

|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Sticky Bone
for Sinus Lift
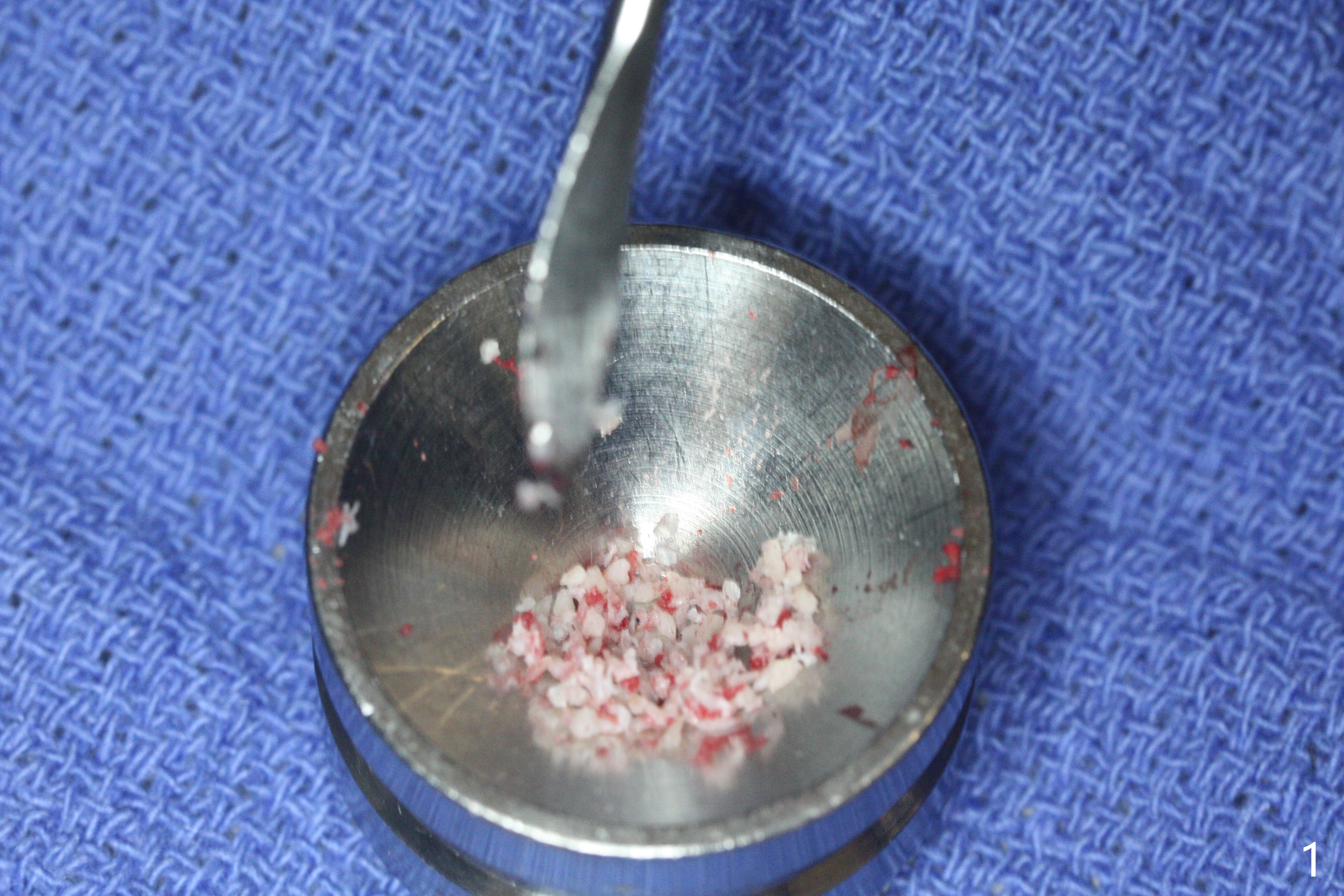
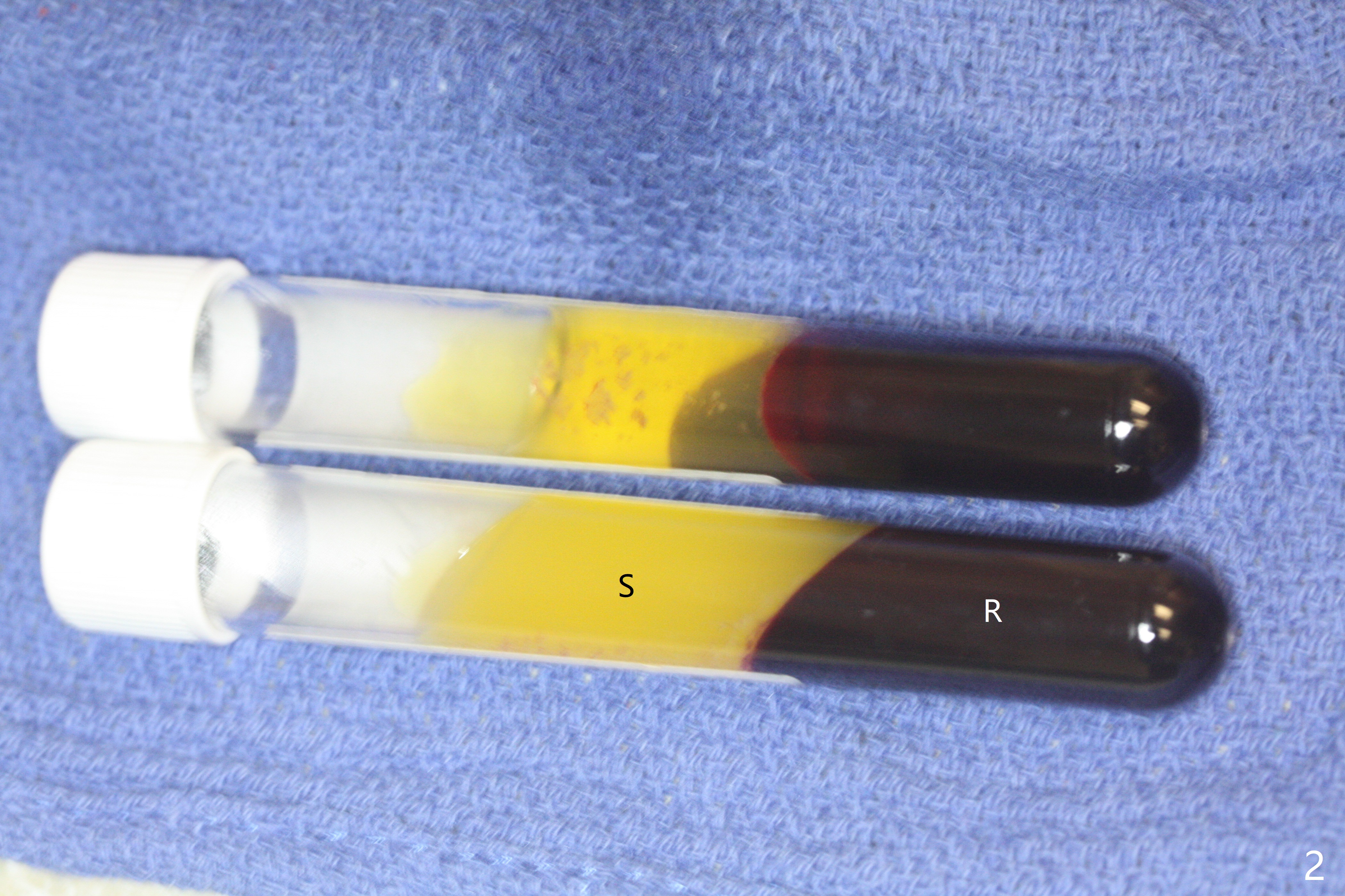
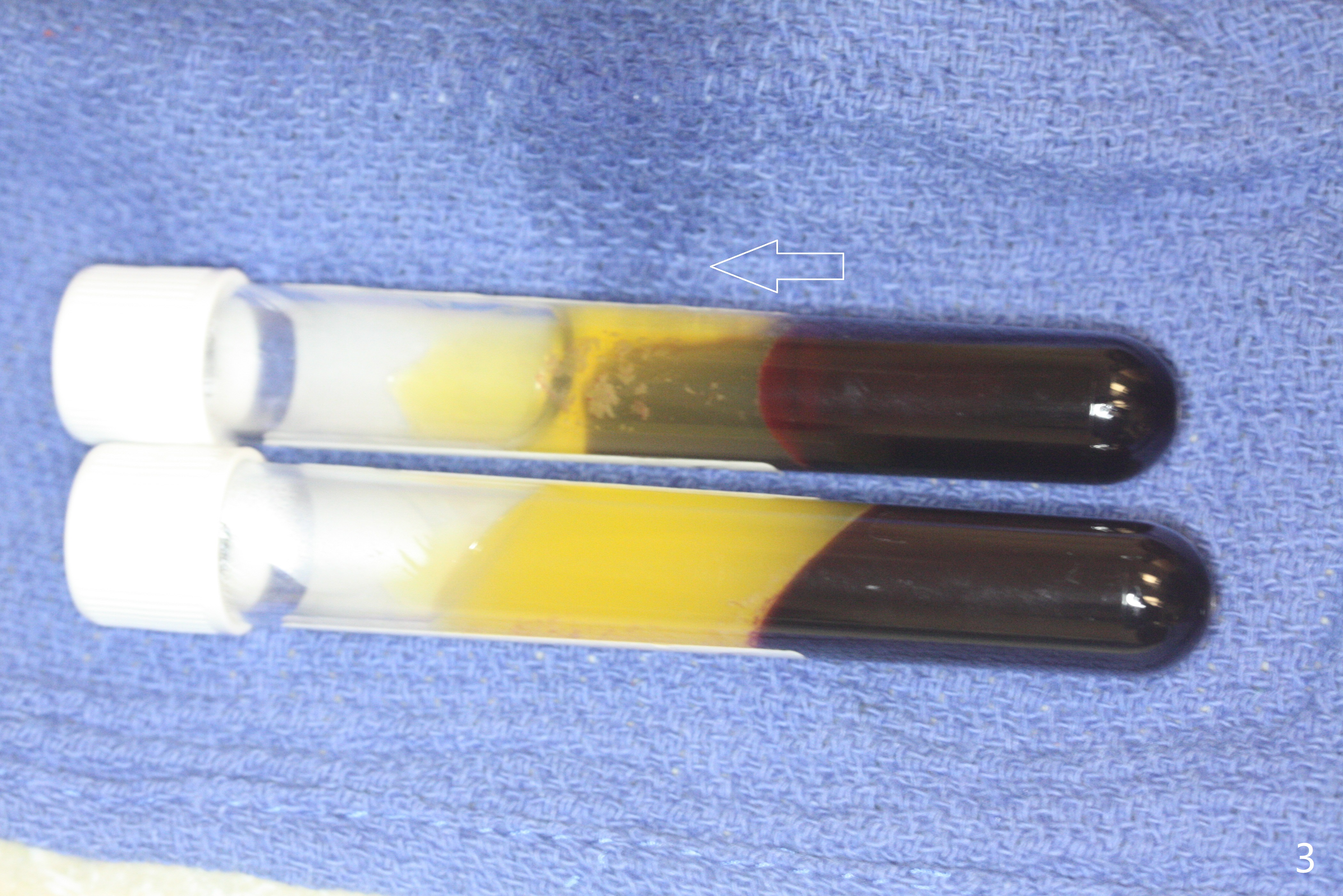
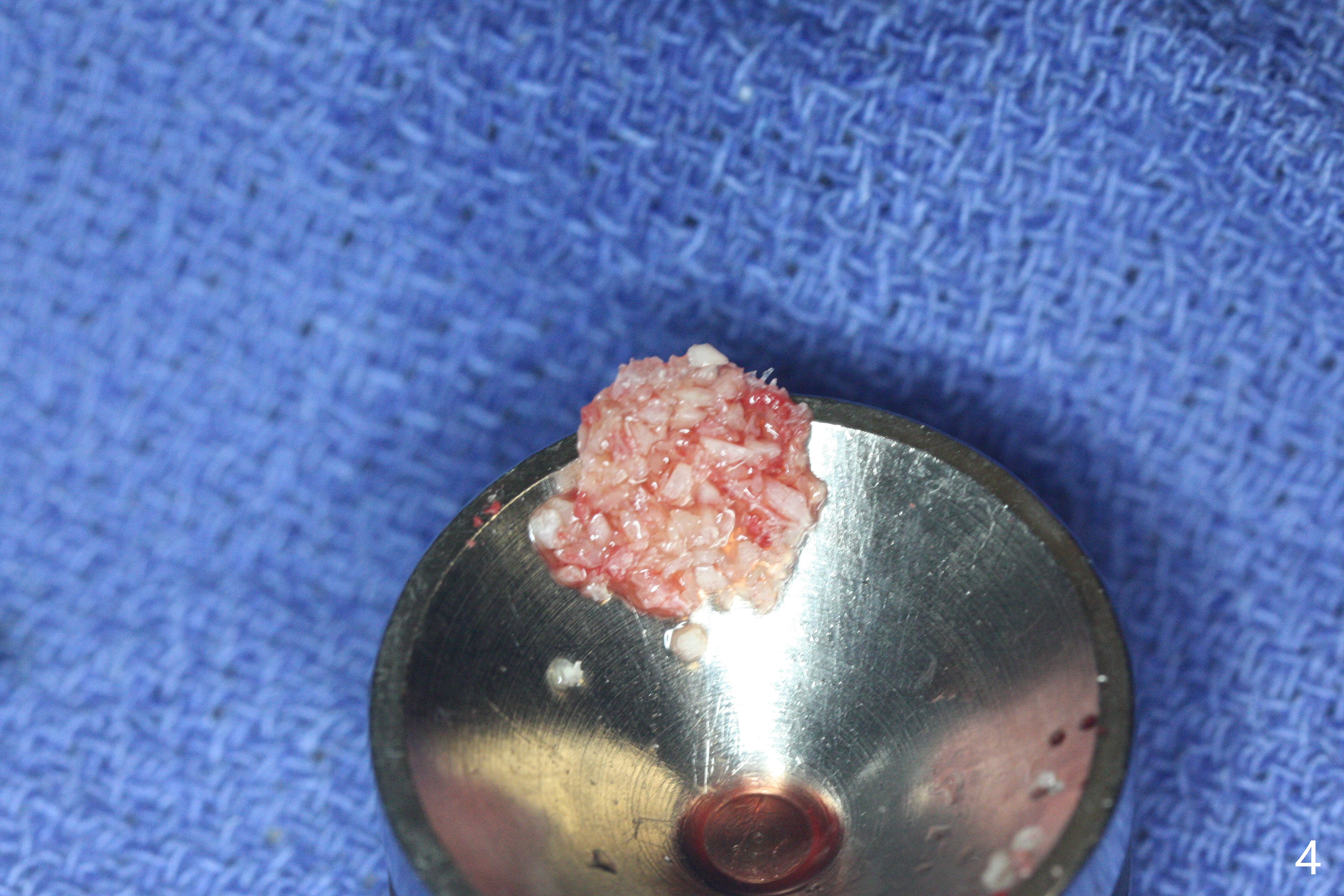
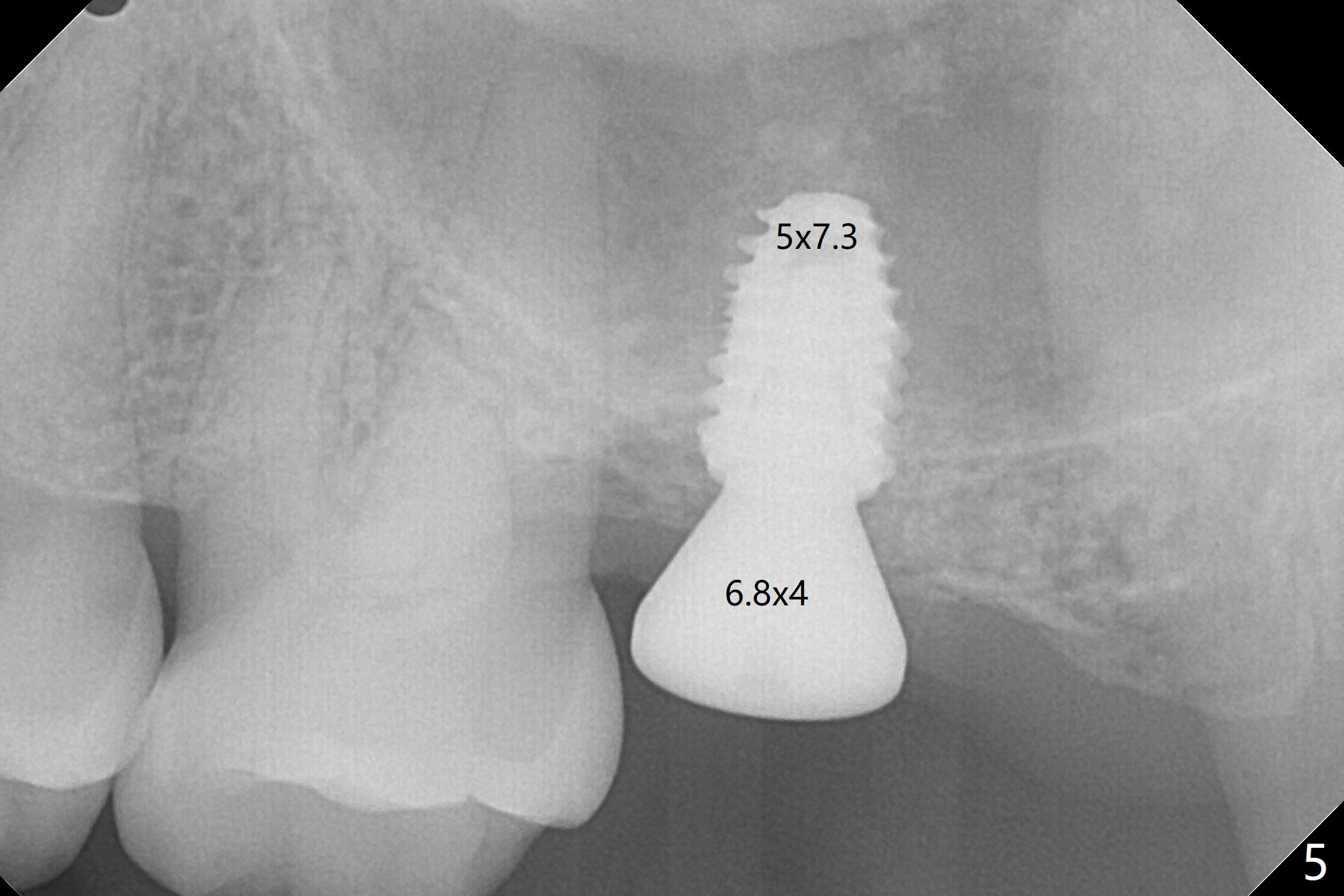
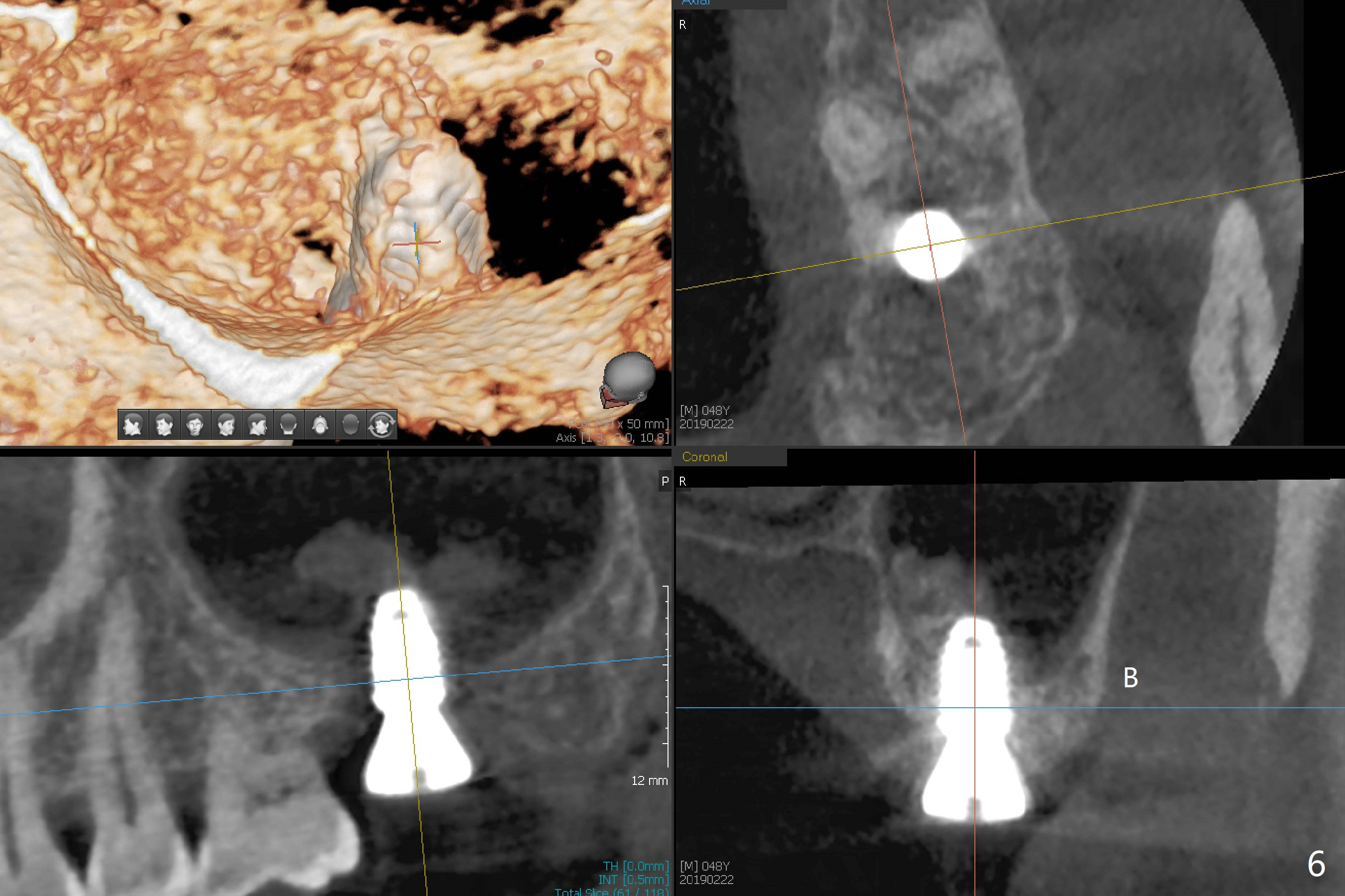
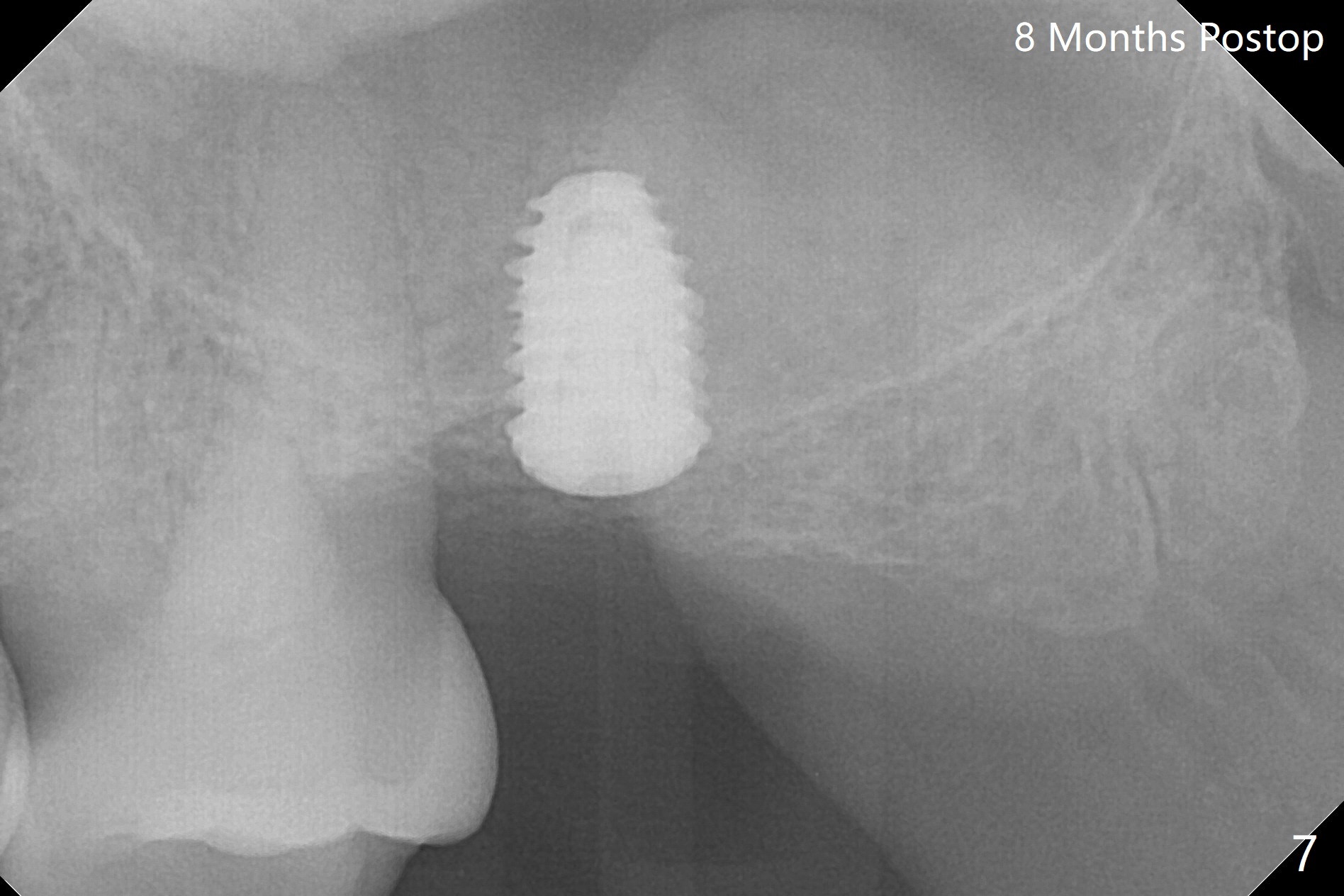
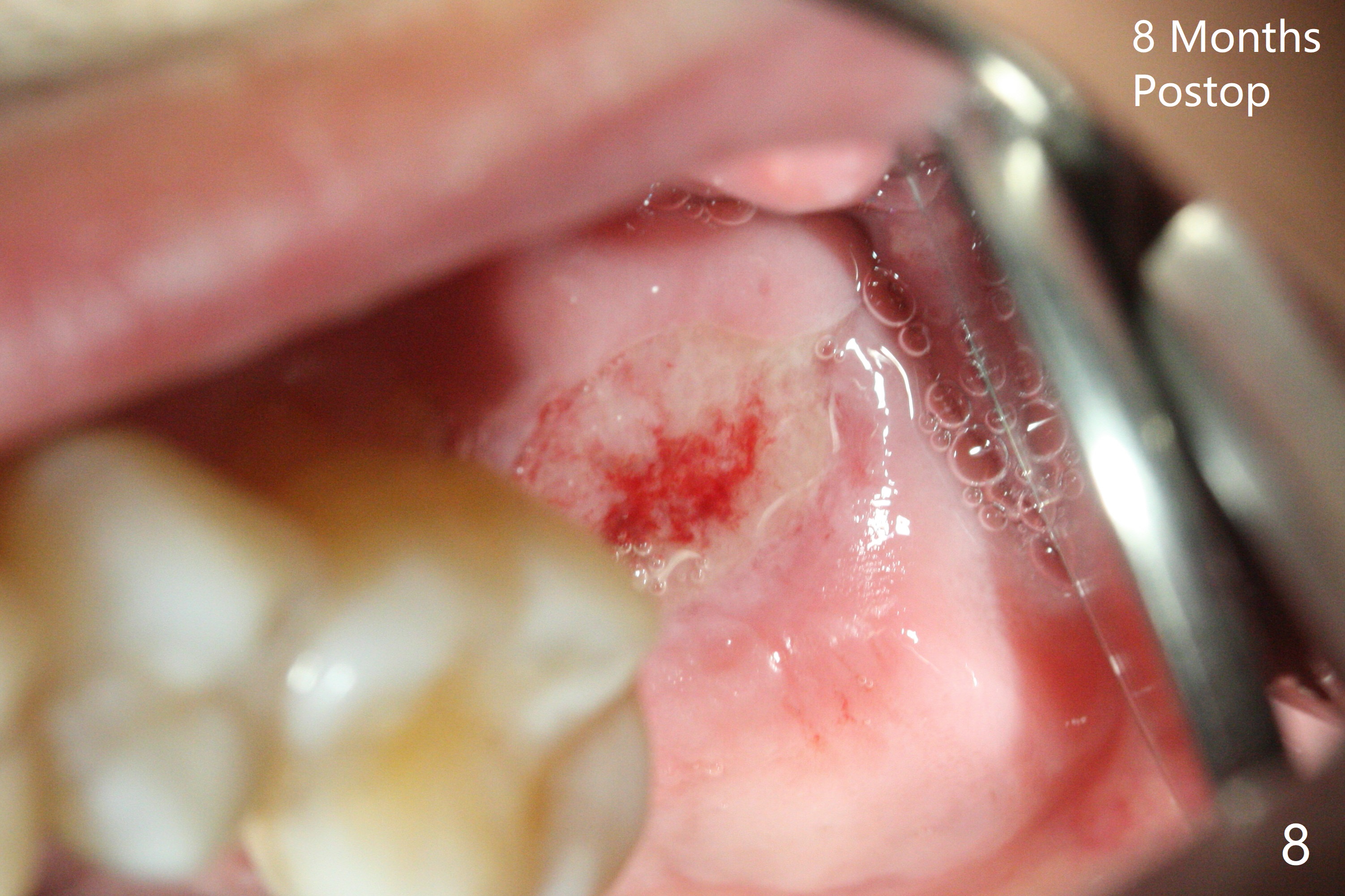
