

|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
||
Improve
Crown/Implant Ratio
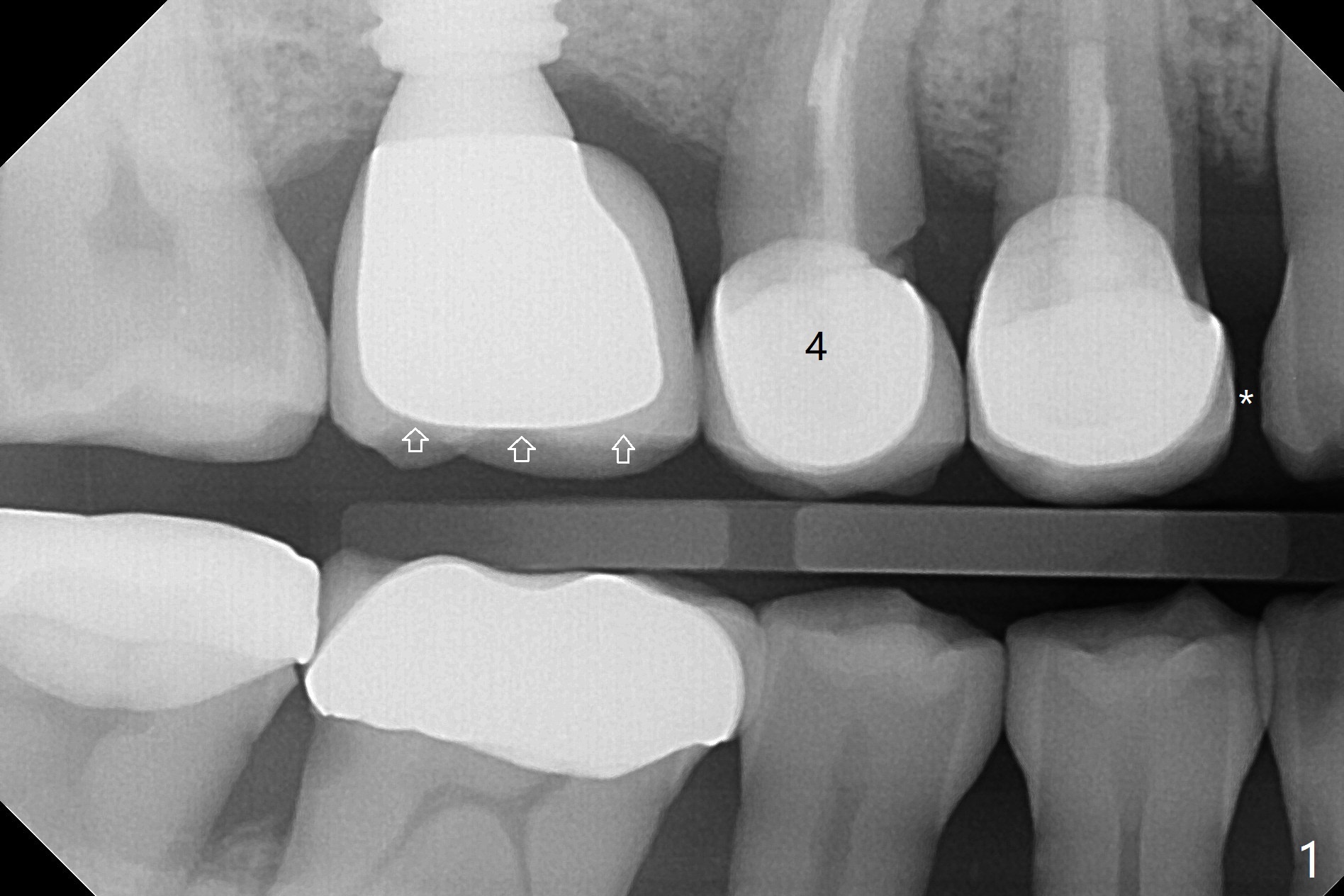
