
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
What should
be done?
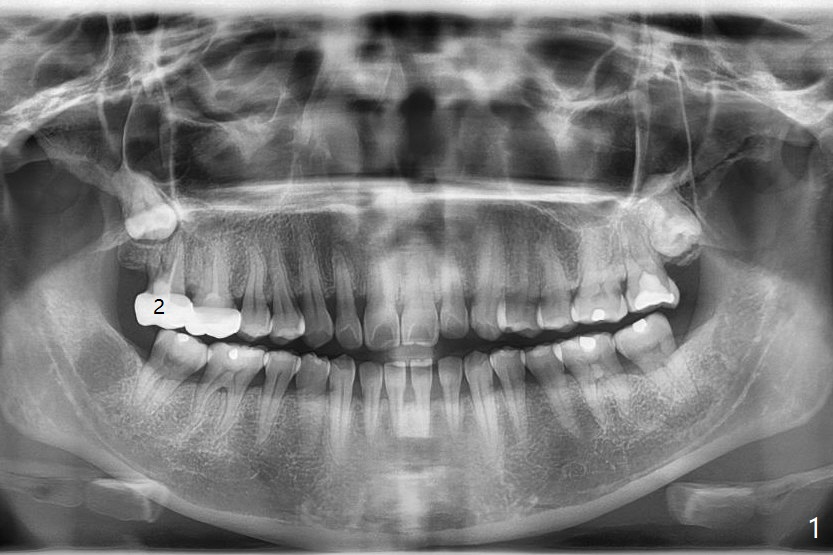
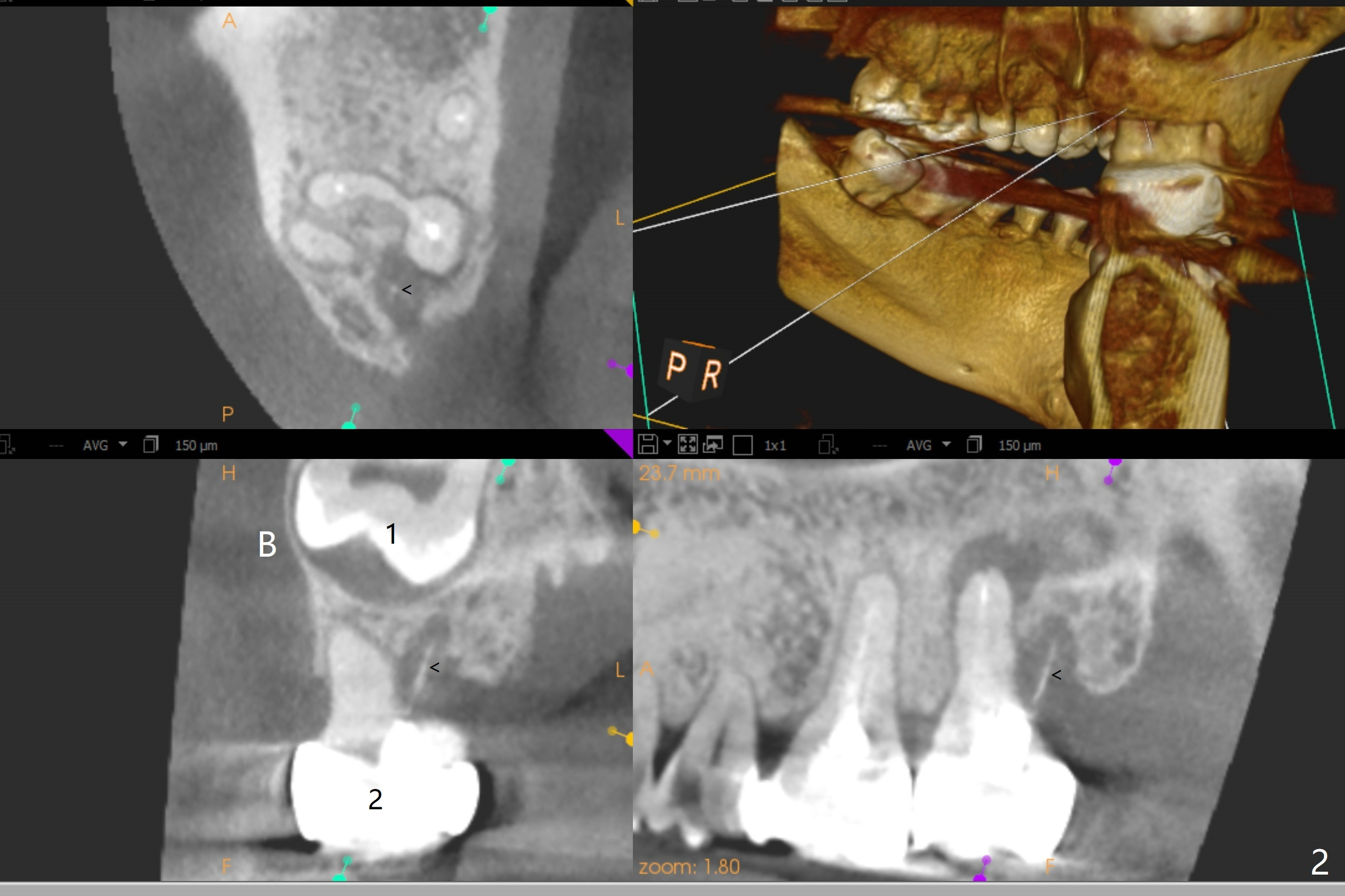
A 38-year-old woman returns to clinic with severe pain in the upper right 2nd molar (Fig.1), requesting immediate extraction. Endo consultation confirms nonsalvageability with gutta percha sticking out of the distobuccal root (Fig.2 arrowheads (B: buccal)). She would like to have an implant. What is the treatment plan? In fact the tooth #2 has been extracted with socket preservation.
