|
|
|
|
|
|
|
|
Sinus Membrane Repair
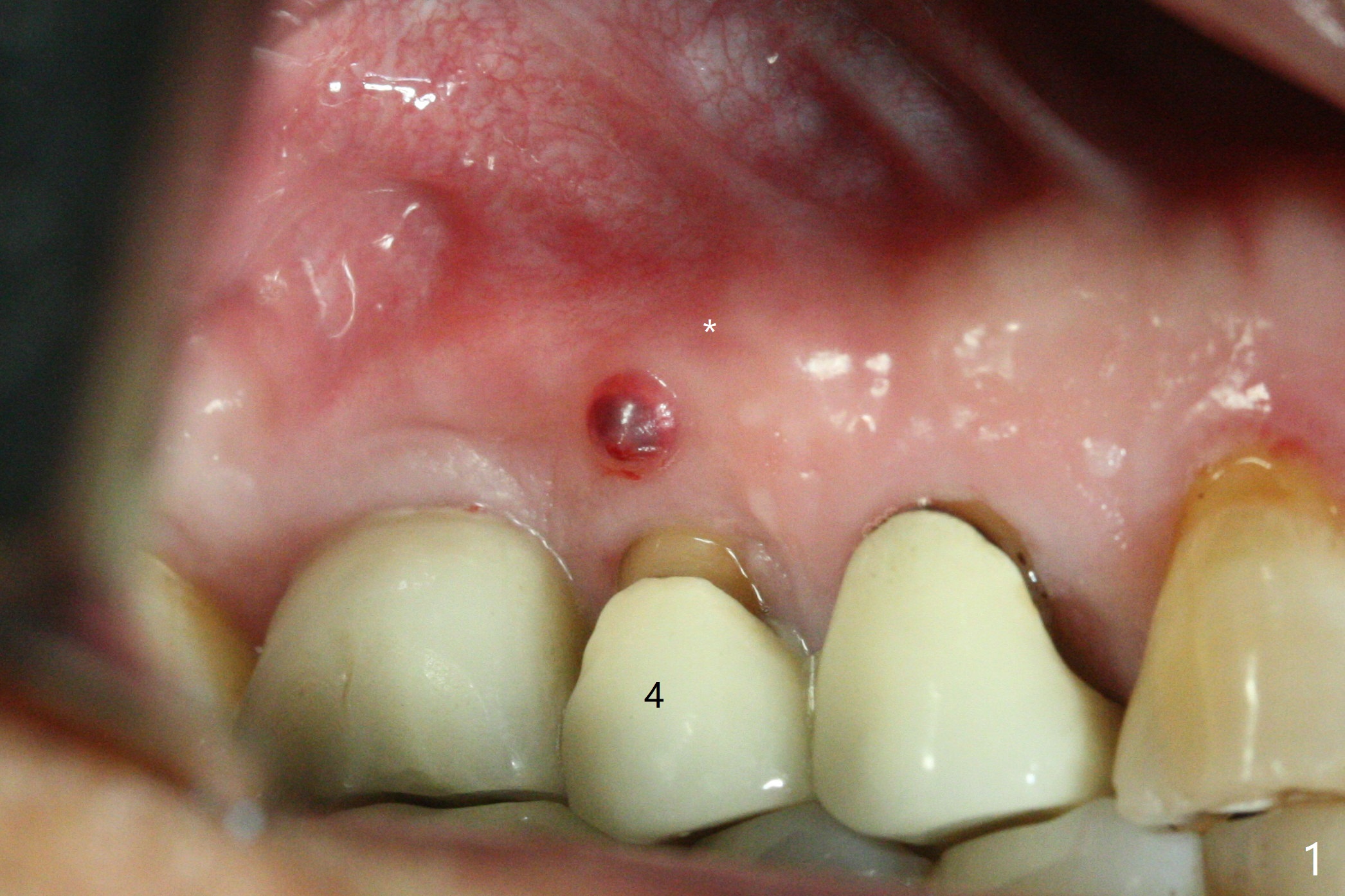
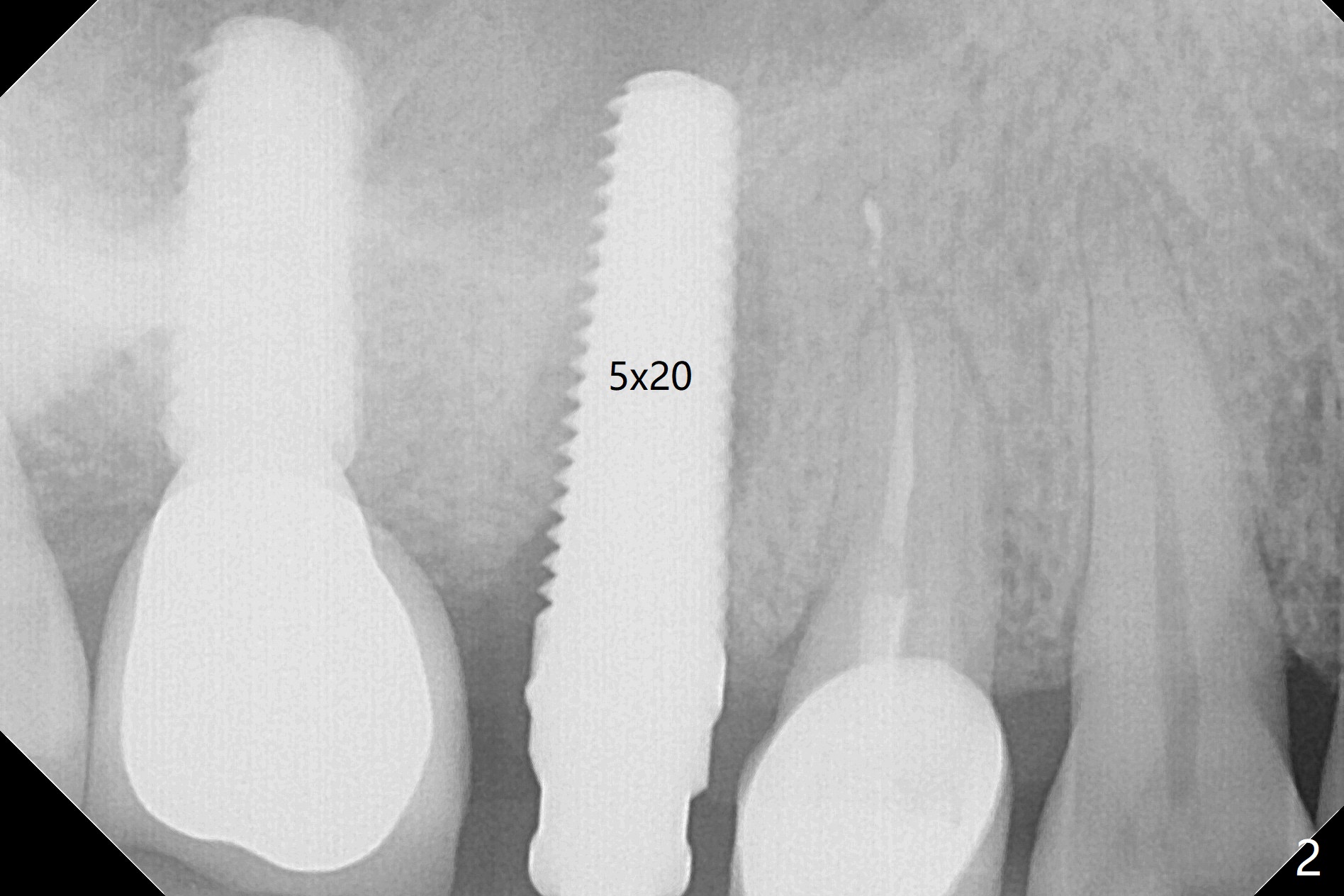
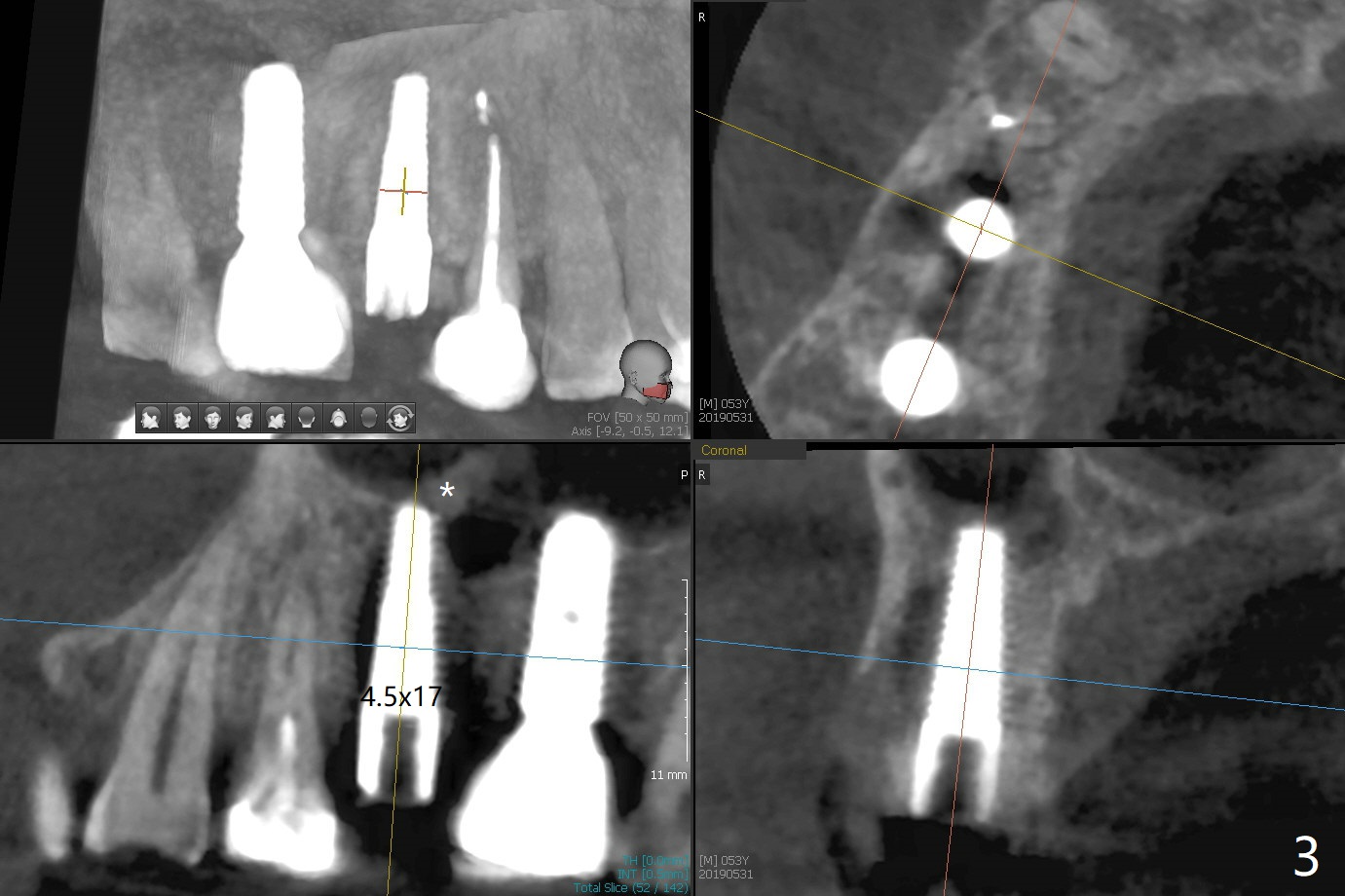
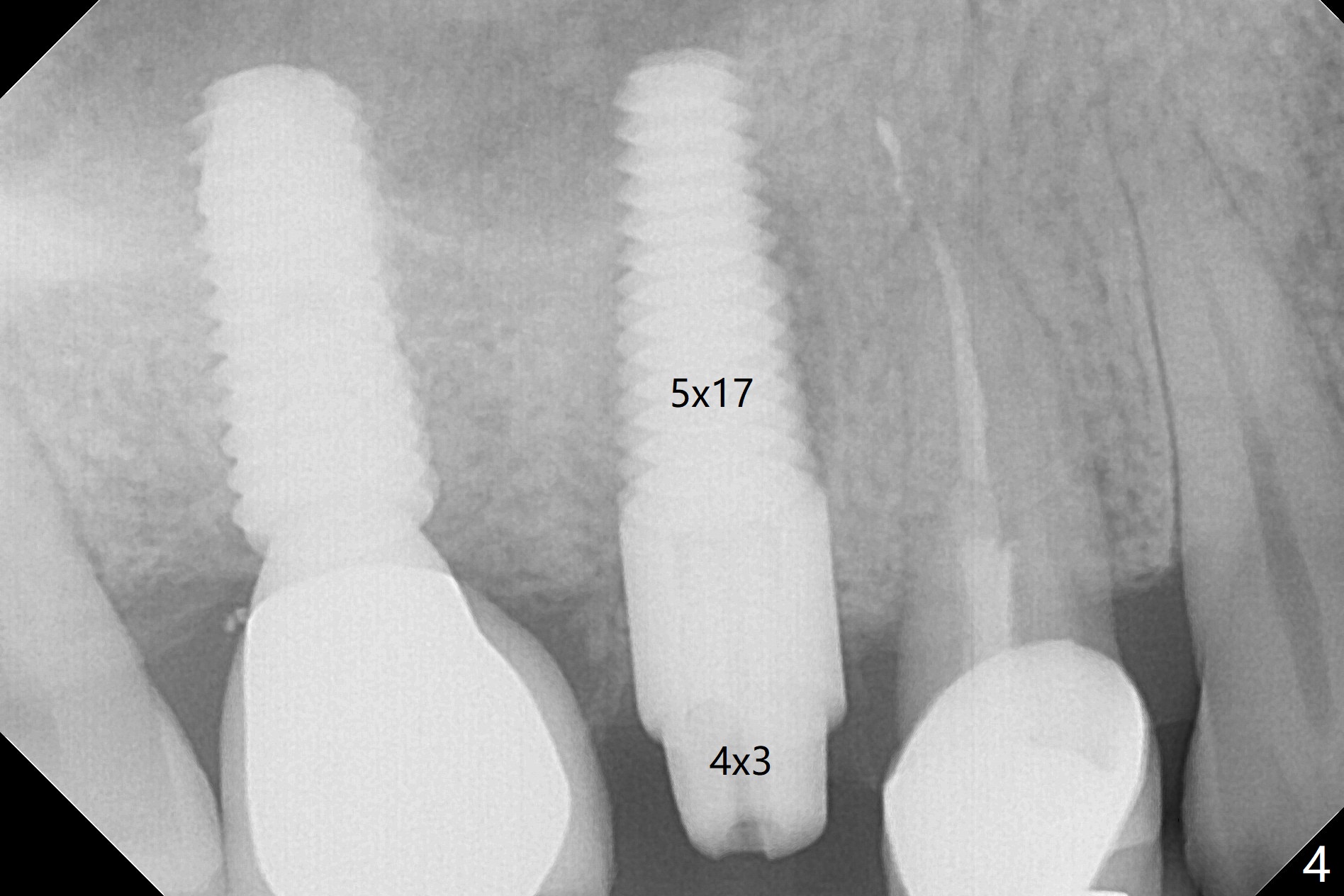
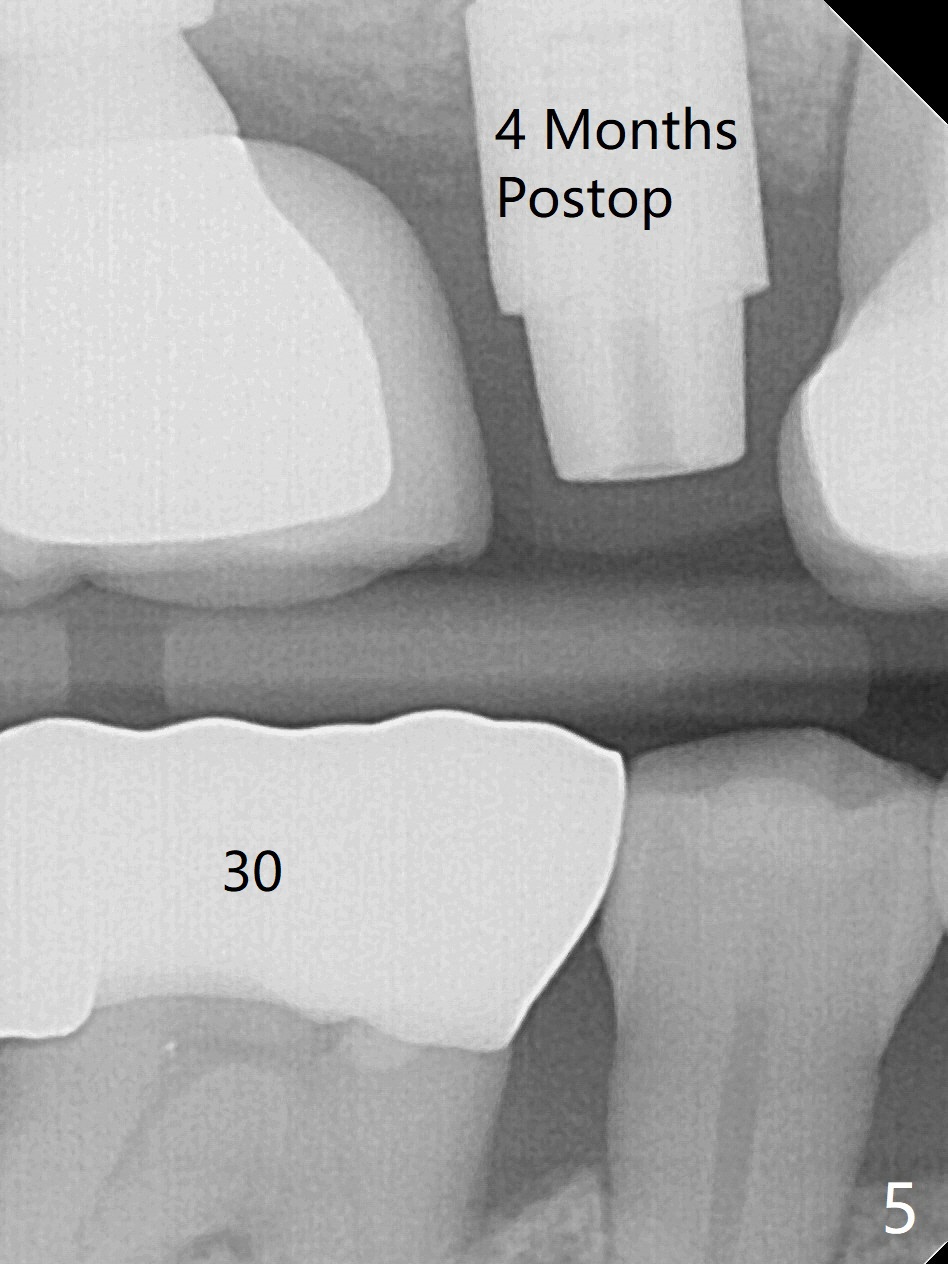
