







|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Endodontic Disease M
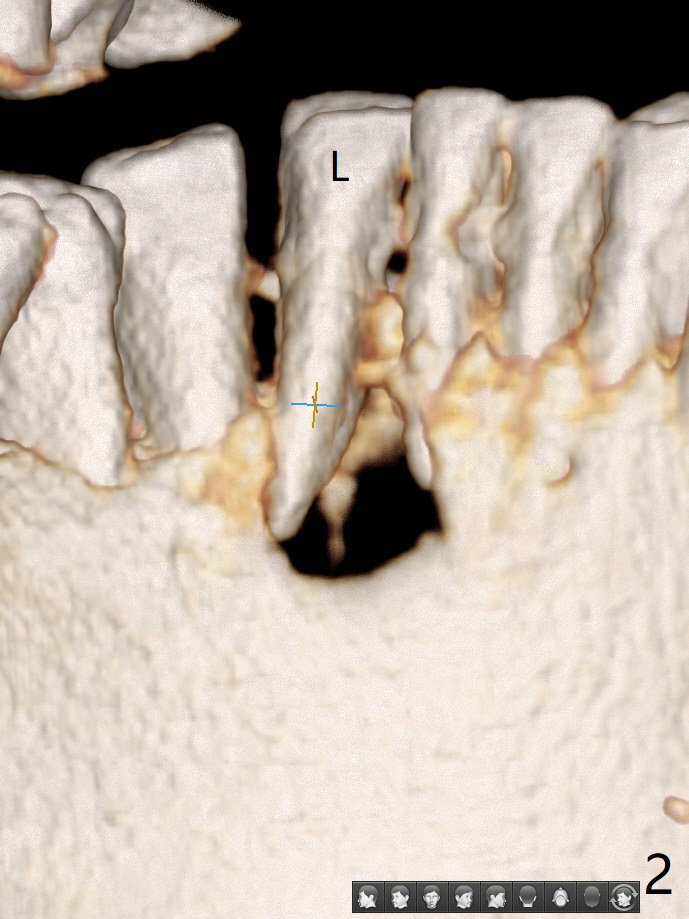
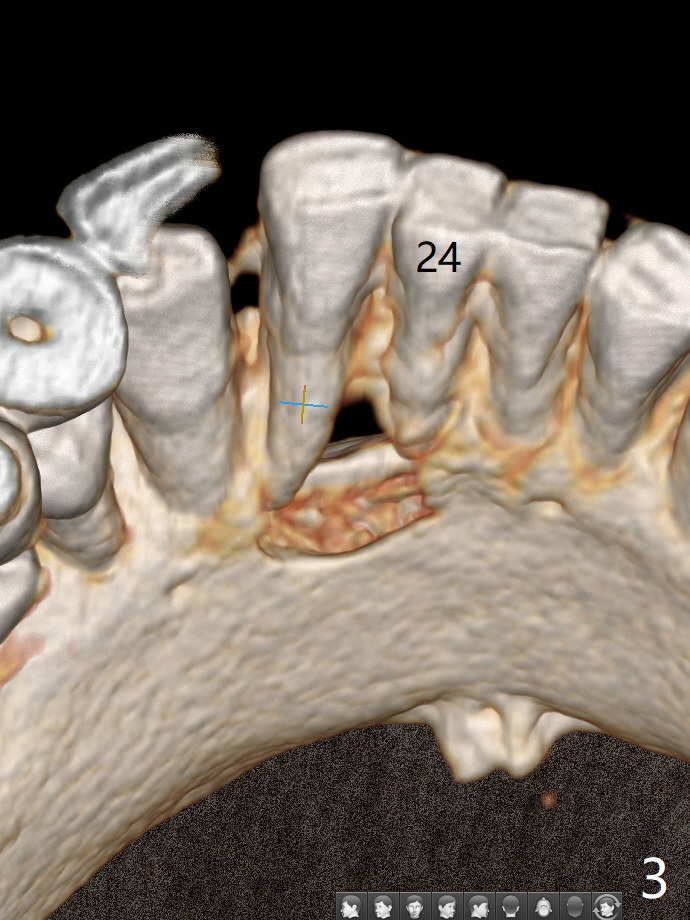
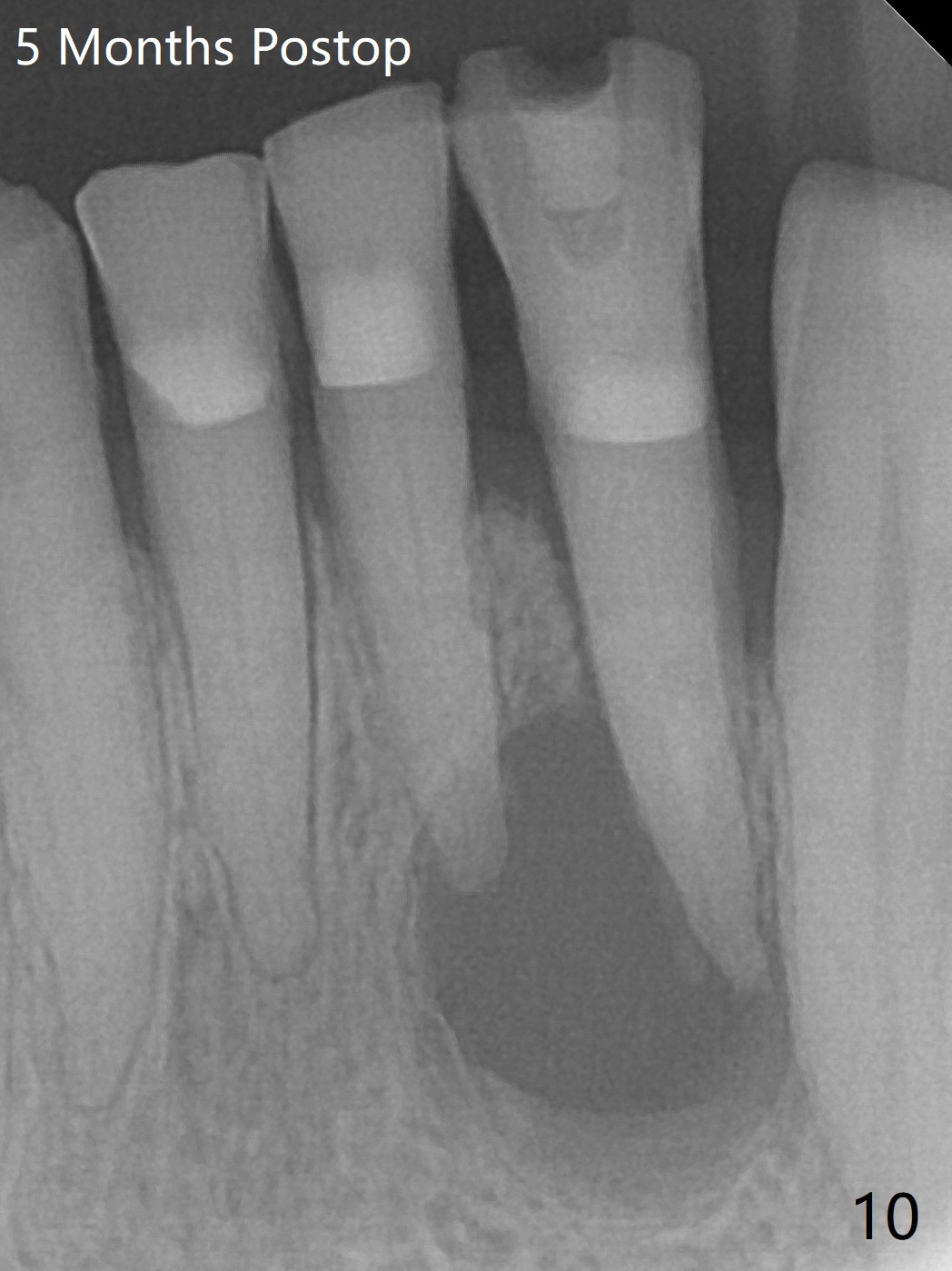
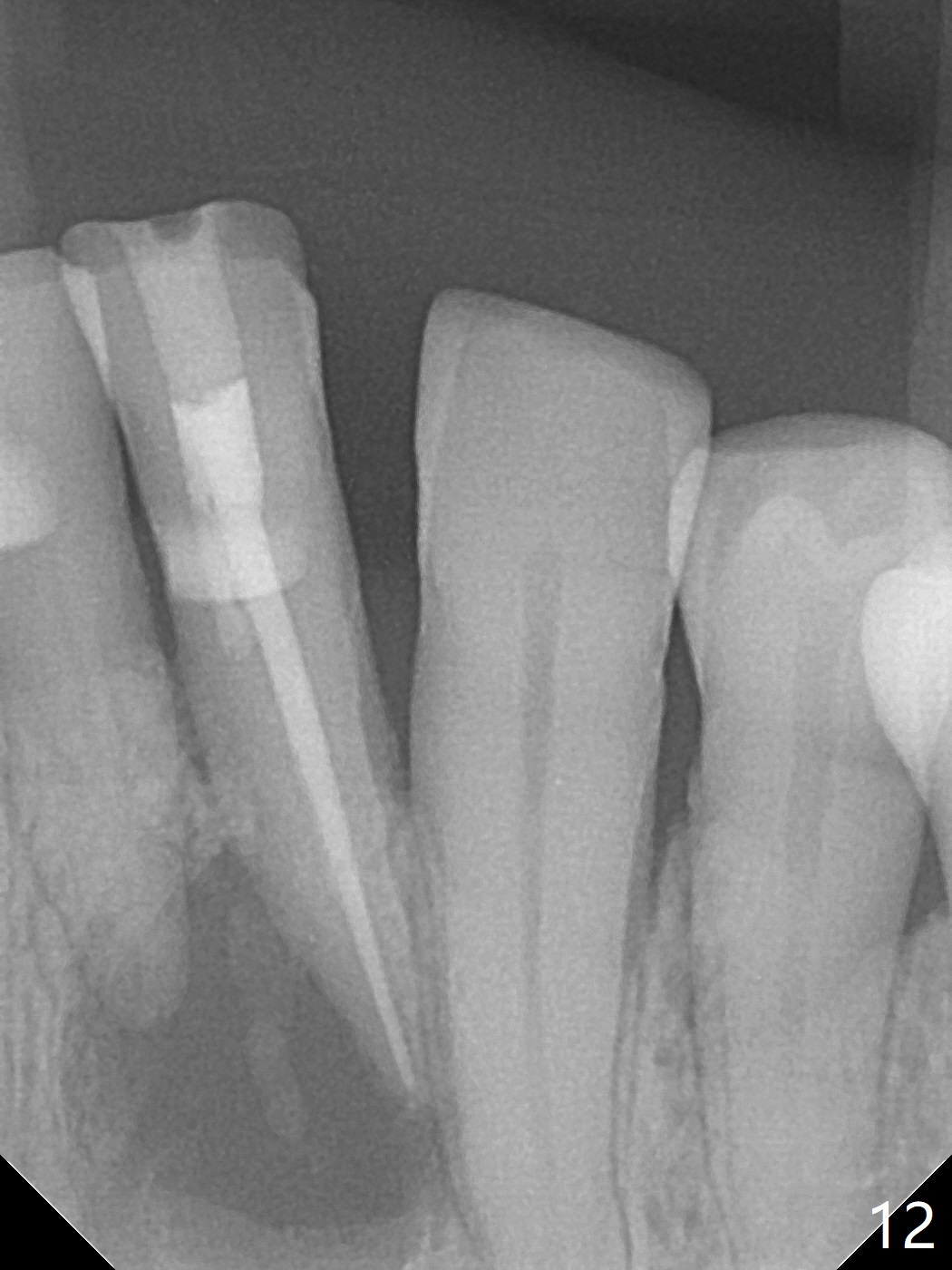
A 73-year-old woman has discomfort associated with #23 four months post Class V composite at #23-25 (Fig.1 C (*: Class V lesions)). Bone loss seems to be more severe lingually, especially at the crest (Fig.2 L). It appears that the apex of the tooth #24 is also in the large apical lesion (Fig.3). Class V composite is apparently continuous with the pulp at #25,24,23 (Fig.5-7). In contrast, Class V defect does not involve the pulp at #26 (Fig.4). If necrosis is confirmed clinically for #23 24 and 25, RCT will be conducted. Due to 7-day Amoxicillin taken for #3 implant, the patient feels that her tongue moves freely, as related to reduction in pain and swelling lingual to #23 (Fig.8 *). Endo ice test shows necrosis of #23 to 25. RCT is initiated at #23 (Fig.9) with buccal and lingual swelling. Endo may have to be at #24 with apicoectomy with PRF. The lingual swelling remains at #23, although there is no pain or purulent discharge 5 and 5.5 months post debridement (Fig.10,11). RCT is finished (Fig.12). Apicoectomy is pending with PRF. Less aggressive curettage will be done at #24 to maintain apical blood supply. Vitality tests have been done without conclusion.
Return to Lower Incisor Immediate Implant, Trajectory II Clindamycin Metronidazole No Antibiotic Shield
Xin Wei, DDS, PhD, MS 1st edition 11/11/2019, last revision 08/09/2020