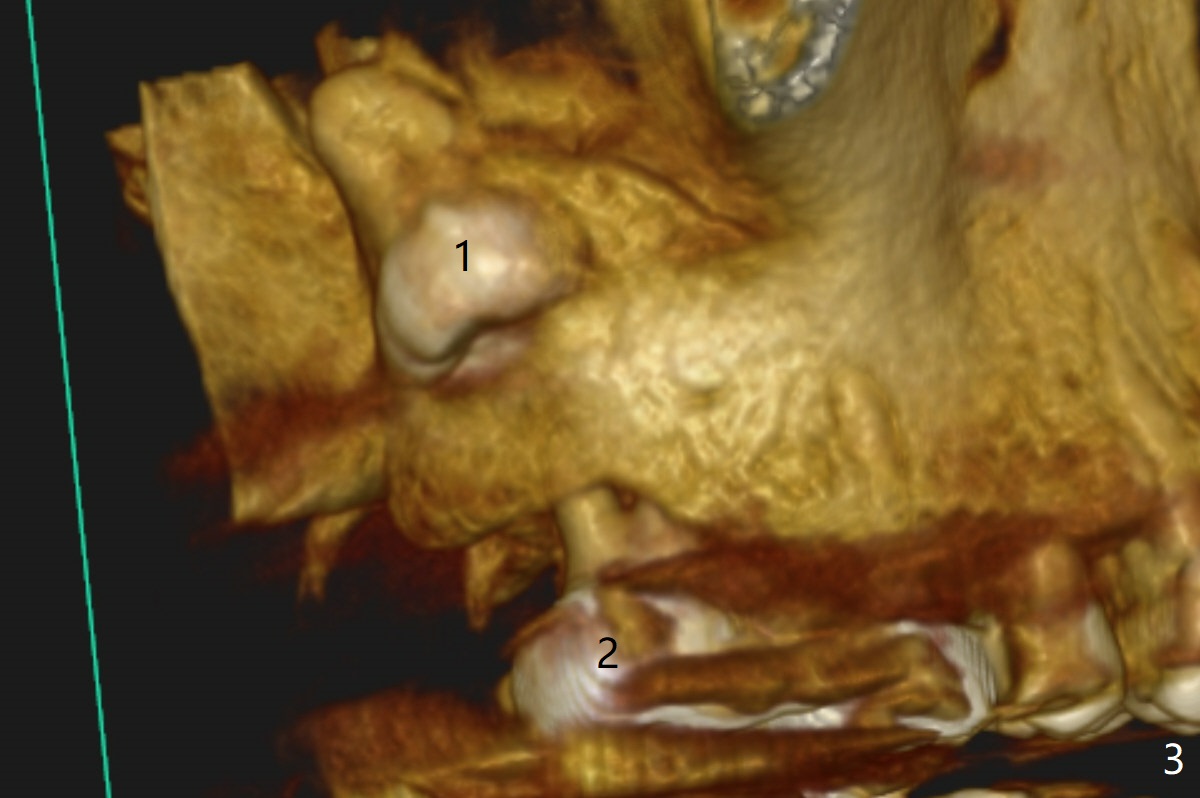
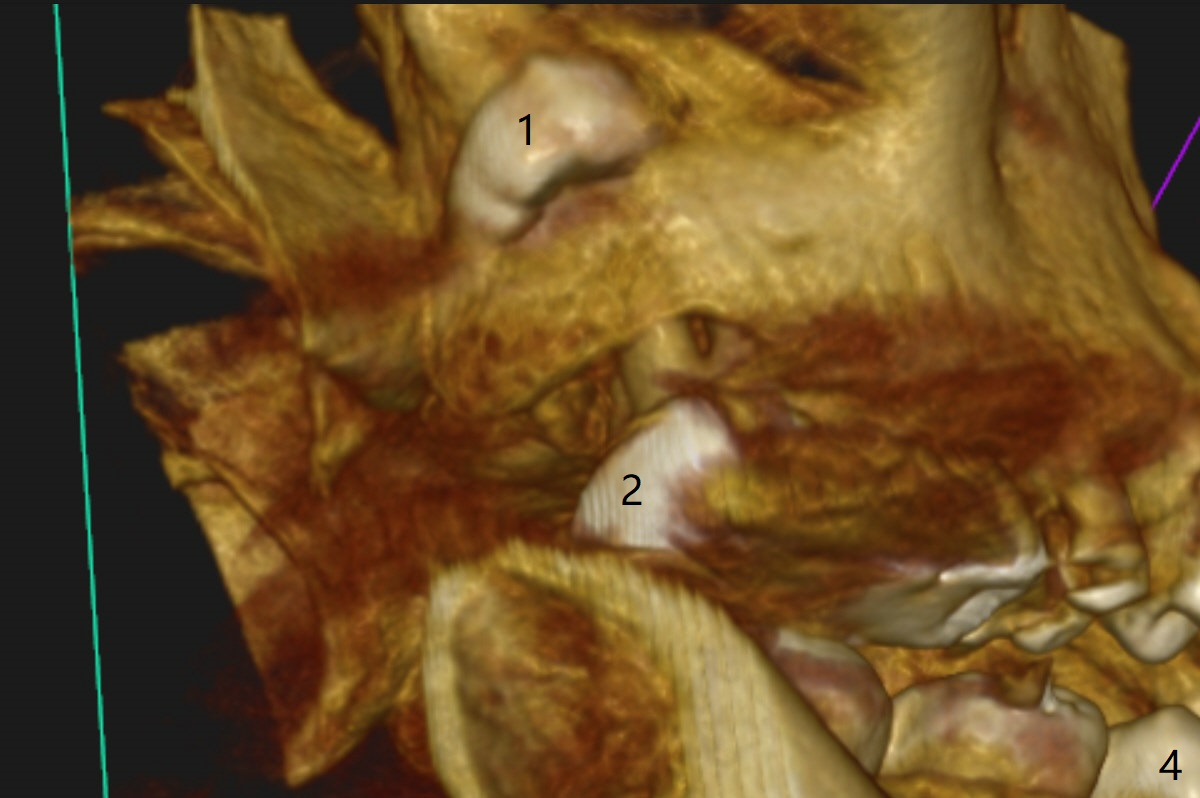
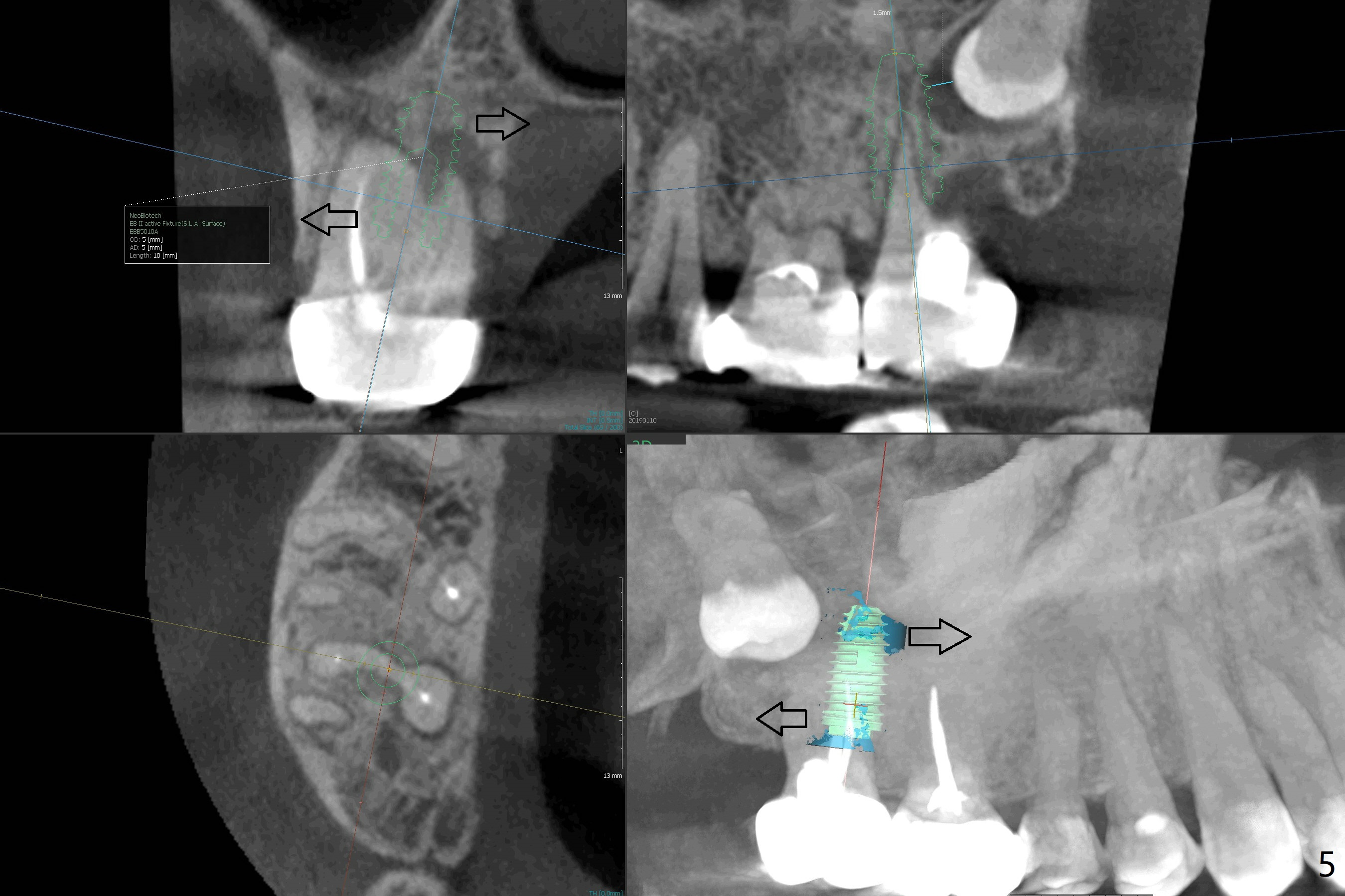
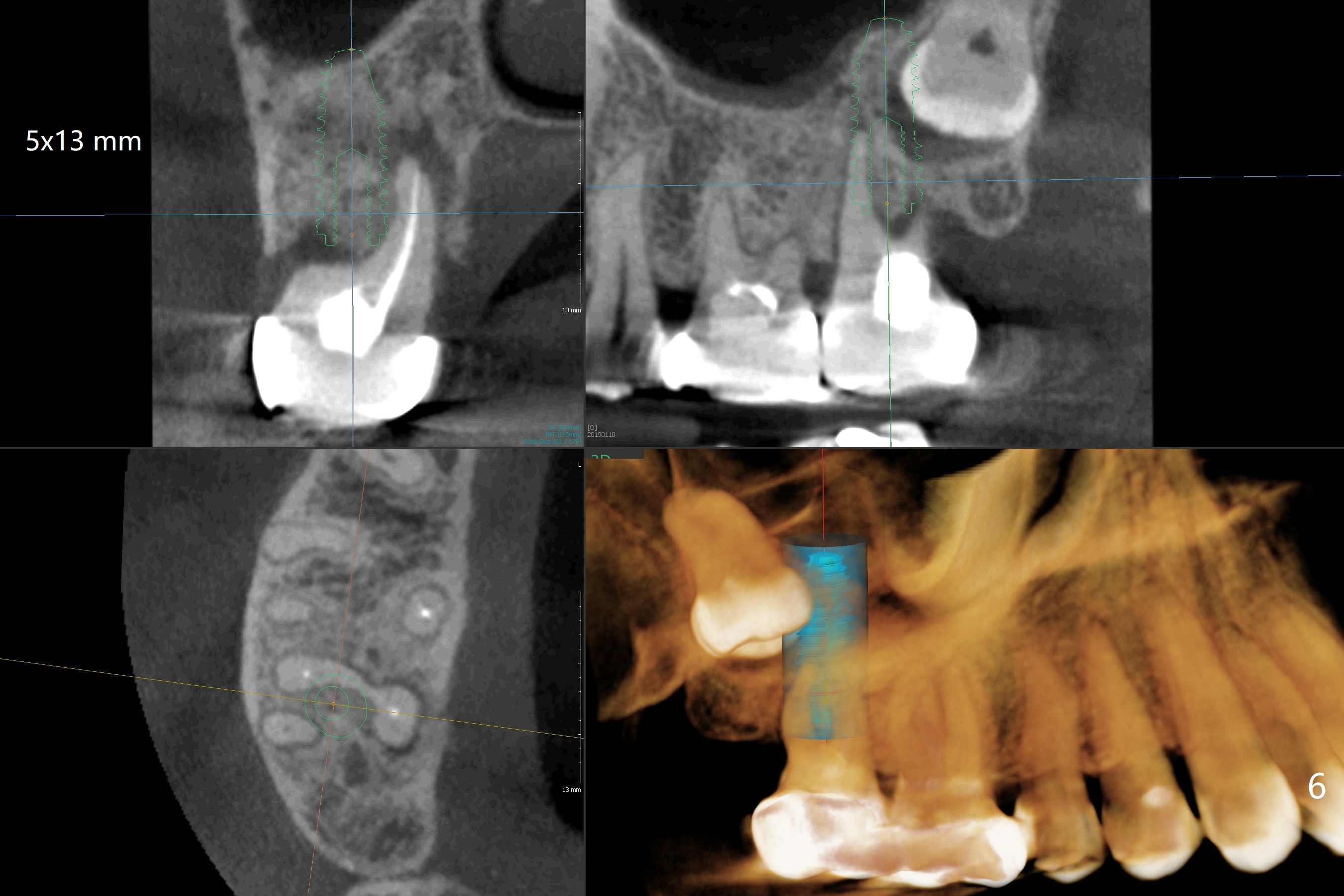
The tooth #1 should have been extracted buccodistally (Fig.3,4). Three or 4 months later, a 5x10 mm implant could be placed distopalatally superiorly to avoid removing the tooth #1 with ~ 1.5 mm clearance (Fig.5). To place an implant in orthopedic manner, the tooth #1 will be removed, while the implant should be longer (5x13 mm) to engage the bone superior to the socket of the tooth #1 (Fig.6).
