|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|||||
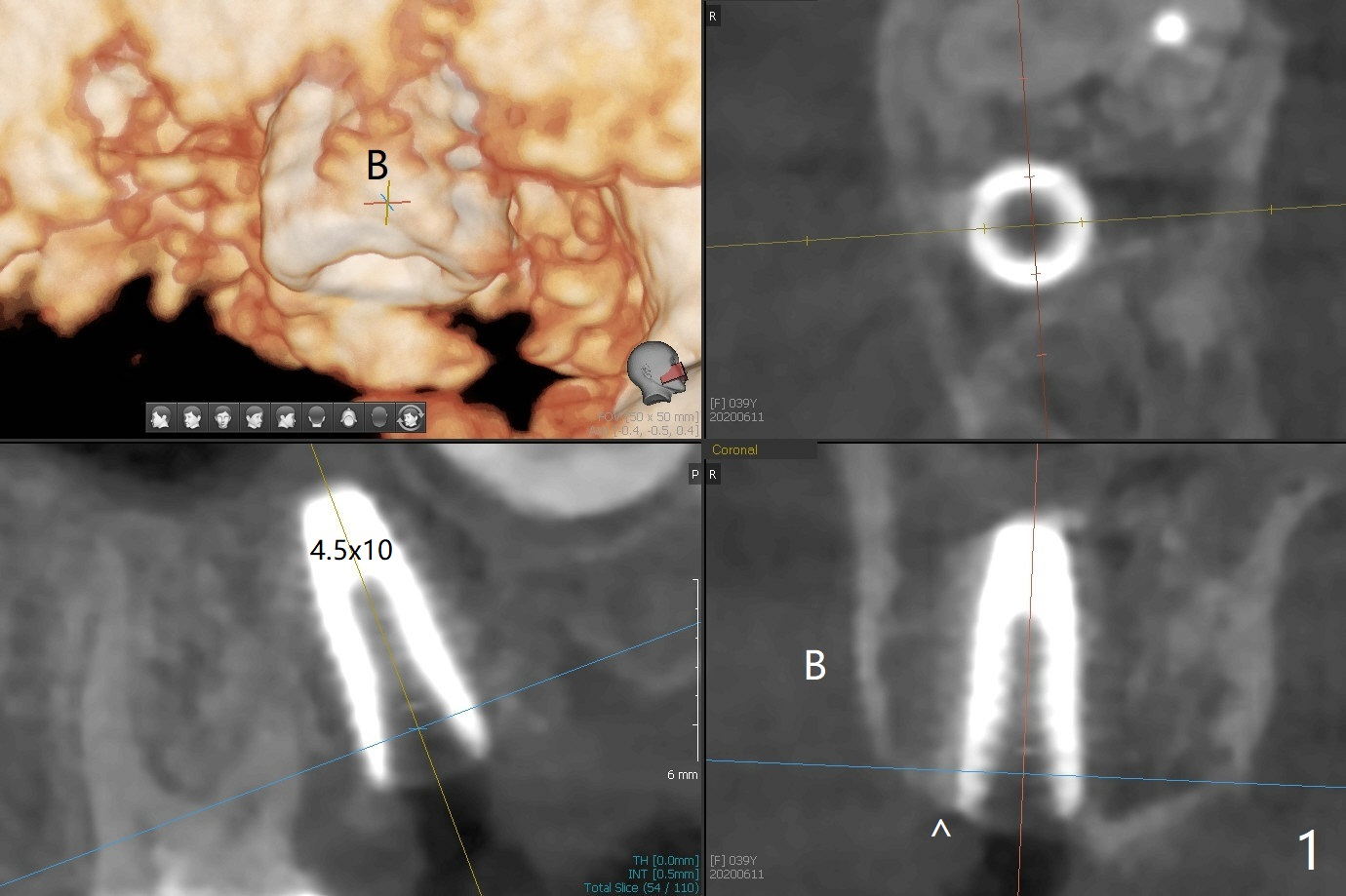
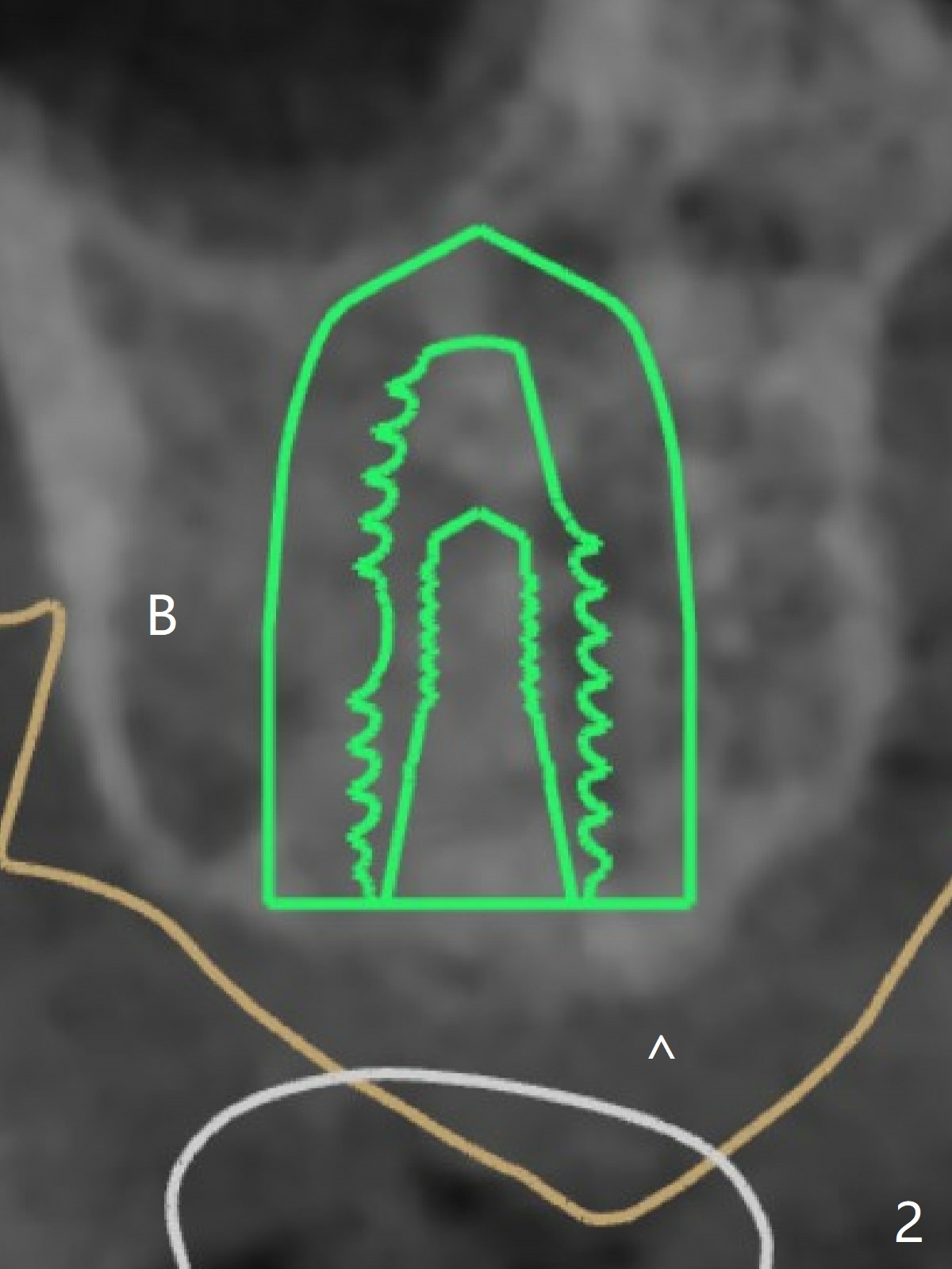
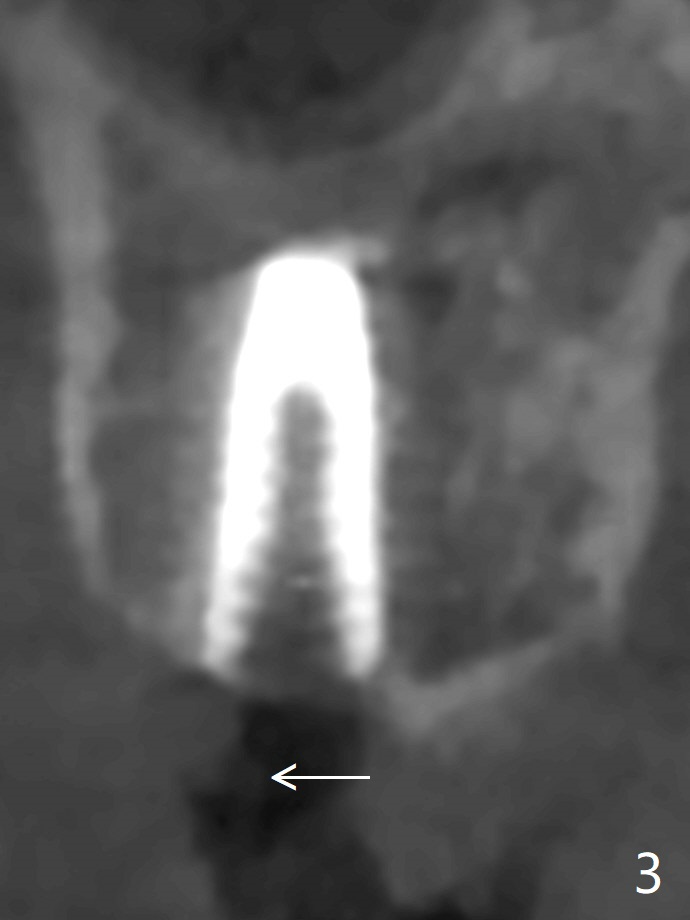
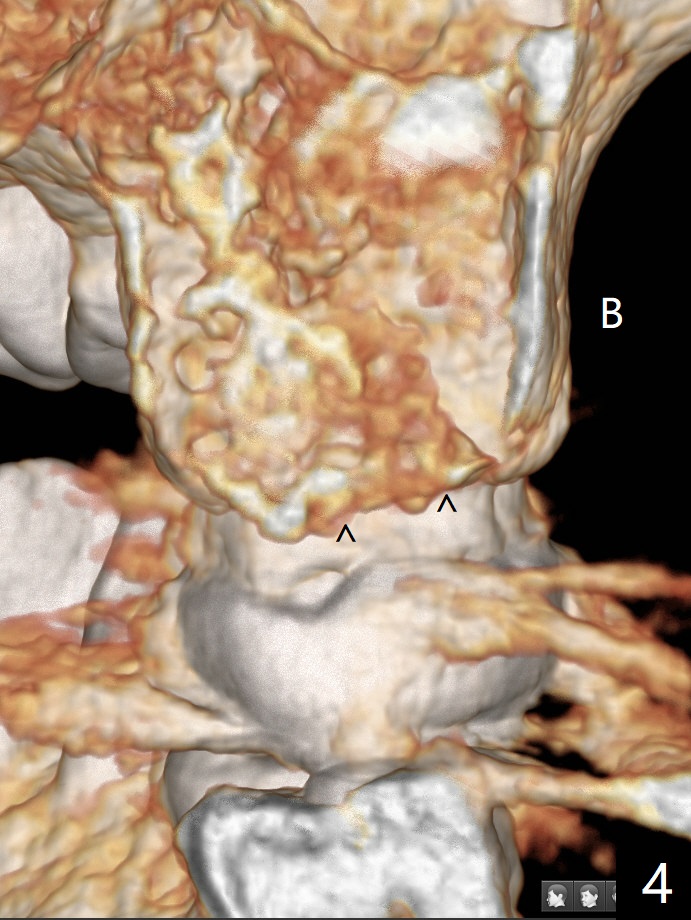
Buccal Slope and Deviation
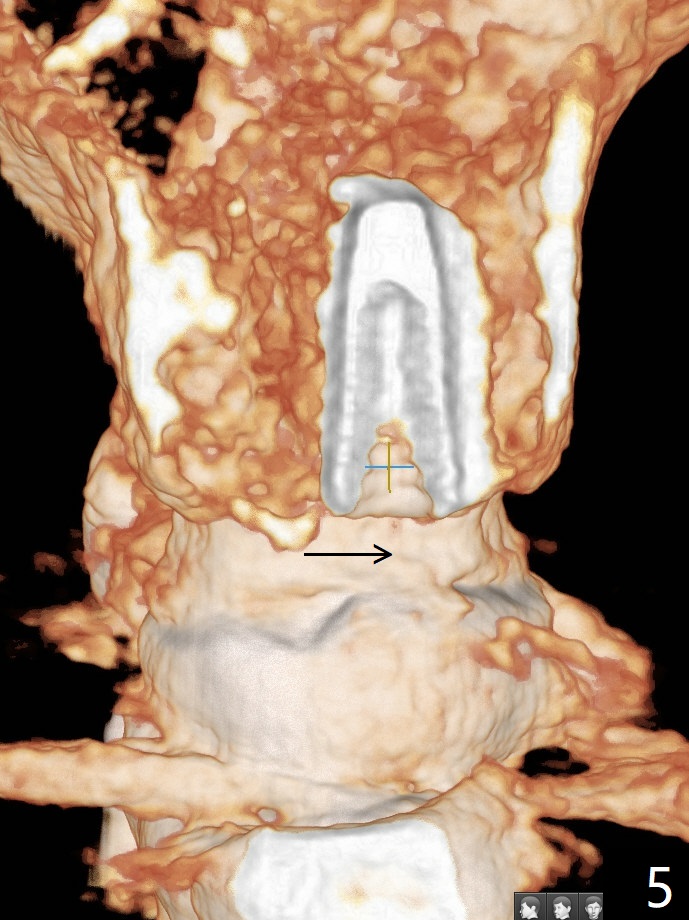