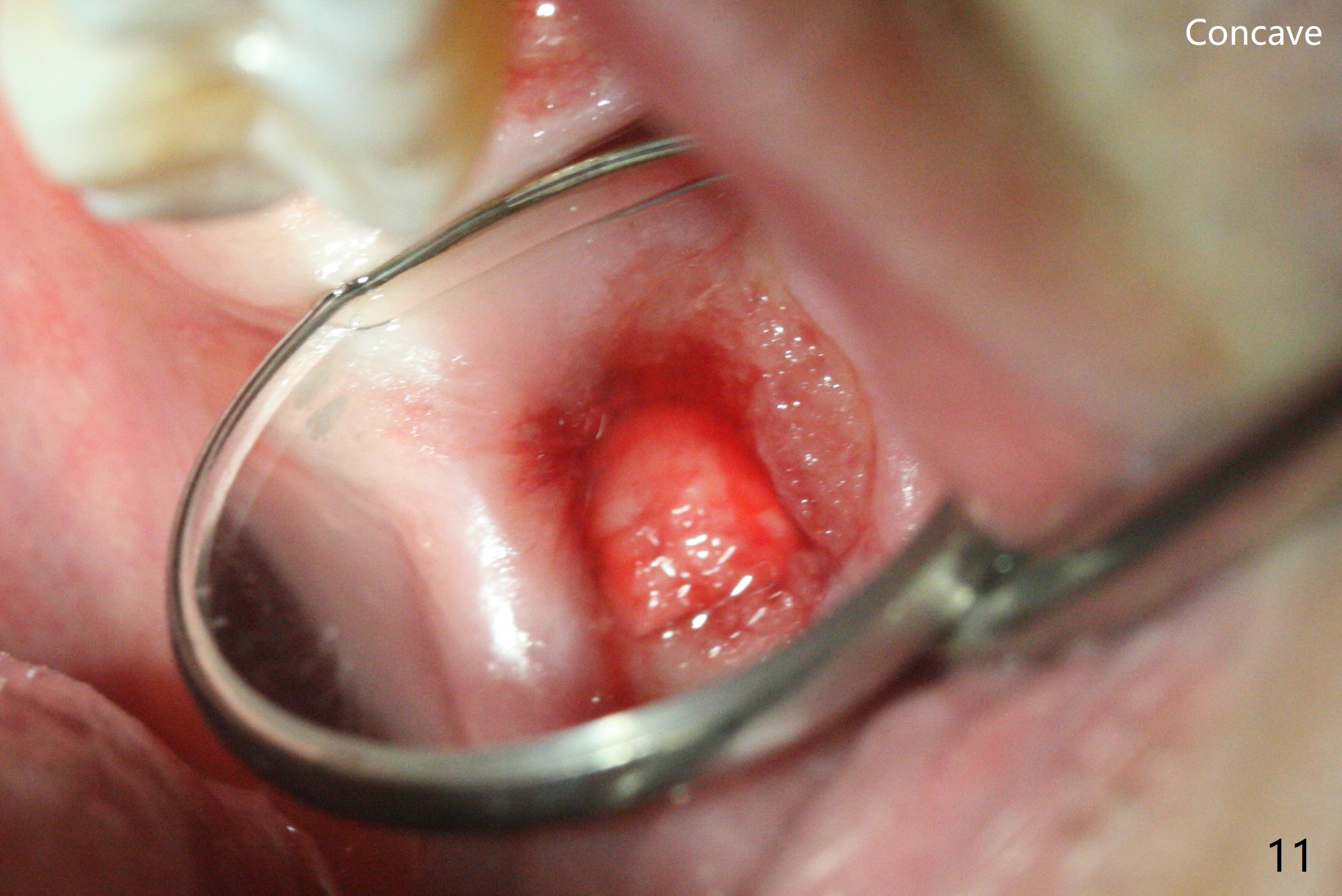
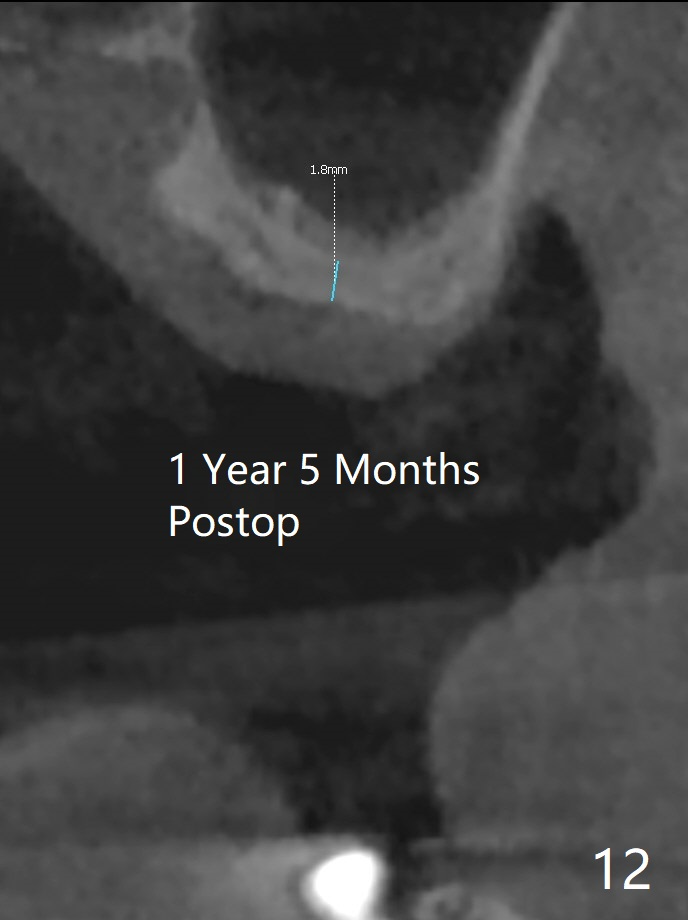
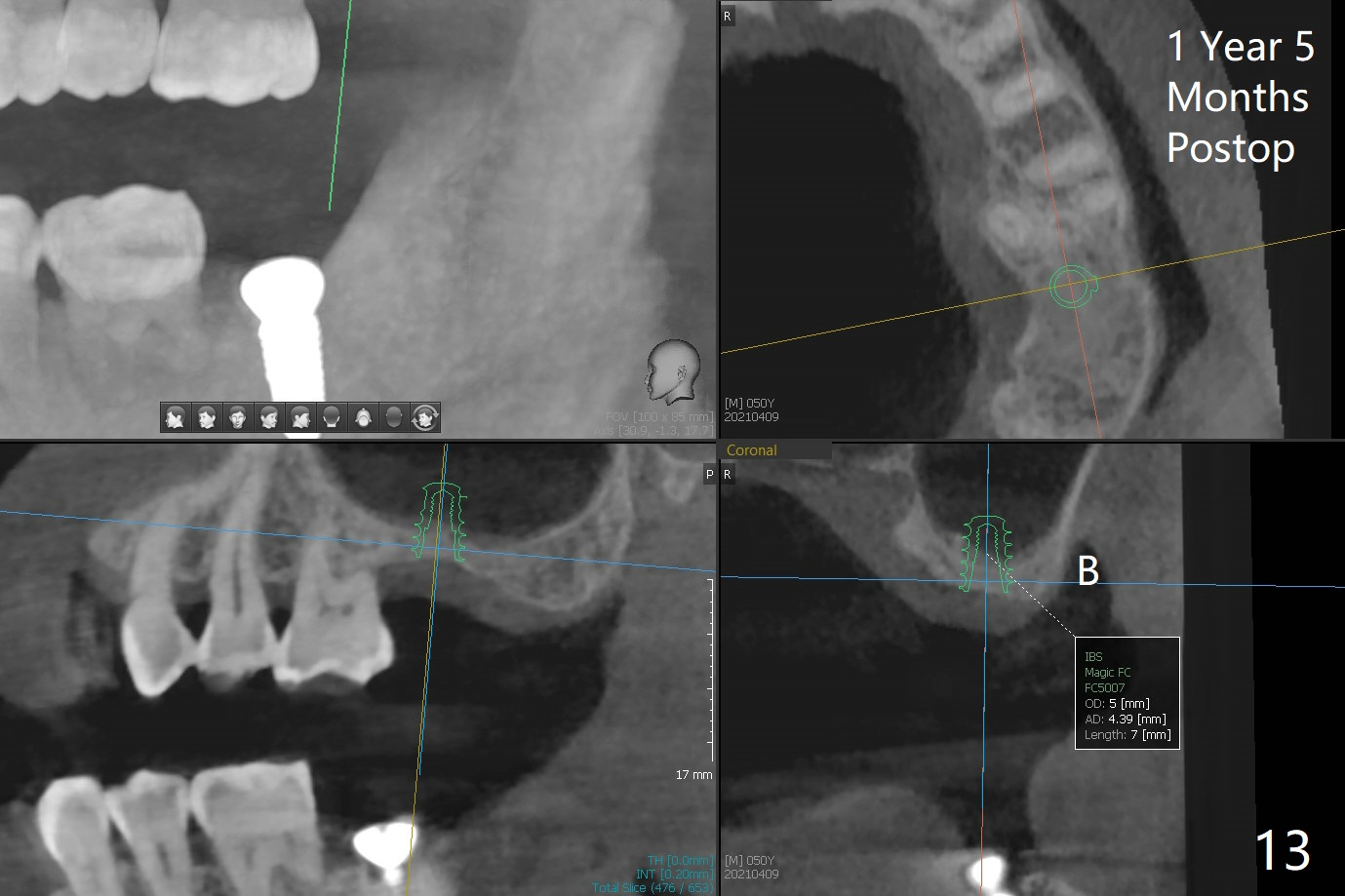
After 4.5x7.3 mm drill with 3 O-rings at #15, use 2.2x7.3 mm one with 2 O-rings. The sinus floor feels like to be perforated, but perio probe does not find the perforation. Nose blowing does not reveal air leakage. It seems fine when 3.0x7.3 mm one with 2 O-rings is being