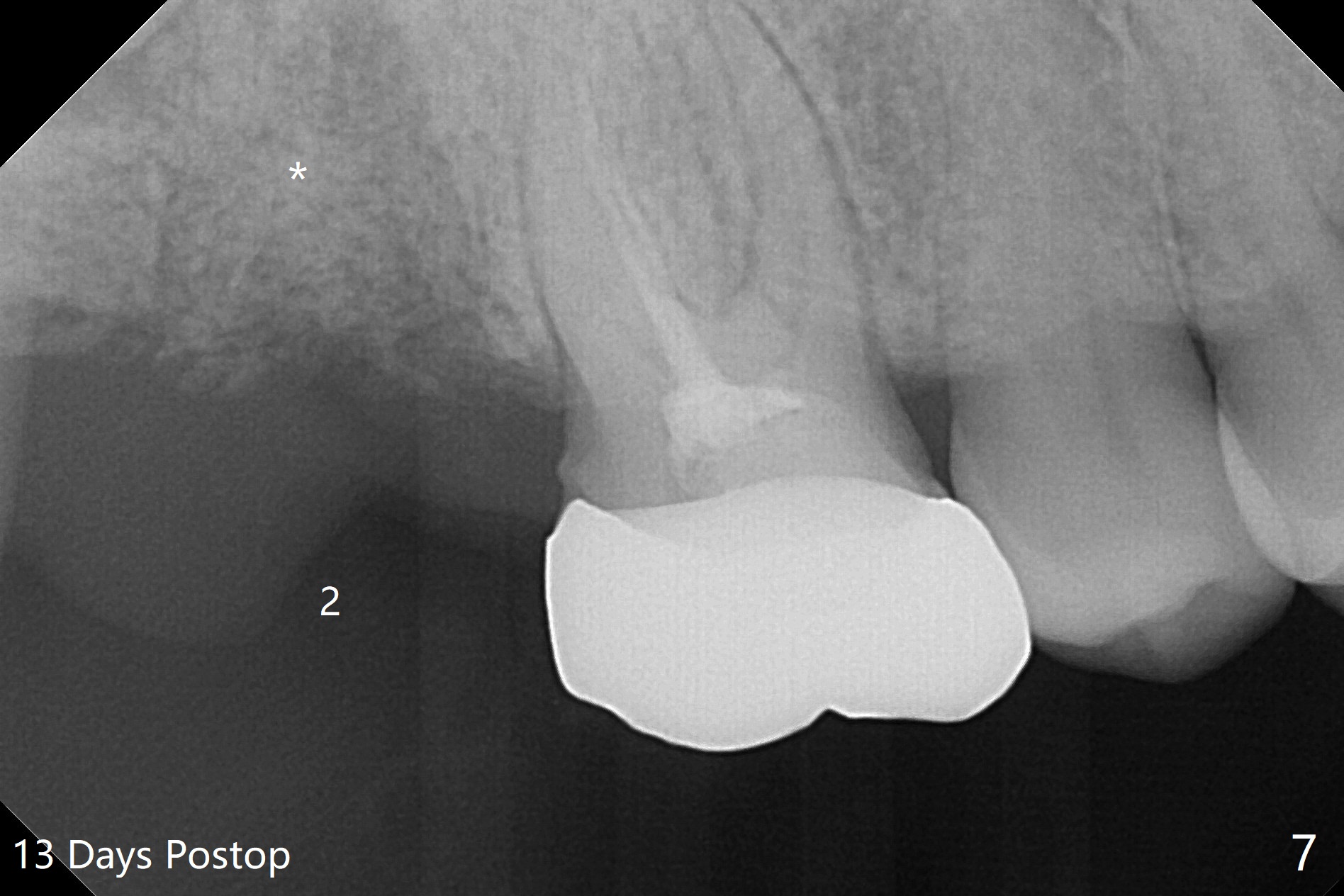
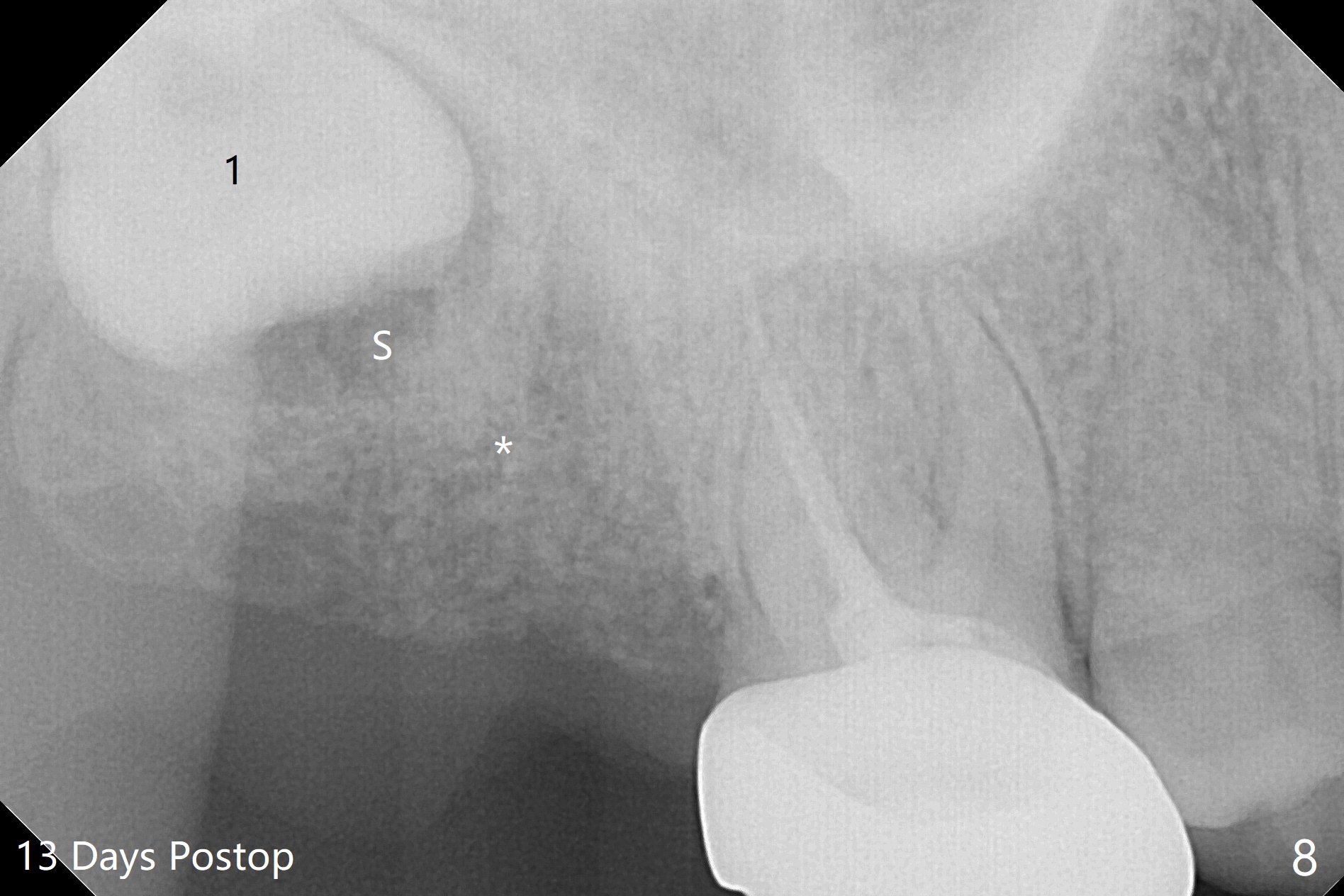
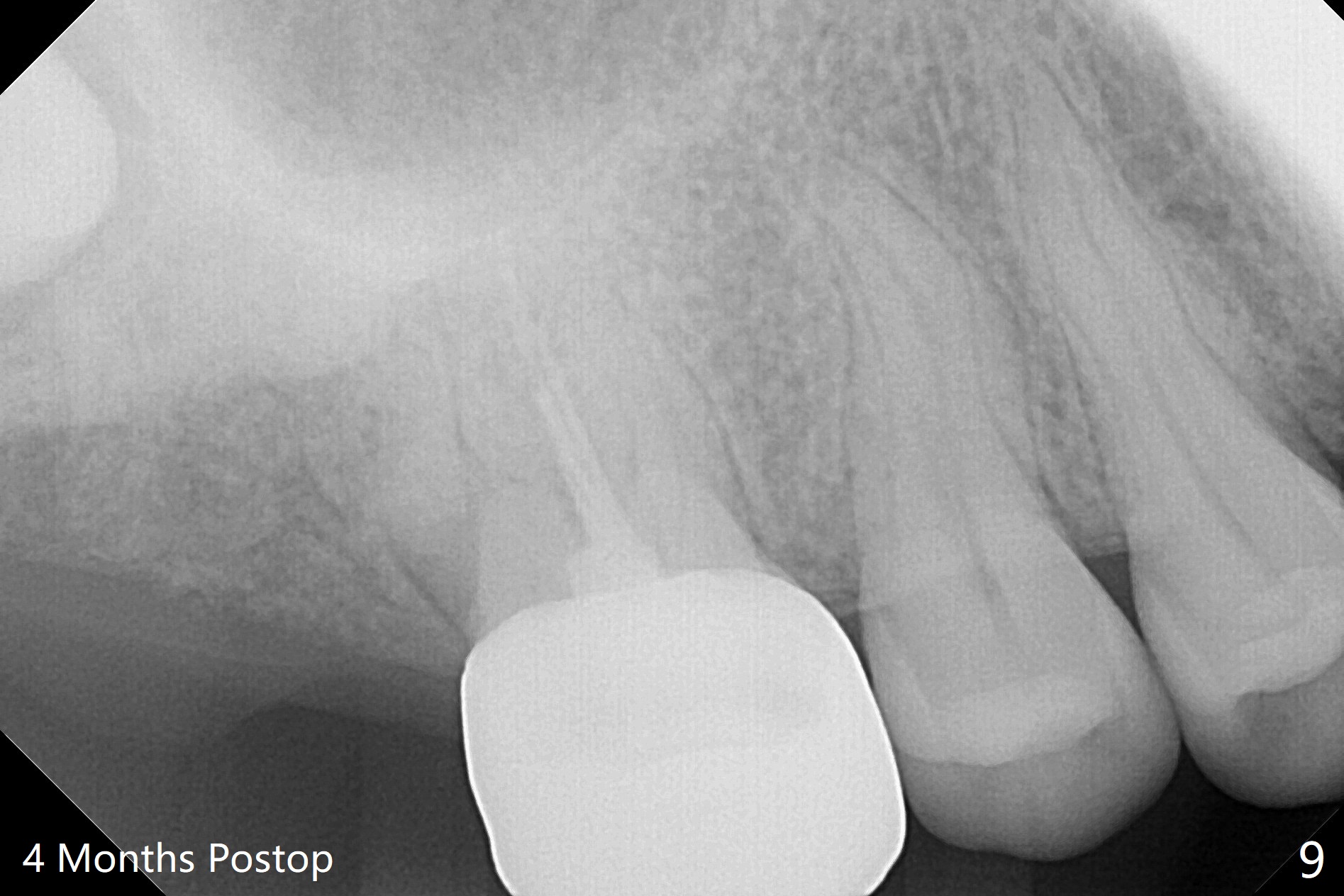
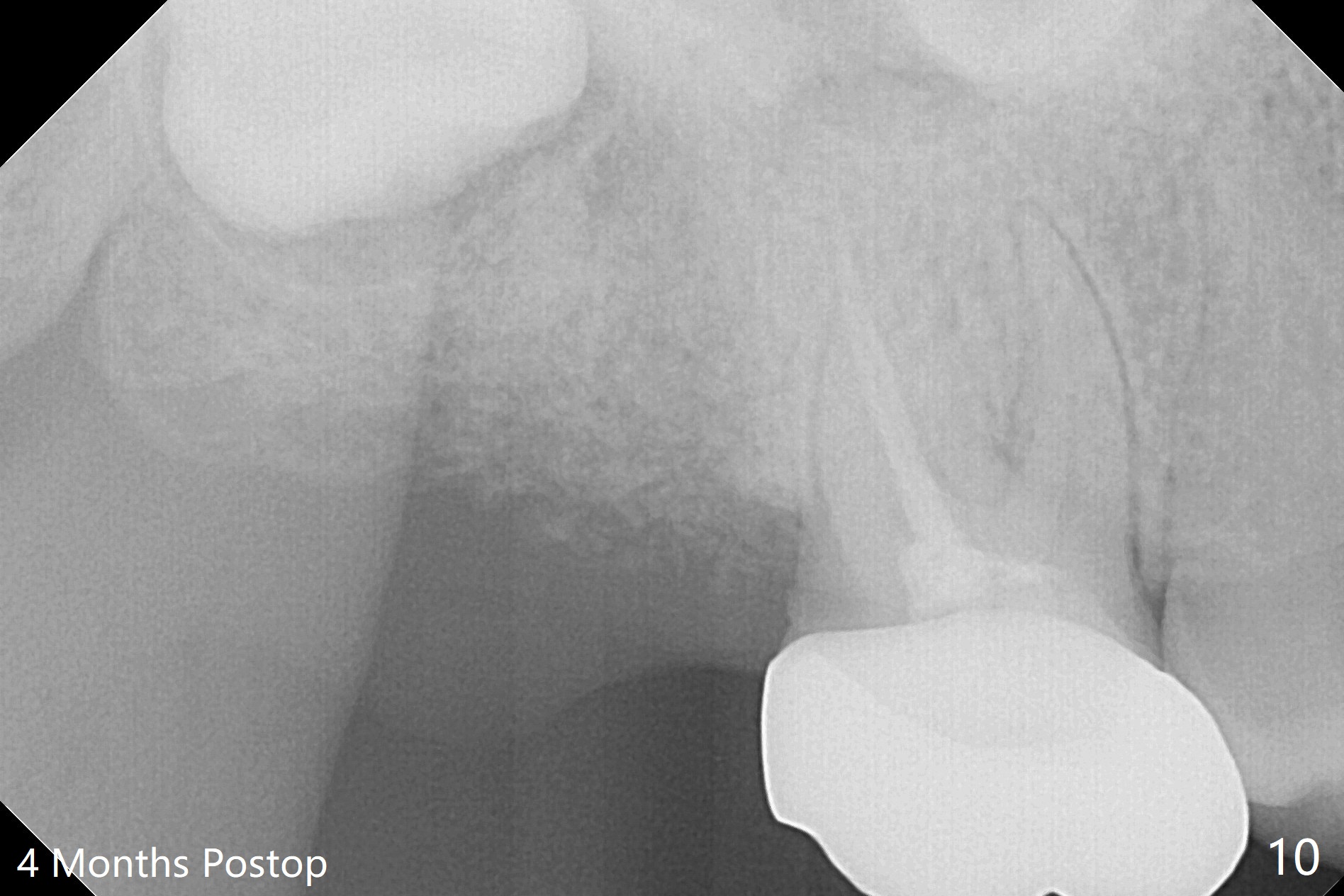
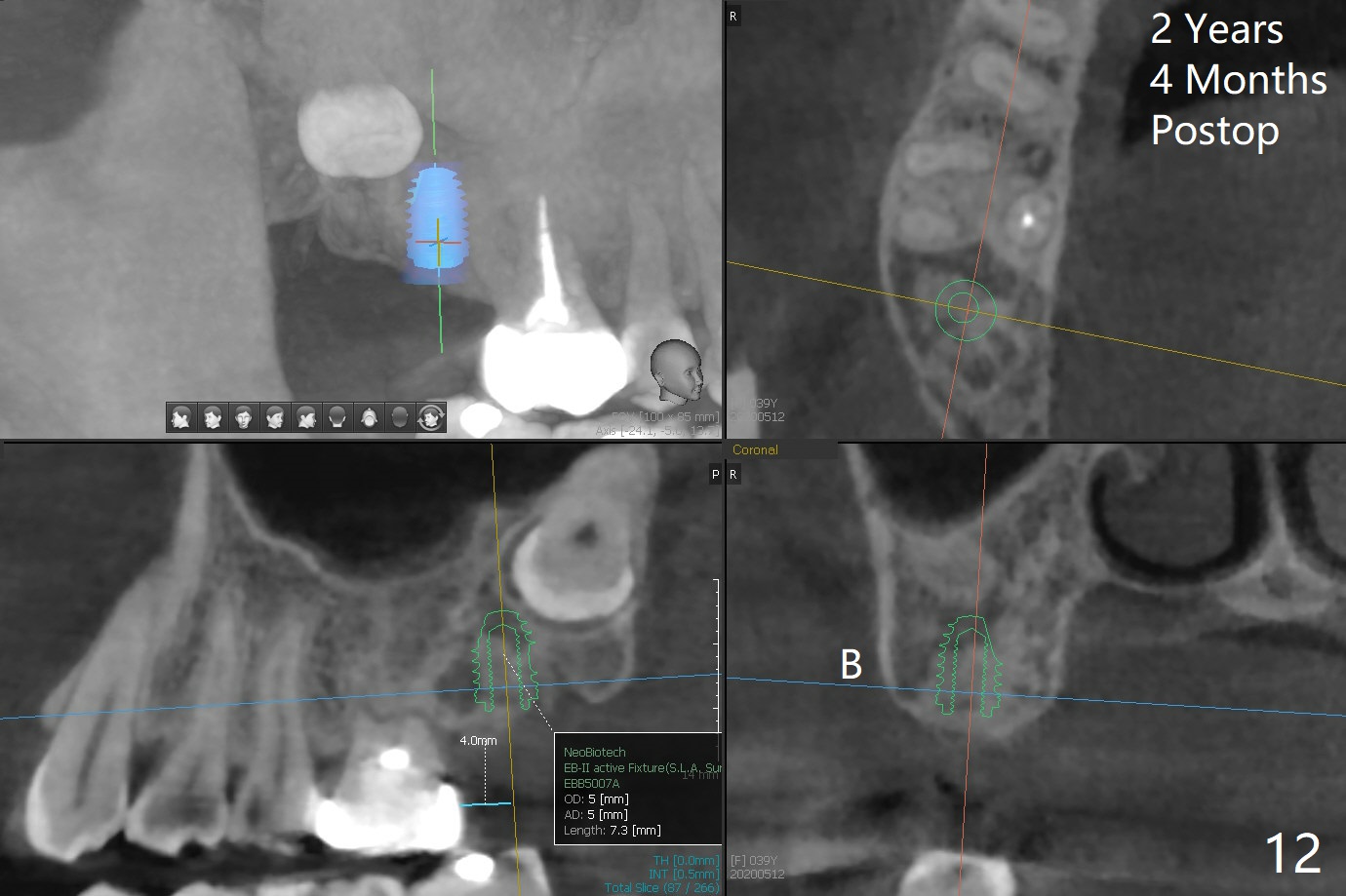
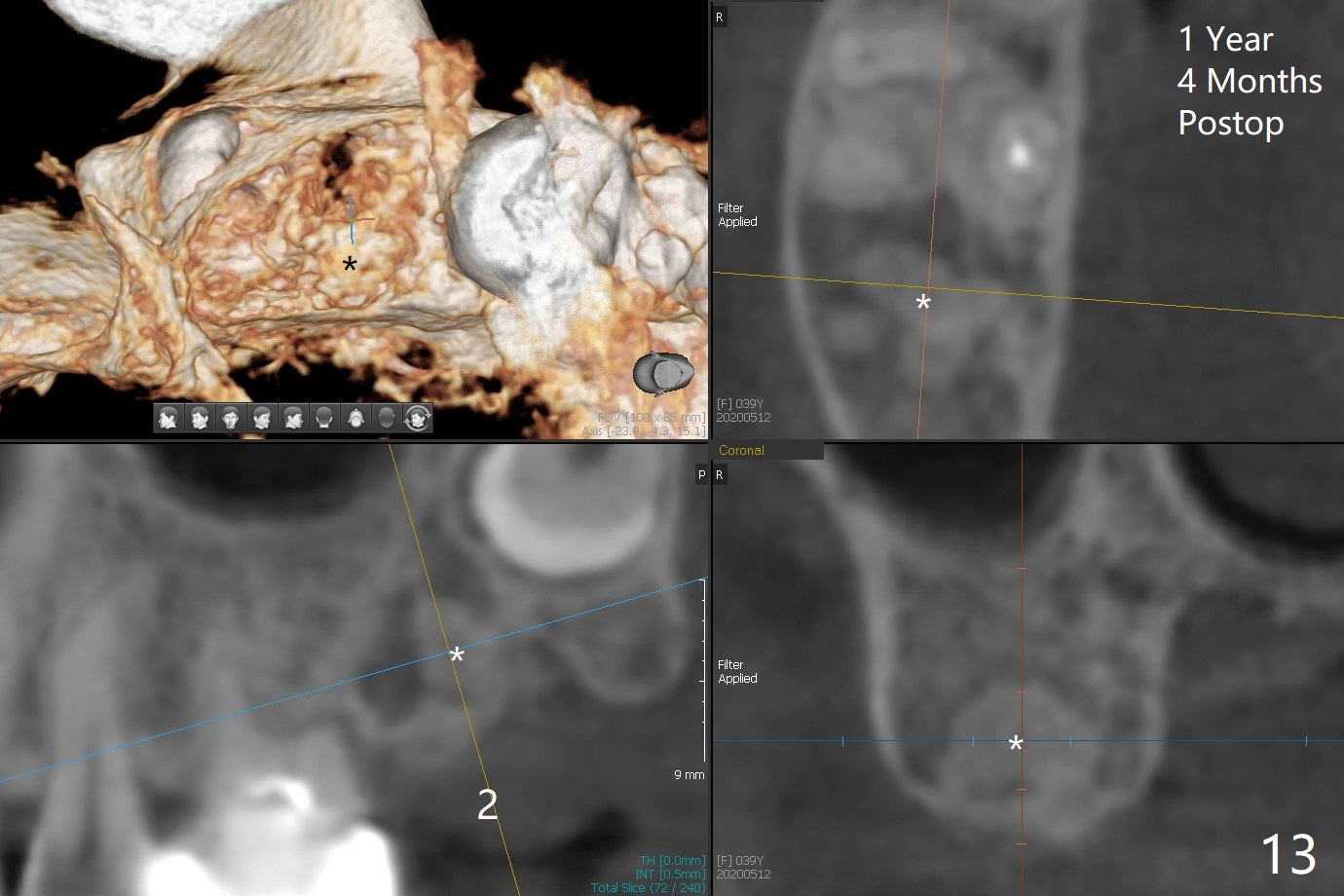