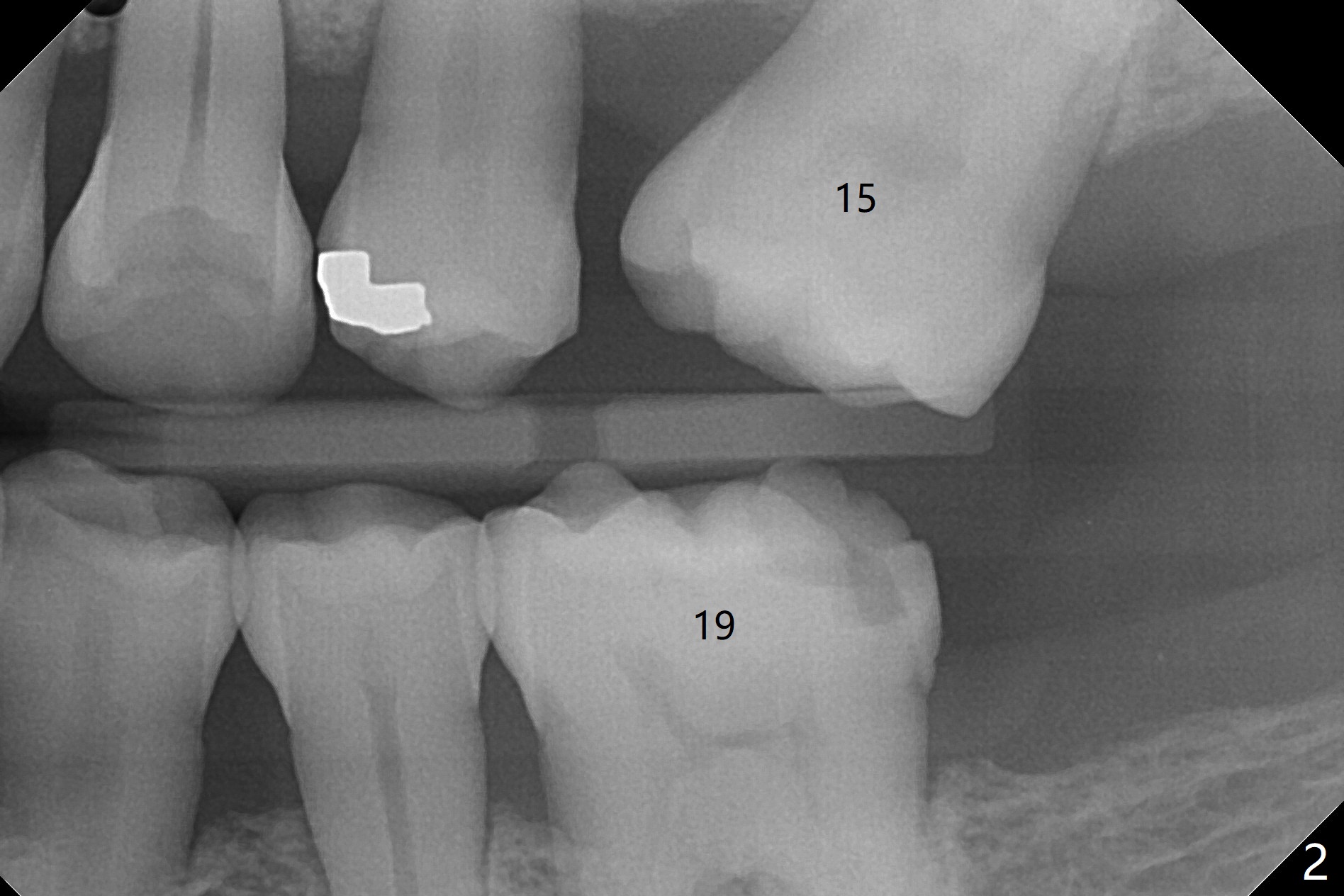