used. The sinus membrane perforates when Magic Sinus Lifter is used. Mixture of autogenous bone (from drills) and allograft does not stick to the periosteal elevator (Fig.1). Forty-minute centrifuge leads to separation of serum (Fig.2 S) from Red Blood Cell layer (R). The separation of the top tube is incomplete with RBC invade the serum layer in a few second (Fig.3 arrow). While the serum layer of the bottom tube is prepared for PRF membrane, a part of the serum layer of the top tube is withdrawn to make sticky bone (Fig.4). The top tube returns to the centrifuge for another 30 minutes to make the second PRF membrane. The first PRF membrane is inserted into the osteotomy and pushed into the sinus with empty feeling, followed by the sticky bone and last by the 2nd PRF membrane. A 5x7.3 mm implant is placed with ~ 10 Ncm, followed by a 6.8x4 mm healing abutment (Fig.5,6 (retrospectively healing screw should be used to reduce sinus-oral communication)). There is no mushroom in the sinus, but hopefully the sticky bone will stick to the bottom of the sinus for maturation. Sinus surgery precaution is provided. Next time tap or dummy implant will be used for sinus lift after initial osteotomy with guide. In fact the patient with diabetes under control has mild cold. The procedure should have been canceled. There is no postop nasal hemorrhage or discharge. The patient returns nearly 8 months postop. The wound is infected. The healing abutment is changed to a healing screw with oral antibiotic. Two weeks later, the area remains infected with symptoms (Fig.7-9). The healing screw is not covered completely. After implant removal, the sinus membrane is perforated. A piece of collagen plug (preferably Osteogen plug) is inserted (Fig.10,11). Because of the concavity, bone graft seems necessary when the wound heals. One week later, perimplantitis develops at #2. The patient is ready for the 3rd placement 1 year 5 months post last implant removal (Fig.12). The bone is 1.8 mm thick, apparently composing of 2 fused cortical plates. Make an incision for both external and internal sinus lift with retraction. Find the old guide to start osteotomy including bone trimmers and use Magic Lifter. If the membrane is broken, open the lateral window to repair with PRF.
Return to Upper Molar Immediate Implant, Trajectory 3rd Placement
Xin Wei, DDS, PhD, MS 1st edition 02/22/2019, last revision 04/11/2021