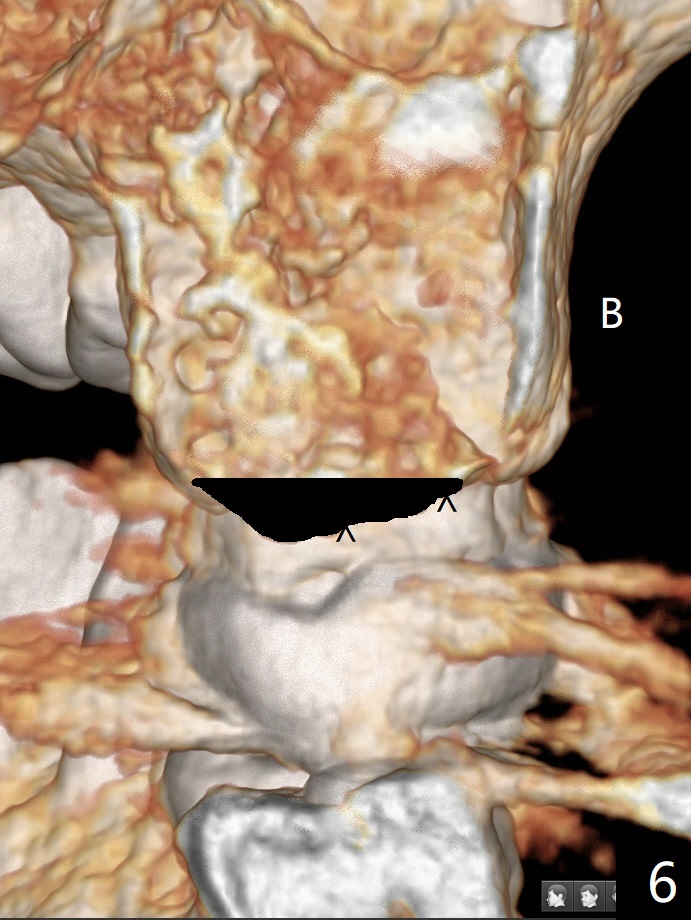
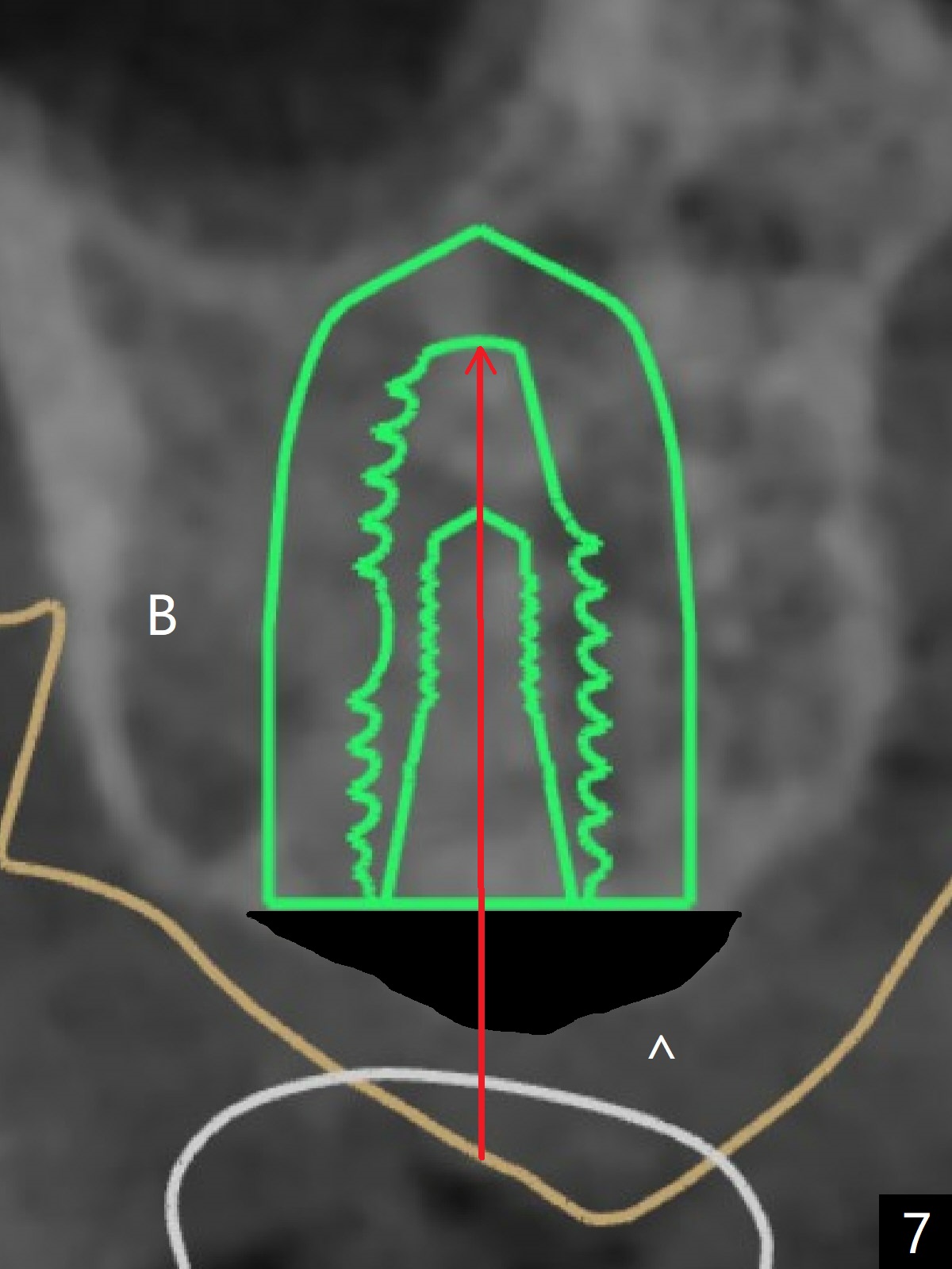
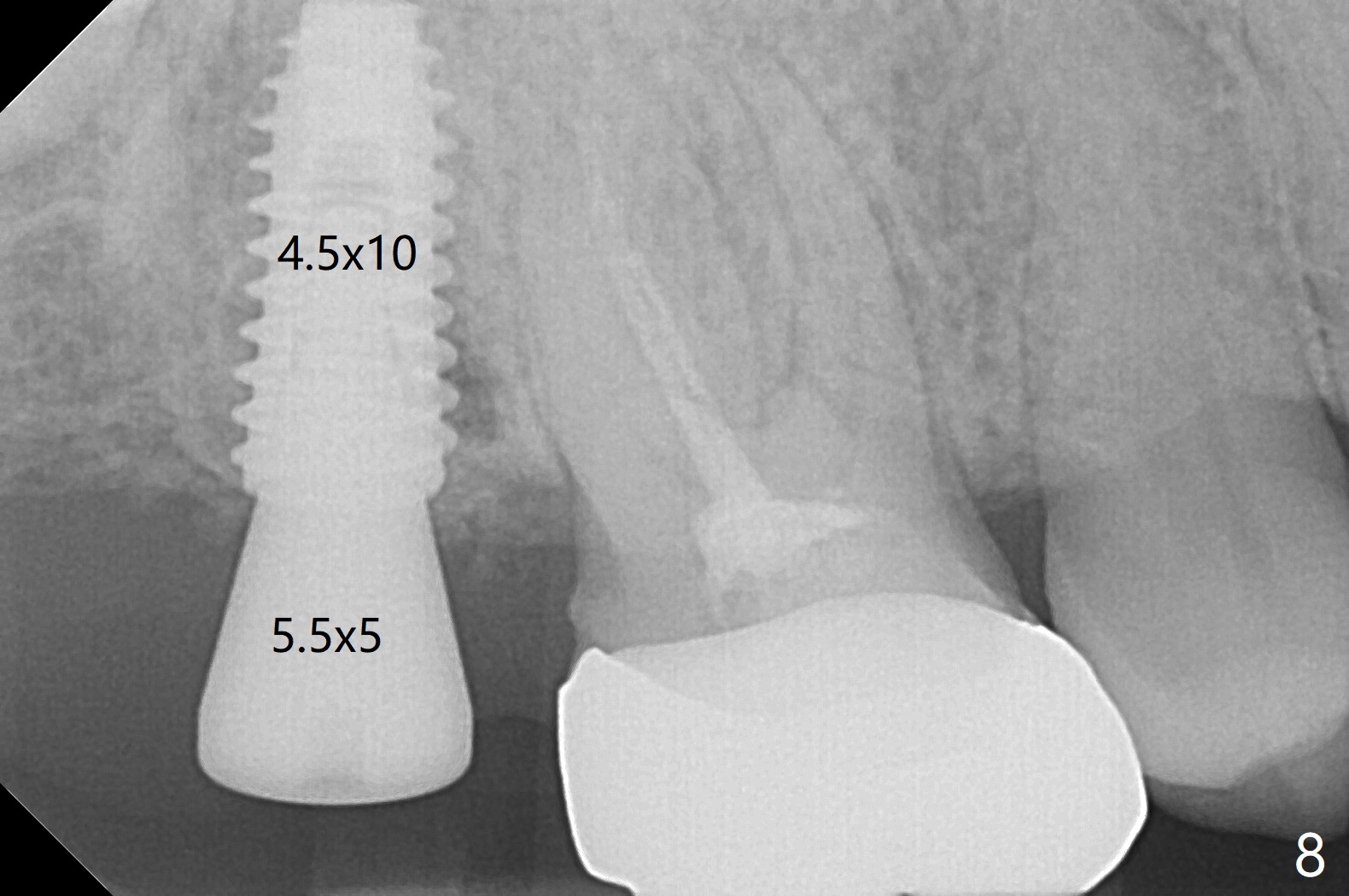
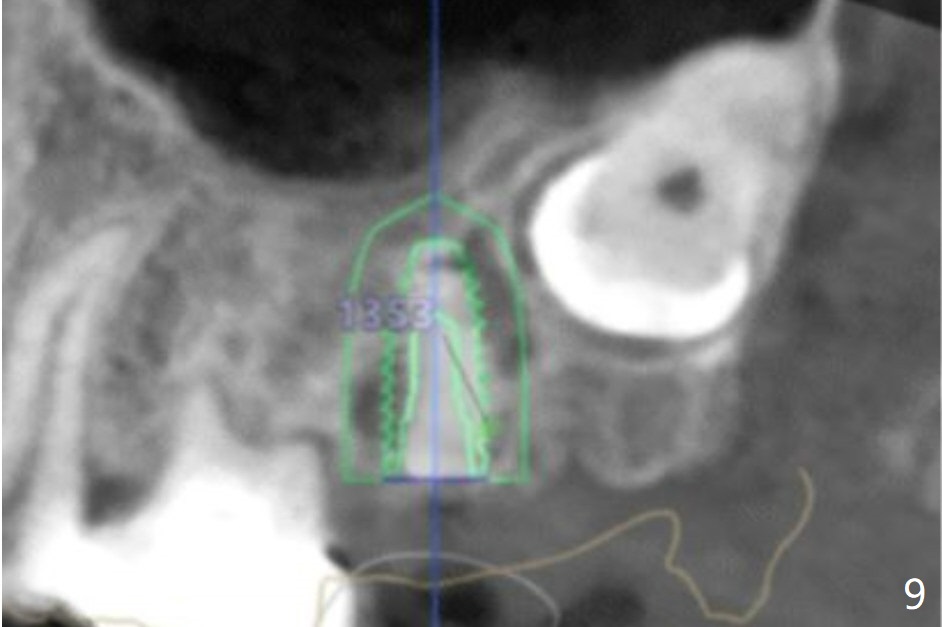
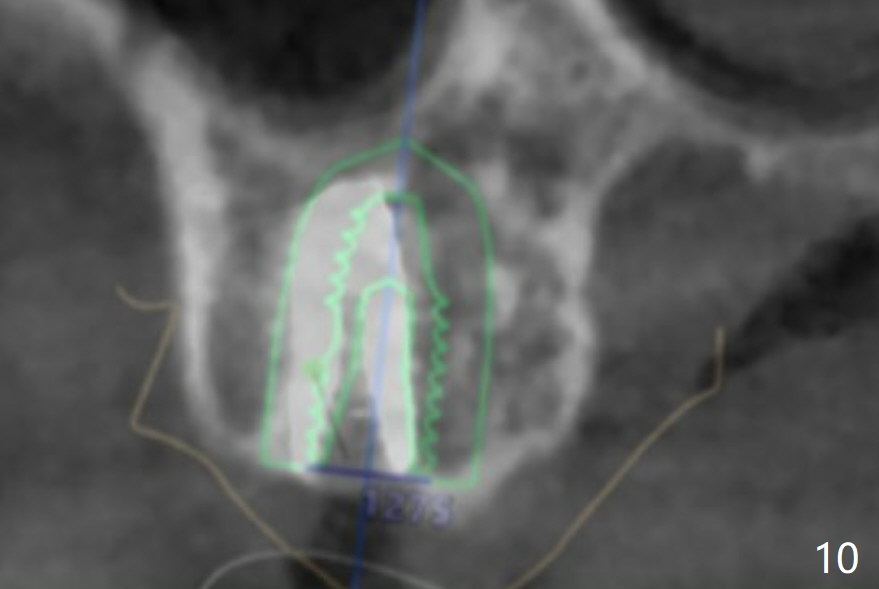
One year 5 months post socket preservation, the ridge looks wide at #2, but there is a buccal slope. A freshly made