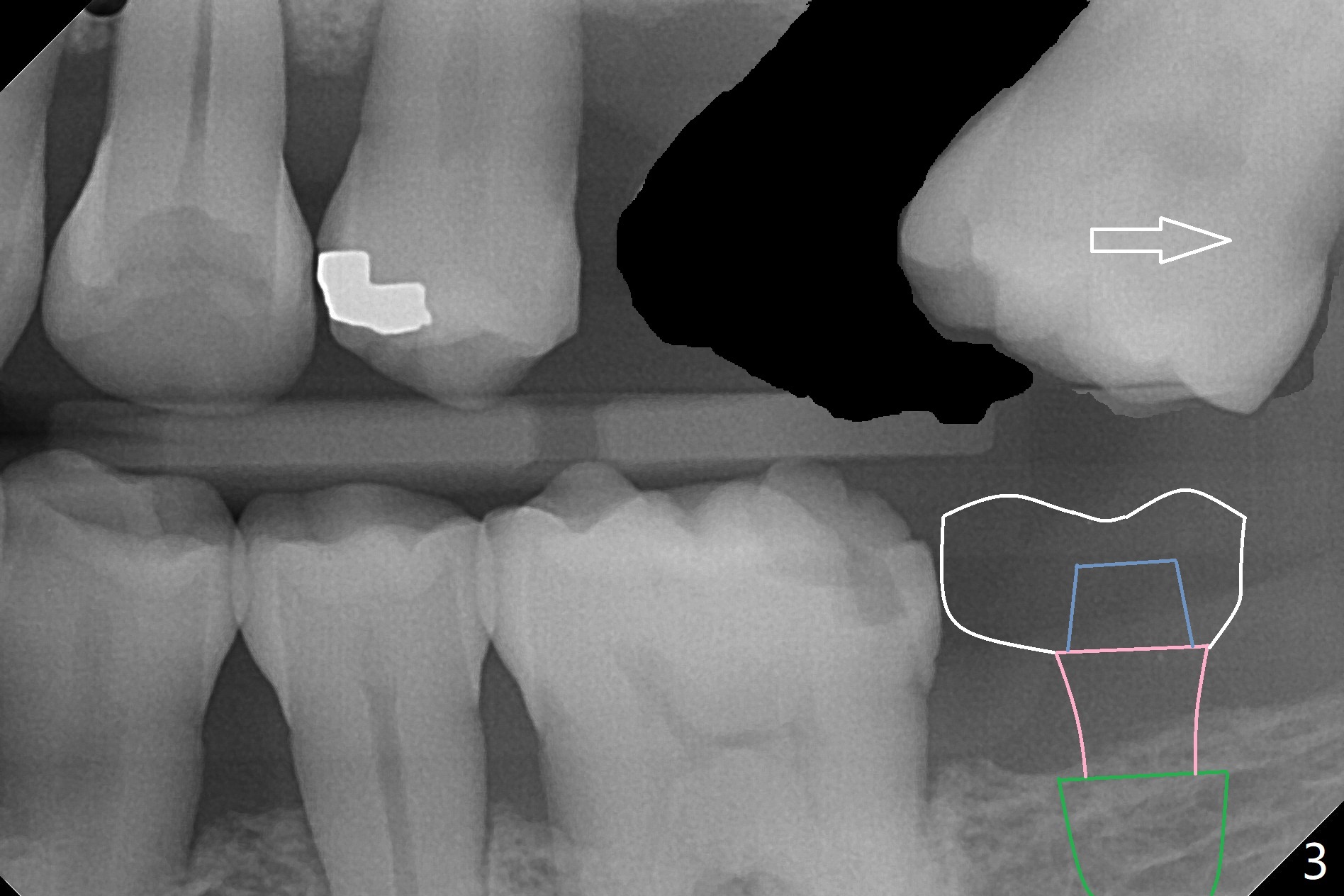
