
|
|
|
|
|
|
|
|
|
|
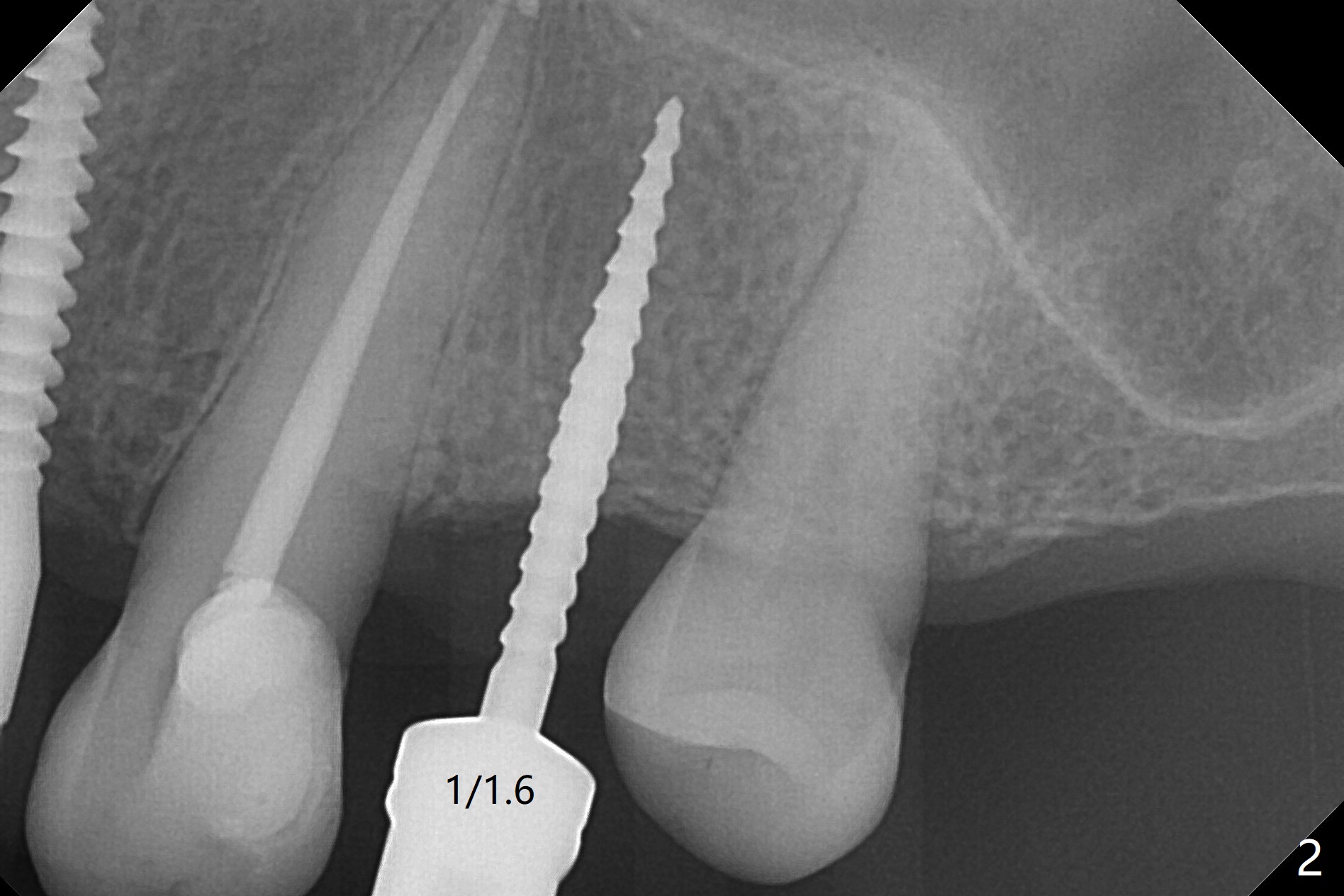
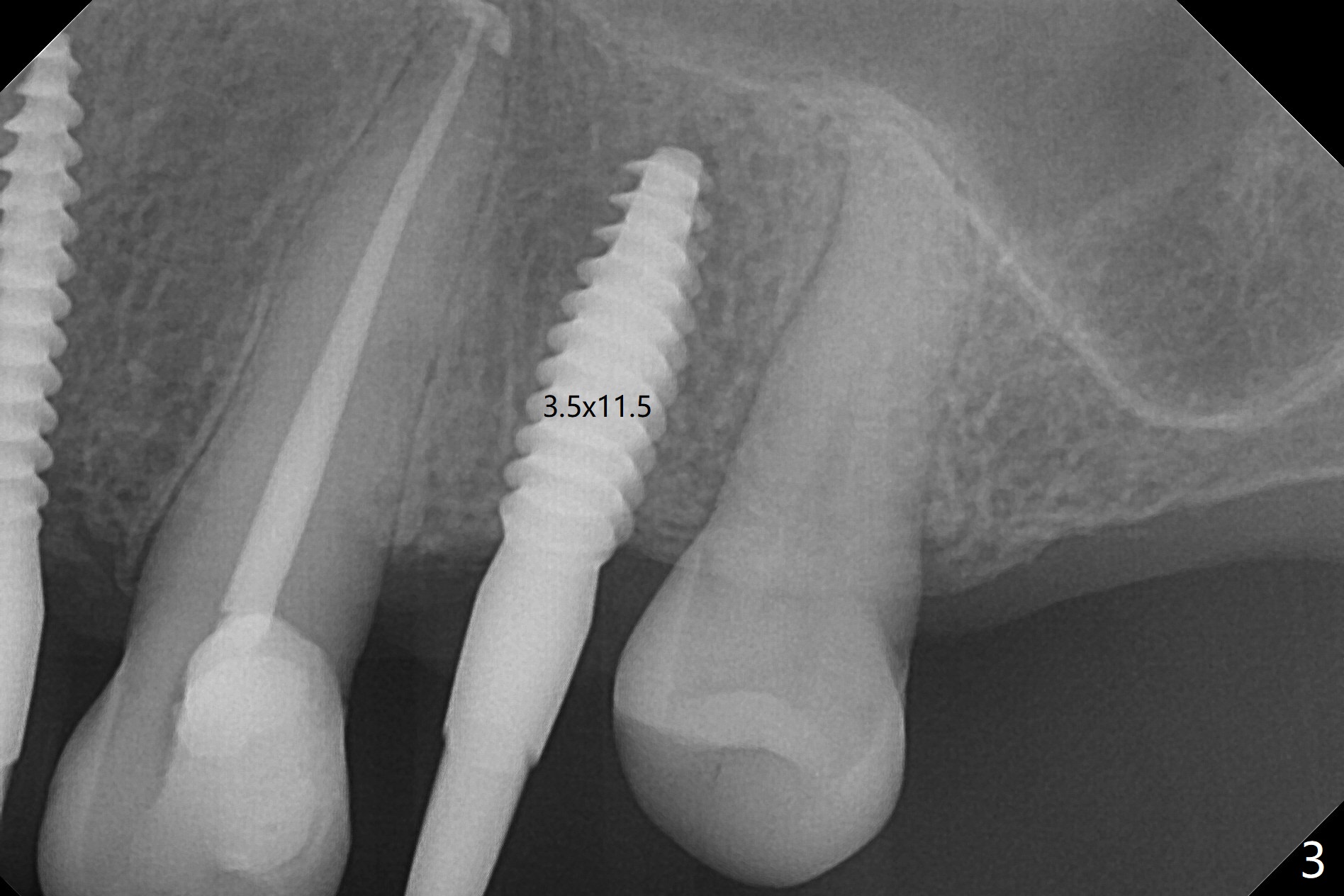
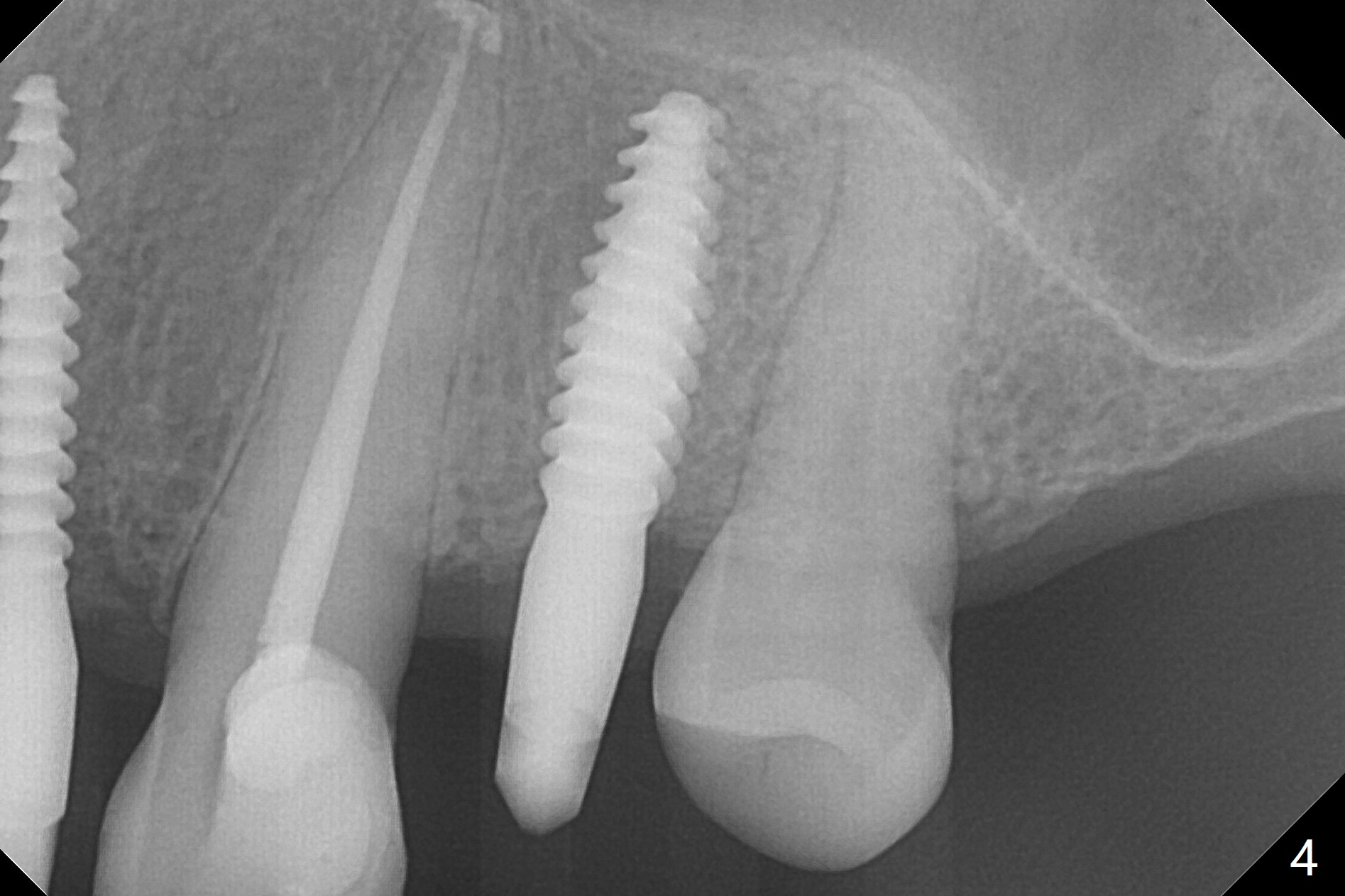
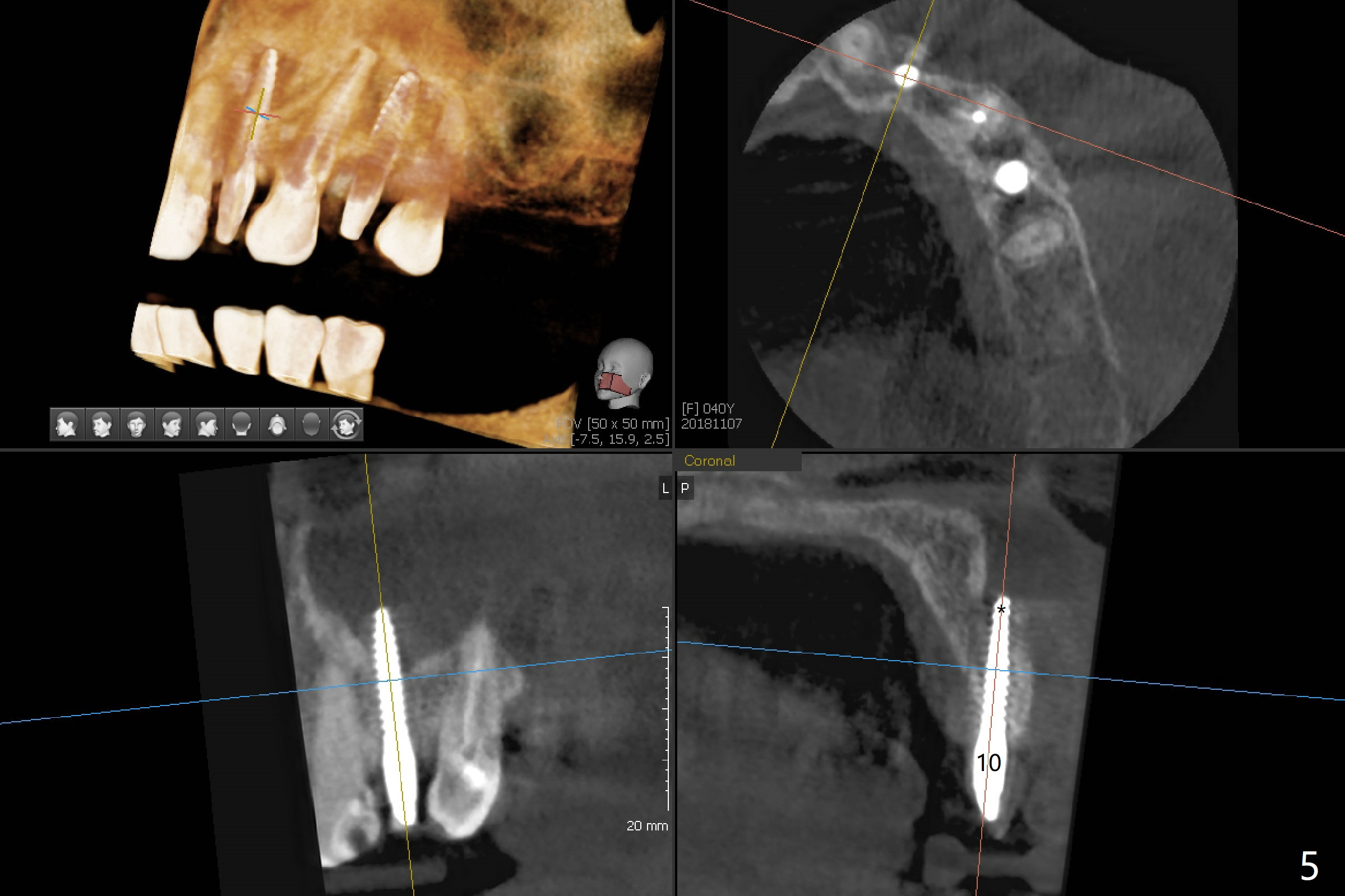
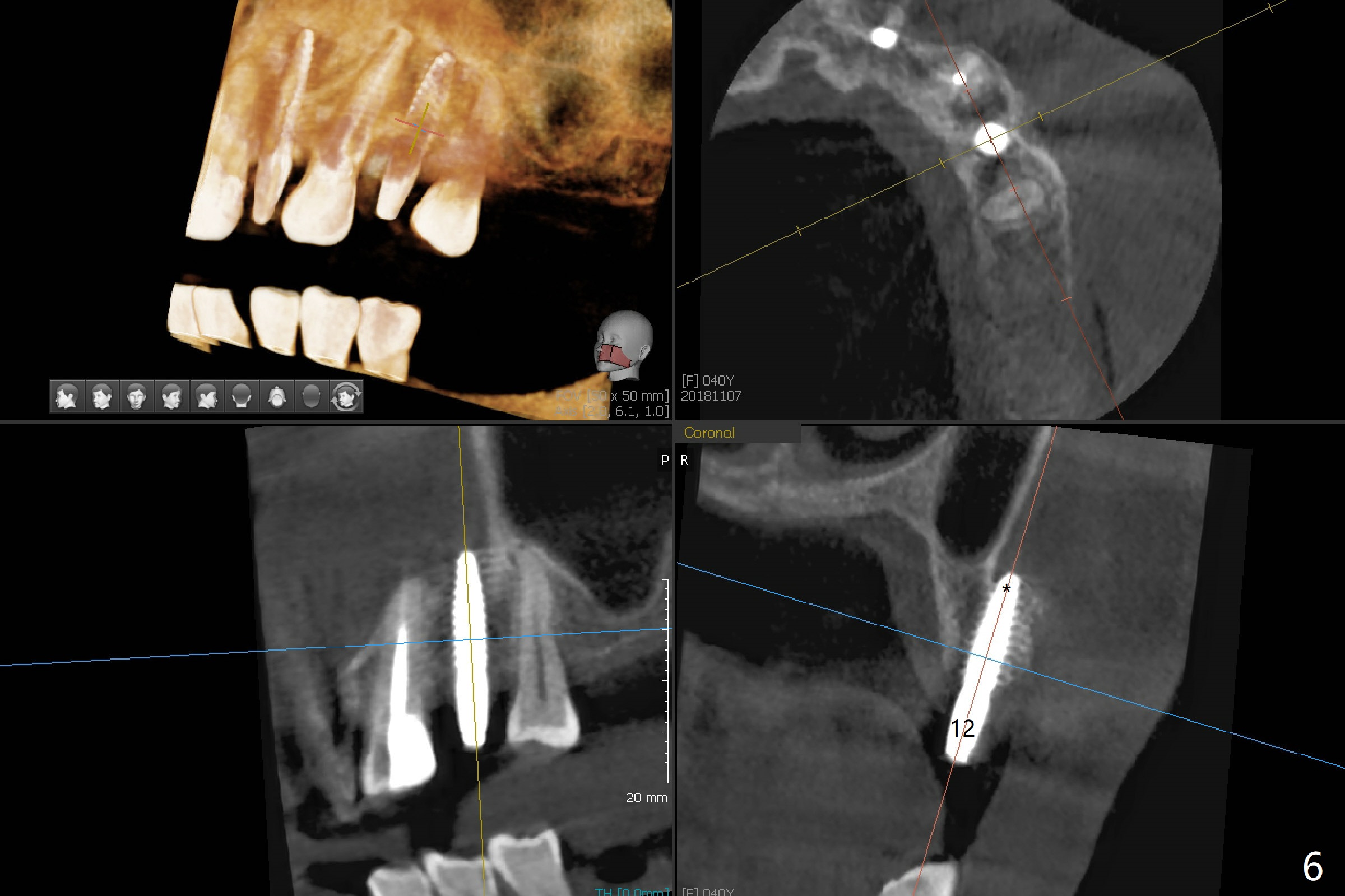