surgical guide is placed at the site. The mouth opening is limited. Tissue punch, bone trimmer and most of drills have to be placed inside the guide before delivering into the mouth. The 10.5 mm bone trimmer is difficult to use. With heavy pressure, it goes down anyway. When a 4.5x10 mm implant is placed, the guide is removed. The implant seems to be buccally placed. More importantly the buccal crest cannot be probed. CT is taken: the implant is equicrestal buccal (Fig.1 ^). As compared to the design (Fig.2), the implant deviates buccal (Fig.3 arrow). The lowest point of the ridge is palatal (Fig.2 ^). That is the buccal portion of the ridge is not even (Fig.4 arrowheads). During osteotomy, drills inadvertently deviates buccal (1400 units), resulting in buccal deviation of the implant (Fig.5 arrow). To overcome the deviation, the ridge has to be exposed by incision. The pointed ridge should be flattened using surgical bur (Fig.6), since the bone trimmer may wobble in the slope and cannot even the ridge. With surgical precision flattening with visual confirmation, the following osteotomy should be able to be maintained as straight as planned (Fig.7). For this case, the guide is reloaded and the implant is placed ~ 1 mm deeper, followed by a 5.5x5 mm healing abutment (Fig.8). Overlapped images of design vs. postop shows that the implant trajectory is normal mesiodistal (Fig.9) and deviated buccopalatal (Fig.10).
Return to No Deviation 位点保留后 位点保存/导板
Xin Wei, DDS, PhD, MS 1st edition 06/11/2020, last revision 11/07/2020