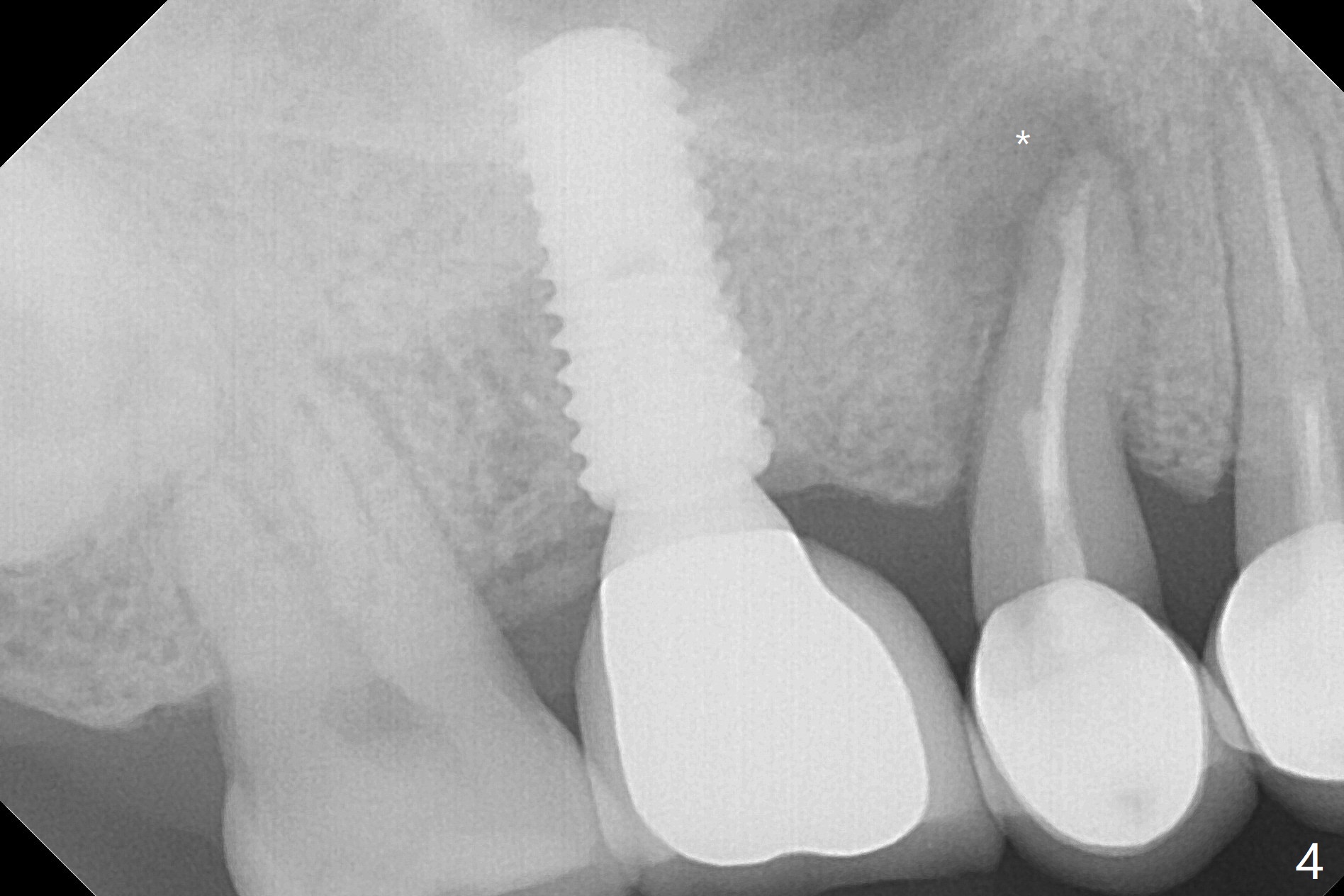
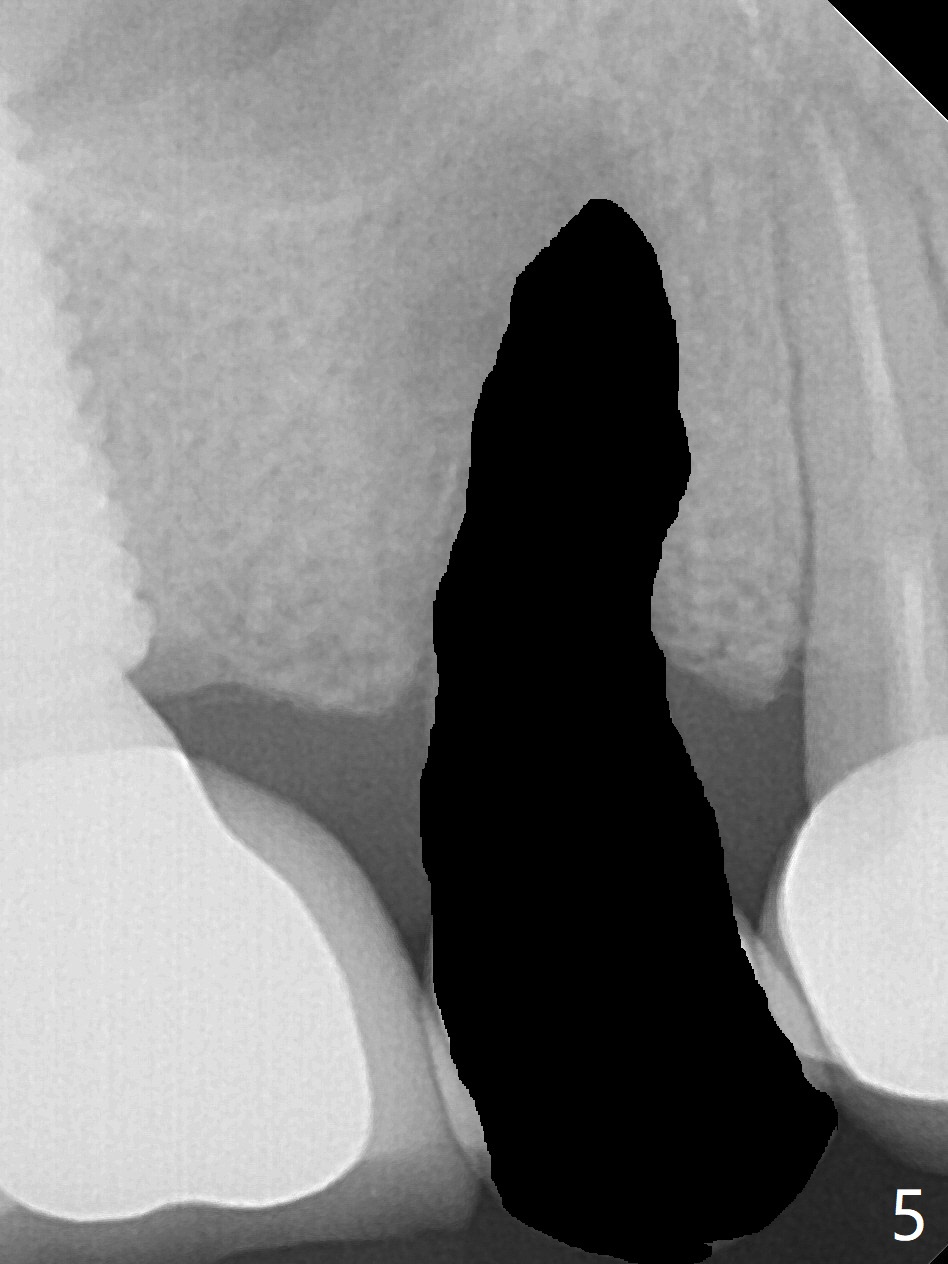