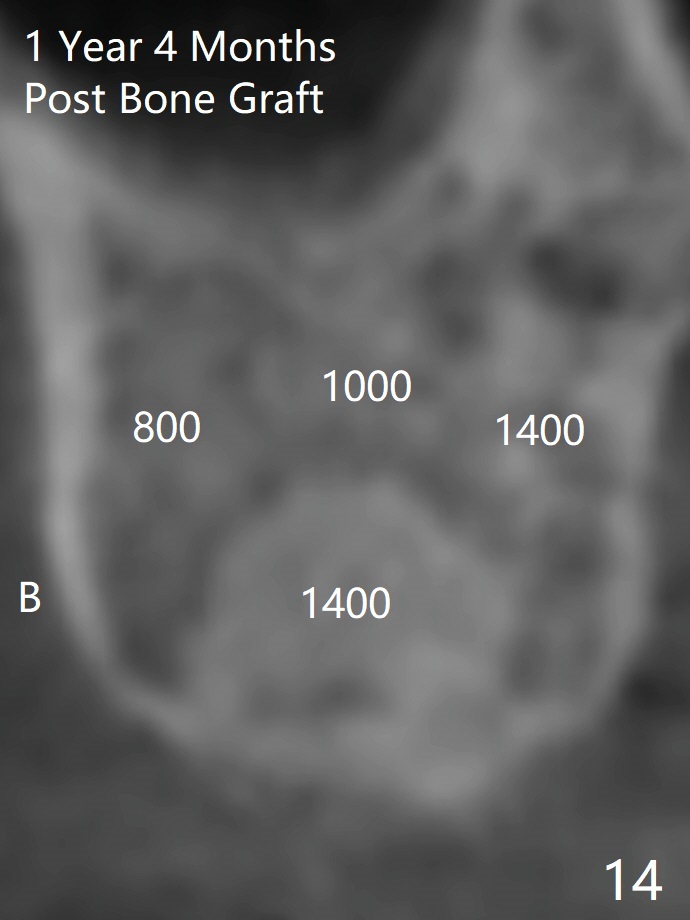
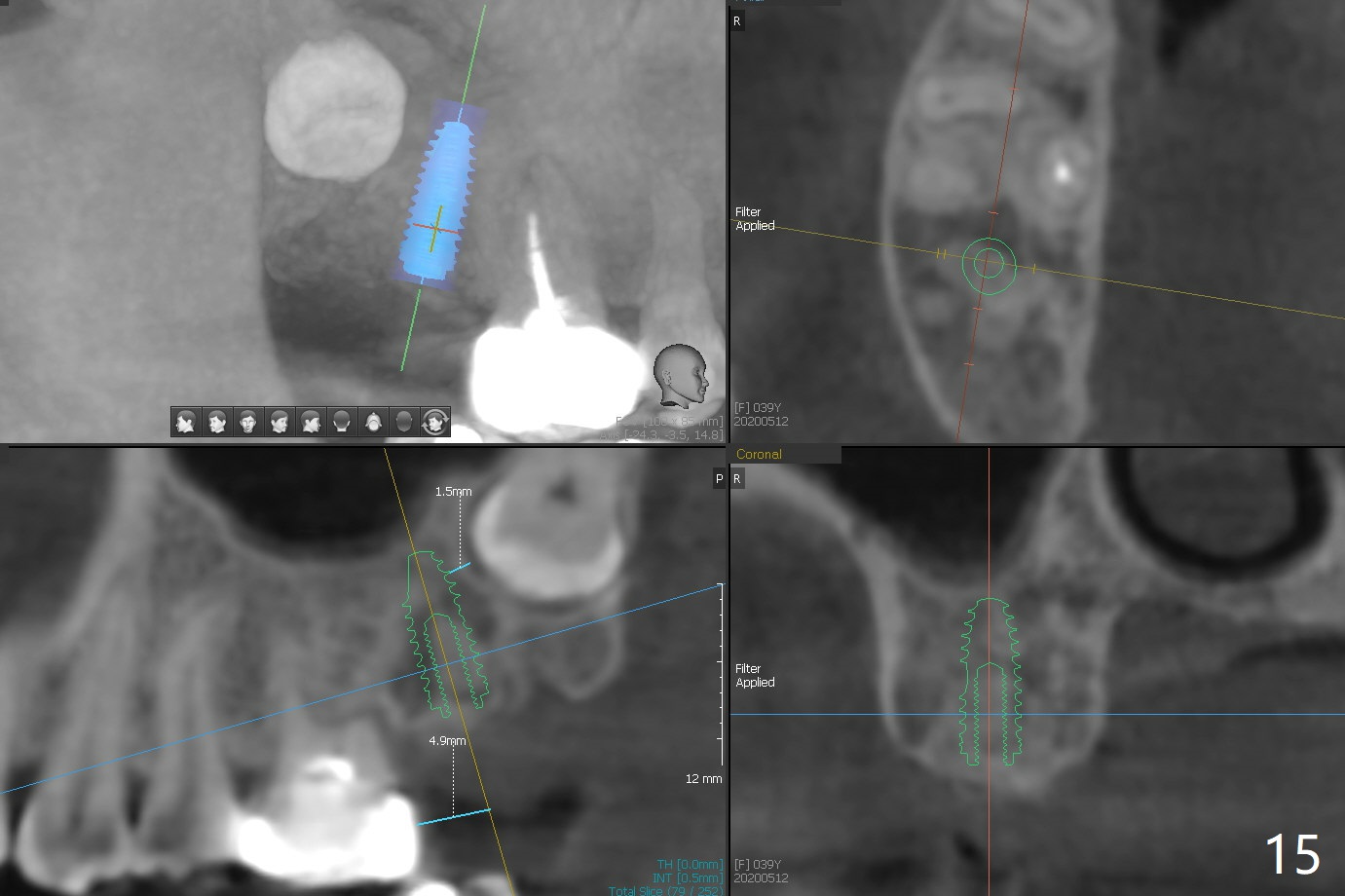
The socket of #2 heals 13 days postop; it appears that the bone graft remains in place (Fig.7,8 *). The patient is instructed to return in 3-4 months for impression and CT for guide. The socket heals 4 months postop (Fig.9,10). She plans to have implant next year, since she wants to add another insurance. The patient returns for implant without removal of the third molar 2 years 4 months post socket preservation (Fig.11). A 5x7.3 mm implant can be placed without invading the sac of the impacted third molar (Fig.12). In fact the lab has a better plan. A lump of bone forms in the previous socket 1 year 4 months postop (Fig.13 *). The ridge is wide and dense (Fig.14). A narrow implant placed oblique could be longer (Fig.15), as compared to a wide, short one (Fig.12).
Return to
Upper
Molar Immediate Implant,
Trajectory,
Weichat
No
Deviation
Graft or
Not Surgery
位点保存/导板
Xin Wei, DDS, PhD, MS 1st edition
01/15/2019, last revision
11/07/2020