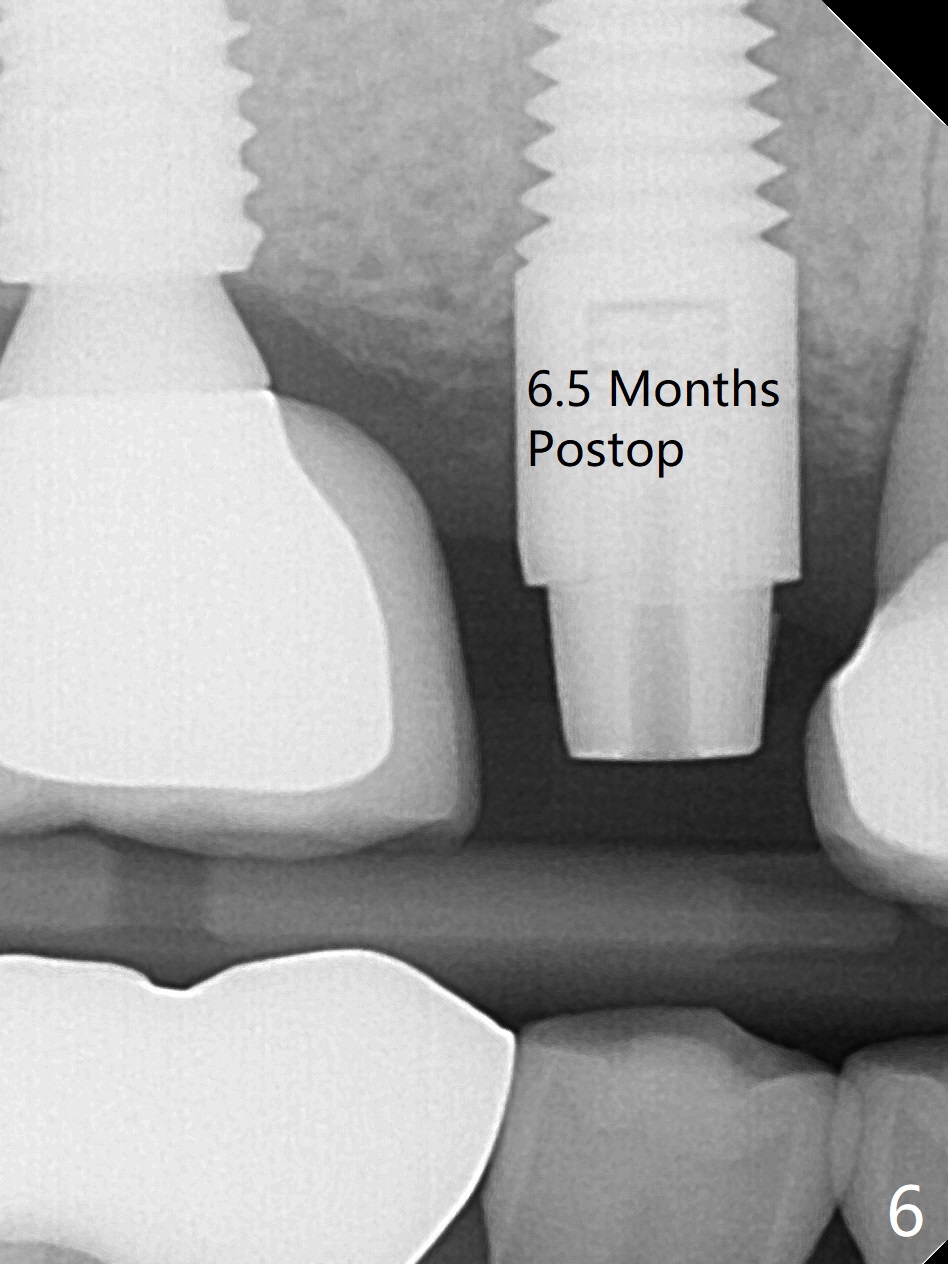
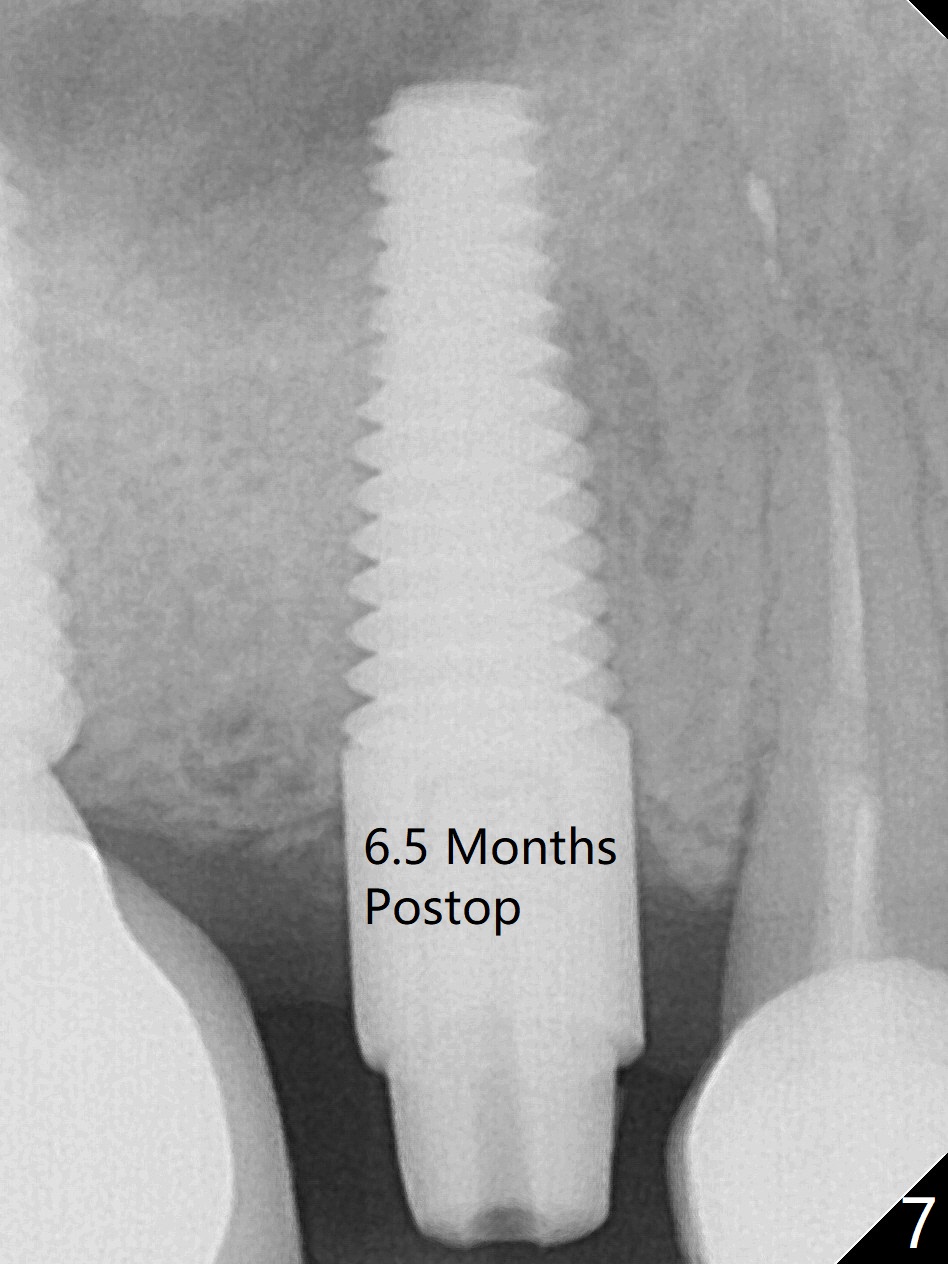
In spite of a fistula at #4, the buccal plate is present because of the exostosis (Fig.1 *). Since the socket is long and narrow, it is difficult to initiate osteotomy in the distal slope. Since the buccal plate is low, osteotomy is established as palatal as possible. The sinus floor is thin, but hard to elevate with Magic Sinus Lifter. Use of 3 mm Magic Expander leads to sinus floor break through and membrane perforation. After increase in the osteotomy with sequential expanders, a 5x20 mm tap is inserted with stability (Fig.2). Two pieces of PRF membrane are inserted for sinus membrane repair, followed by small amount of allograft (mixed with PRF, Fig.3 *) and a 4.5x17 mm dummy implant. A 5x17 mm tissue level implant is placed with >45 Ncm; with immediate placement of a 4x3 mm abutment (Fig.4), an immediate provisional is fabricated. There is no postop nasal hemorrhage. The immediate provisional has occlusal perforation 1.5 months postop. The tooth #13 has mobility due to its overuse and missing the teeth #14 and 18. Bitewing taken while redoing crown for #30 shows that the implant threads are subcrestal (Fig.5). There is no crestal bone resorption 6.5 months postop (Fig.6,7), while the periradicular radiolucency decreases (Fig.7).
Return to Upper Premolar Immediate Implant, Trajectory Limited Ortho Xin Wei, DDS, PhD, MS 1st edition 05/31/2019, last revision 06/08/2020