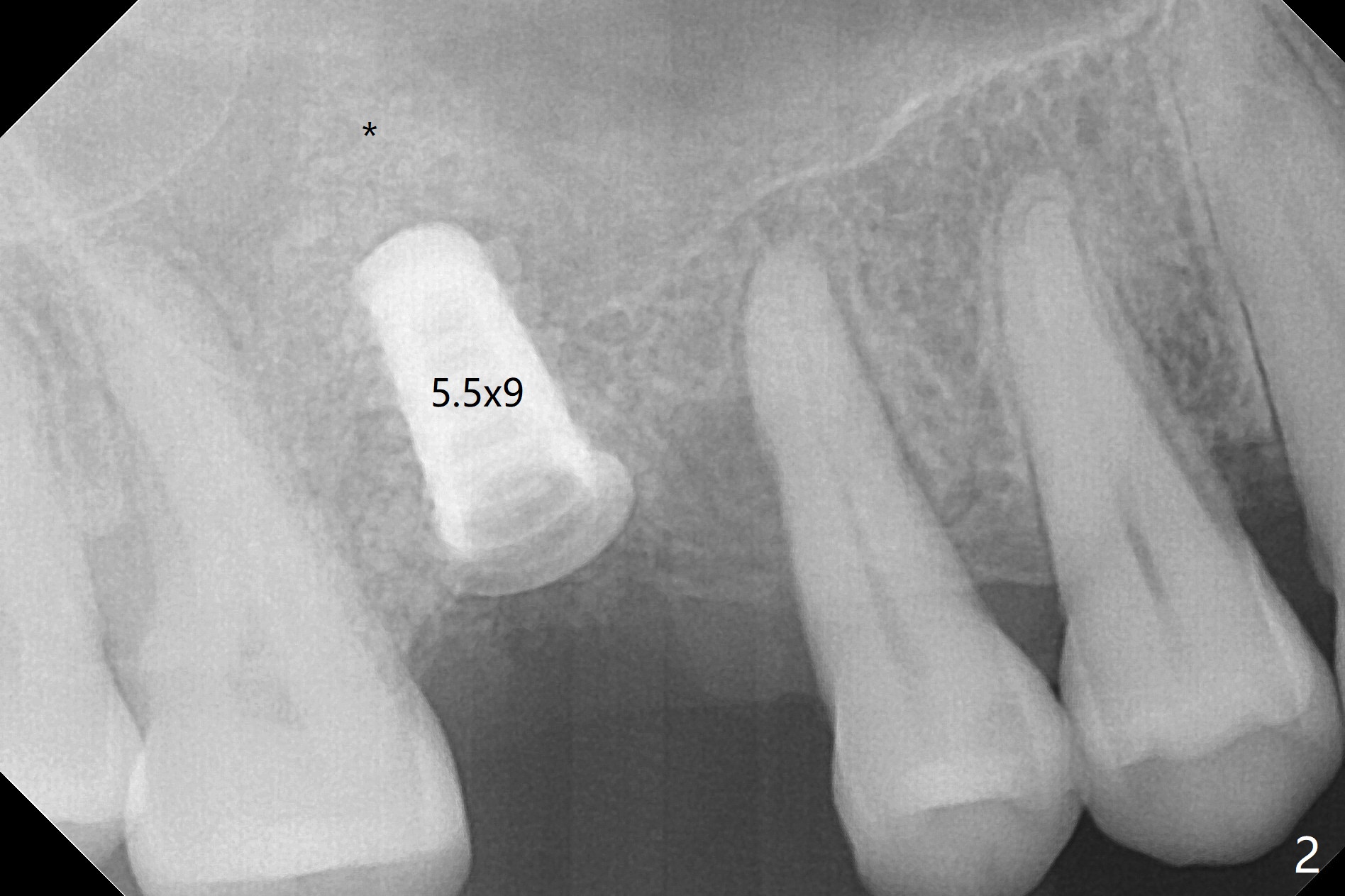
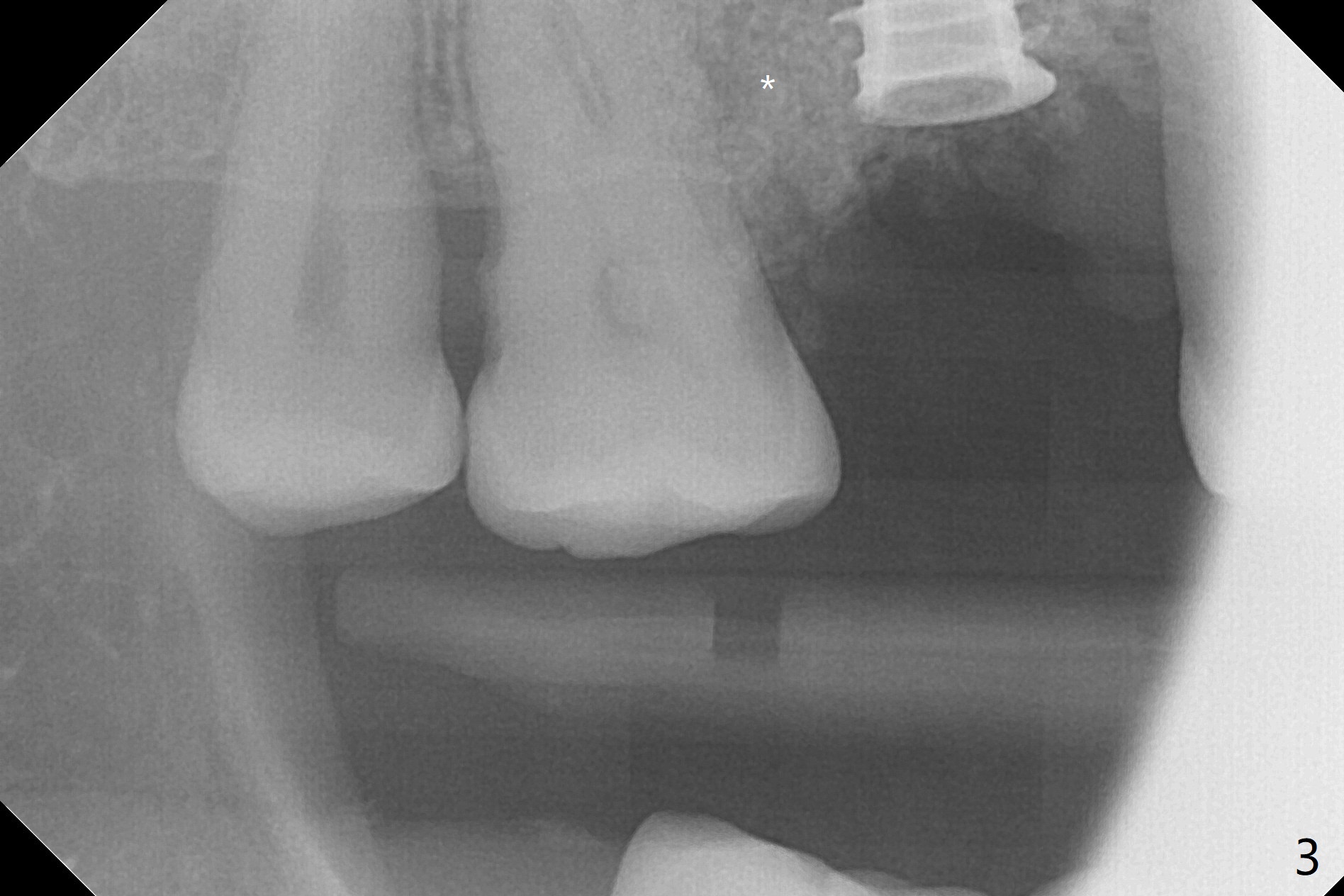
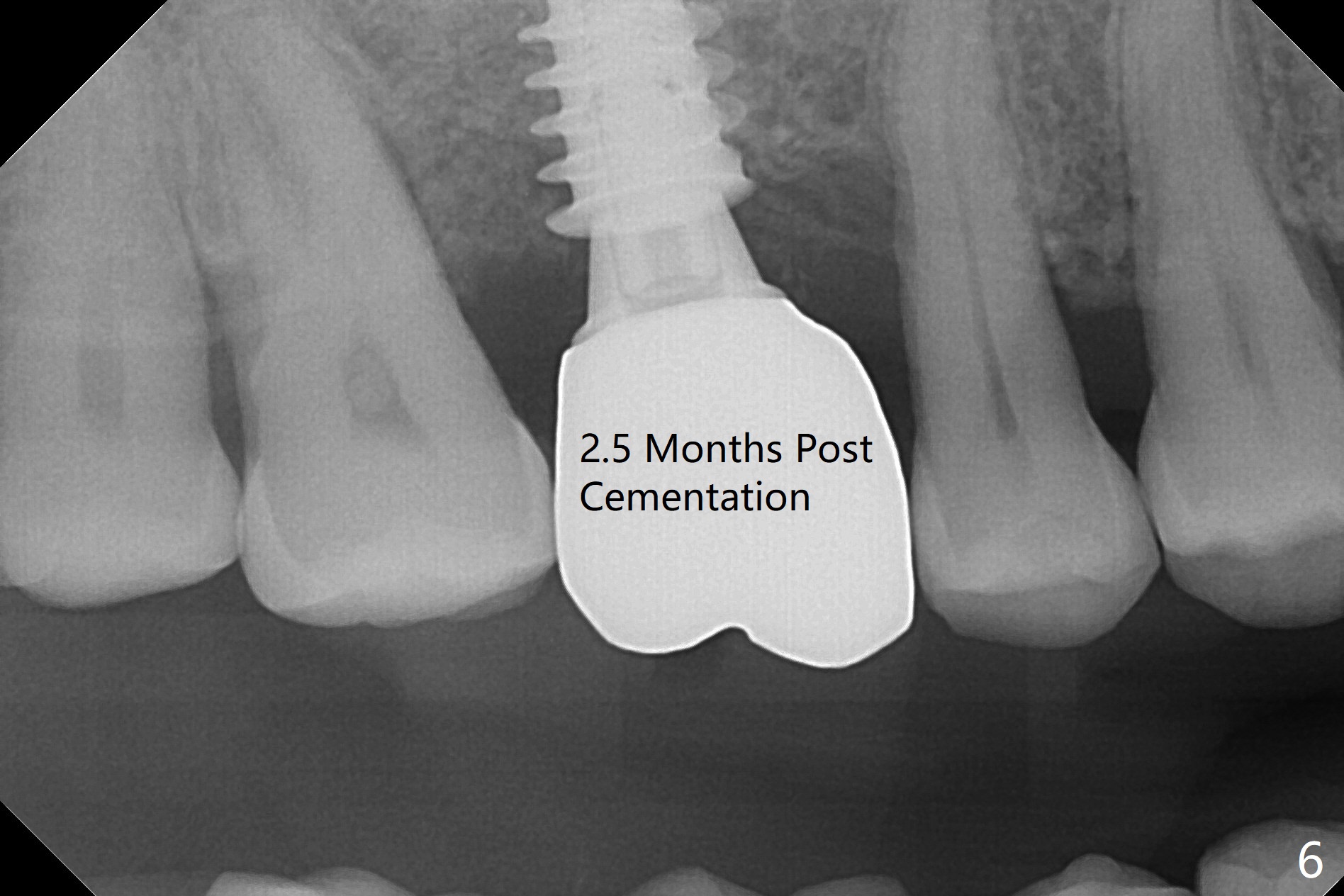
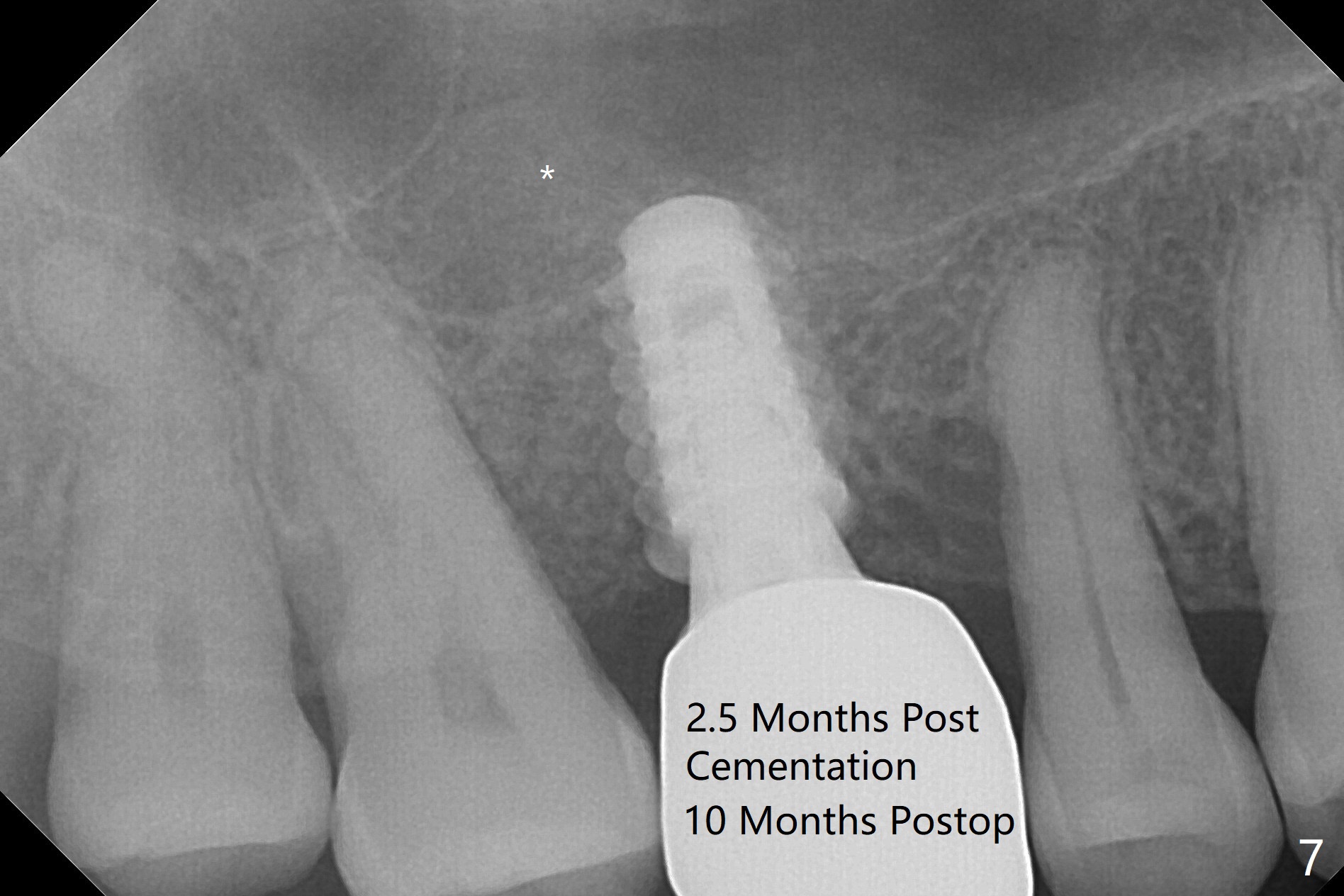
After extraction and debridement, osteotomy is initiated in the mesiobuccal socket free hand. Since the remaining bone is ~ 2 mm, the sinus floor is perforated suddenly. Fortunately the sinus membrane is not, as related to its thickening (similar to water ballooning, without symptom). Use 