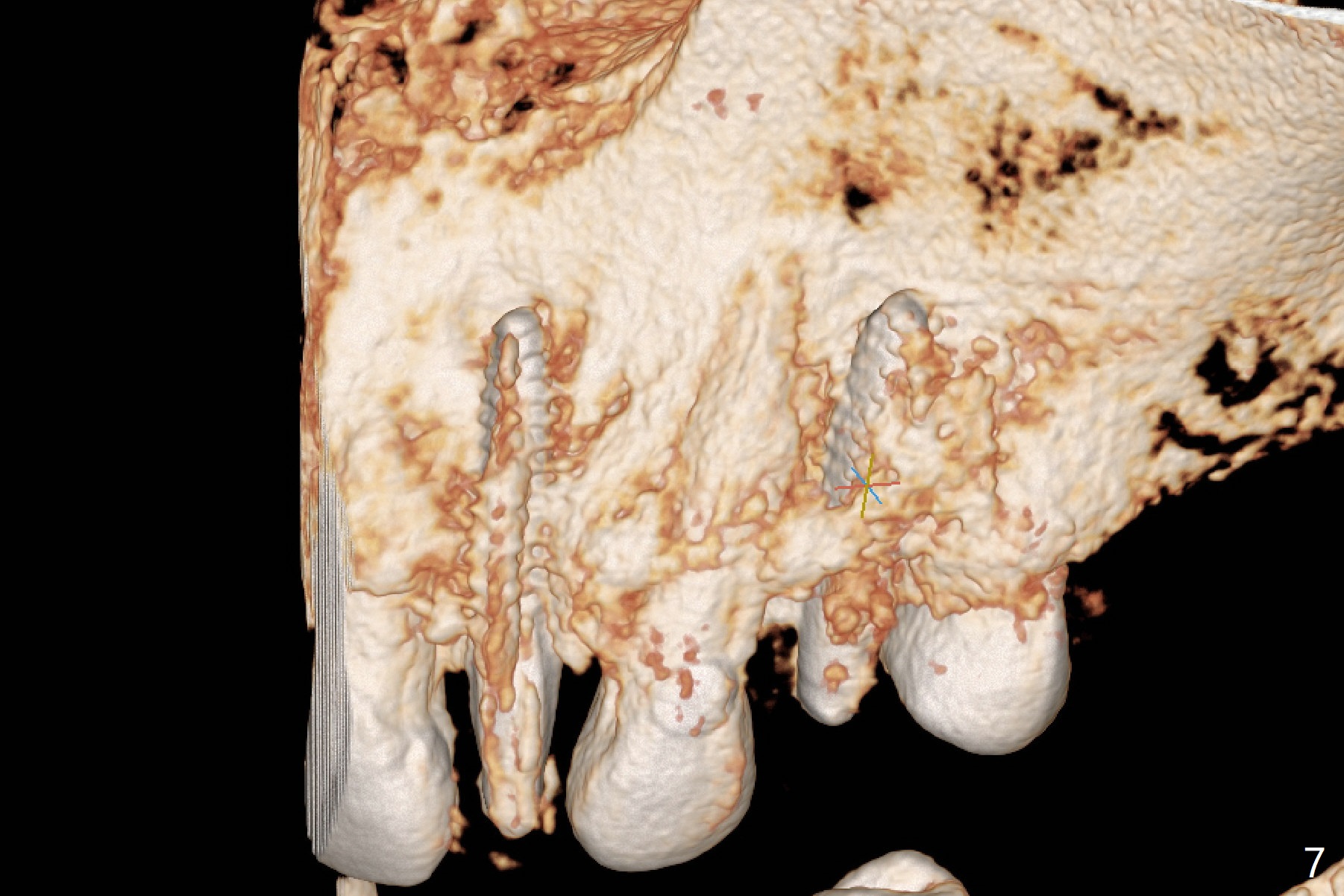
Buccal Perforation
After removal of #10 sleeve and 3 spot adjustment, the guide is seated without satisfaction. When the guide is removed after pointed drill, the osteotomy seems distal (Fig.1). Incision is made with flap elevation for free hand osteotomy. A 1/1.6 mm bone expander is inserted after 1.2 mm drill, the trajectory appears to be right (Fig.2). As the osteotomy increases in diameter, the buccal plate feels to be vibratory. A 3.5x11.5 mm 1-piece implant placed initially is apparently away the sinus floor (Fig.3). Further placement (subcrestal, Fig.4) seems to be associated with more buccal plate perforation (Fig.6 *), which is repaired by bone graft. Since the implant at #10 appears to be doing okay 1.5 months postop (Fig.5), the implant at #12 is not removed immediately. A tunnel incision will be made for bone graft in the most apical concave areas (Fig.7). The osteotomy should have been made more palatal to reduce the chance of the buccal perforation. CBCT should have been taken while the 1/1.6 bone expander was in place.
Return to Upper Premolar Immediate Implant, Trajectory Xin Wei, DDS, PhD, MS 1st edition 11/07/2018, last revision 11/18/2018