2-3.5 mm drills to enlarge the bony perforation (mainly lateral movement), followed by pushing bone graft upstairs with a curette (Fig.1 *); insert a 4x9 mm dummy implant (Fig.1) to determine the length of the final implant (Fig.2,3). A drawback of this case is the low torque (<20 Ncm), considering the thin bone. Following deeper implant placement, a 5.2x6(2) mm temporary abutment is placed for an immediate provisional to keep large amount of bone graft in place (Fig.3 *). There is no pain 1 week postop, while the immediate provisional remains stable partially because of the temporary abutment (Fig.4 ^). Four months postop, the temporary crown is loose. After removal of the temp and the temp abutment, gingival cuff is erythematous. A 6x4 mm healing abutment is placed. The bone graft (Fig.3 *) appears to have attached to the root of the neighboring tooth and the implant threads 7 months post op (COVID 19, Fig.5 arrowheads)). The bone graft appears to continue to merge with the neighboring root, bone and implant 10 months postop (2.5 months post cementation, Fig.6). The bone graft in the sinus seems to collapse and condense 10 months postop (Fig.7 *).
Upper Molar Immediate Implant, Prevent Molar Periimplantitis (Protocols, Table) Trajectory II 23 Xin Wei, DDS, PhD, MS 1st edition 11/11/2019, last revision 09/14/2020