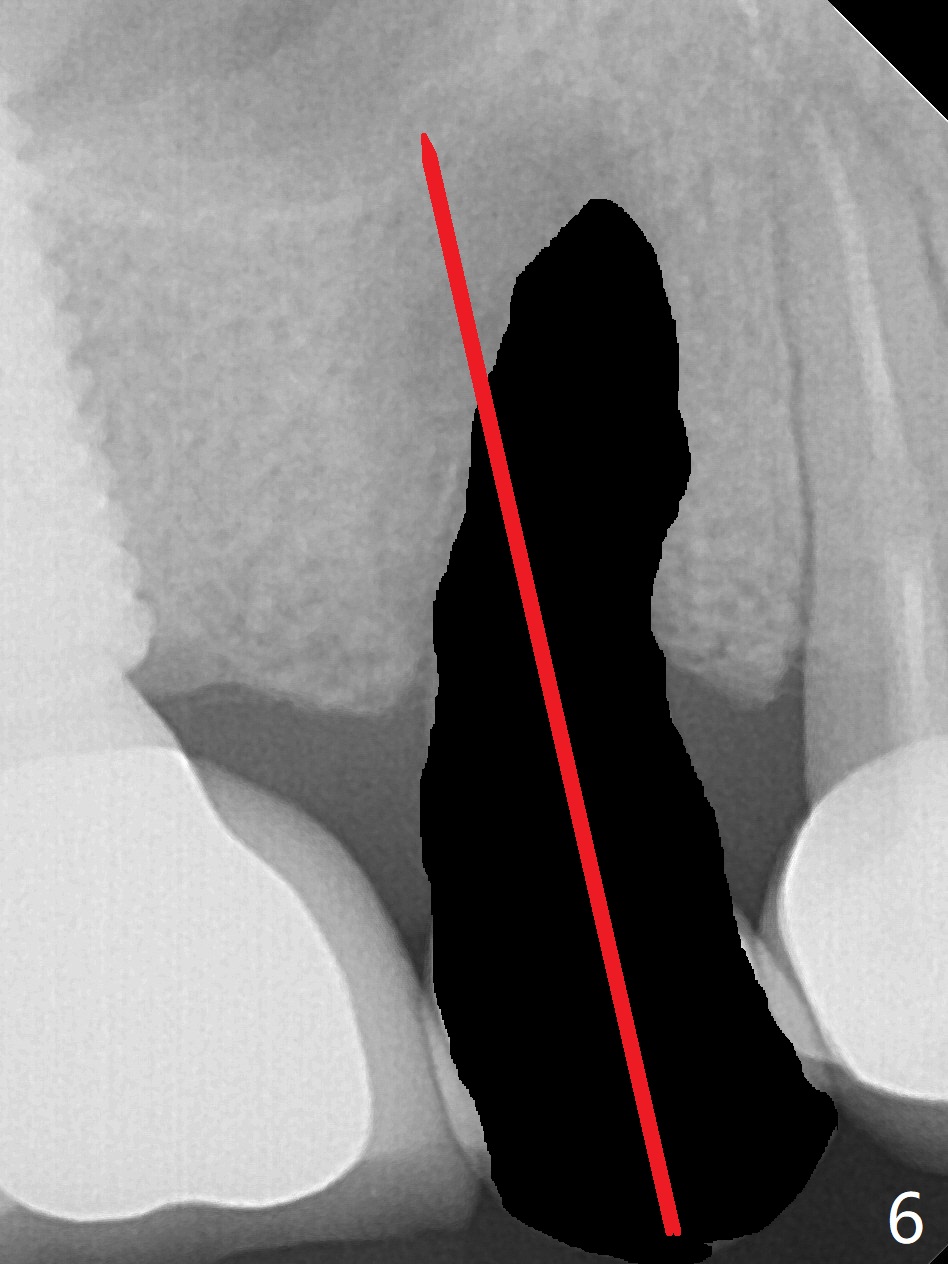
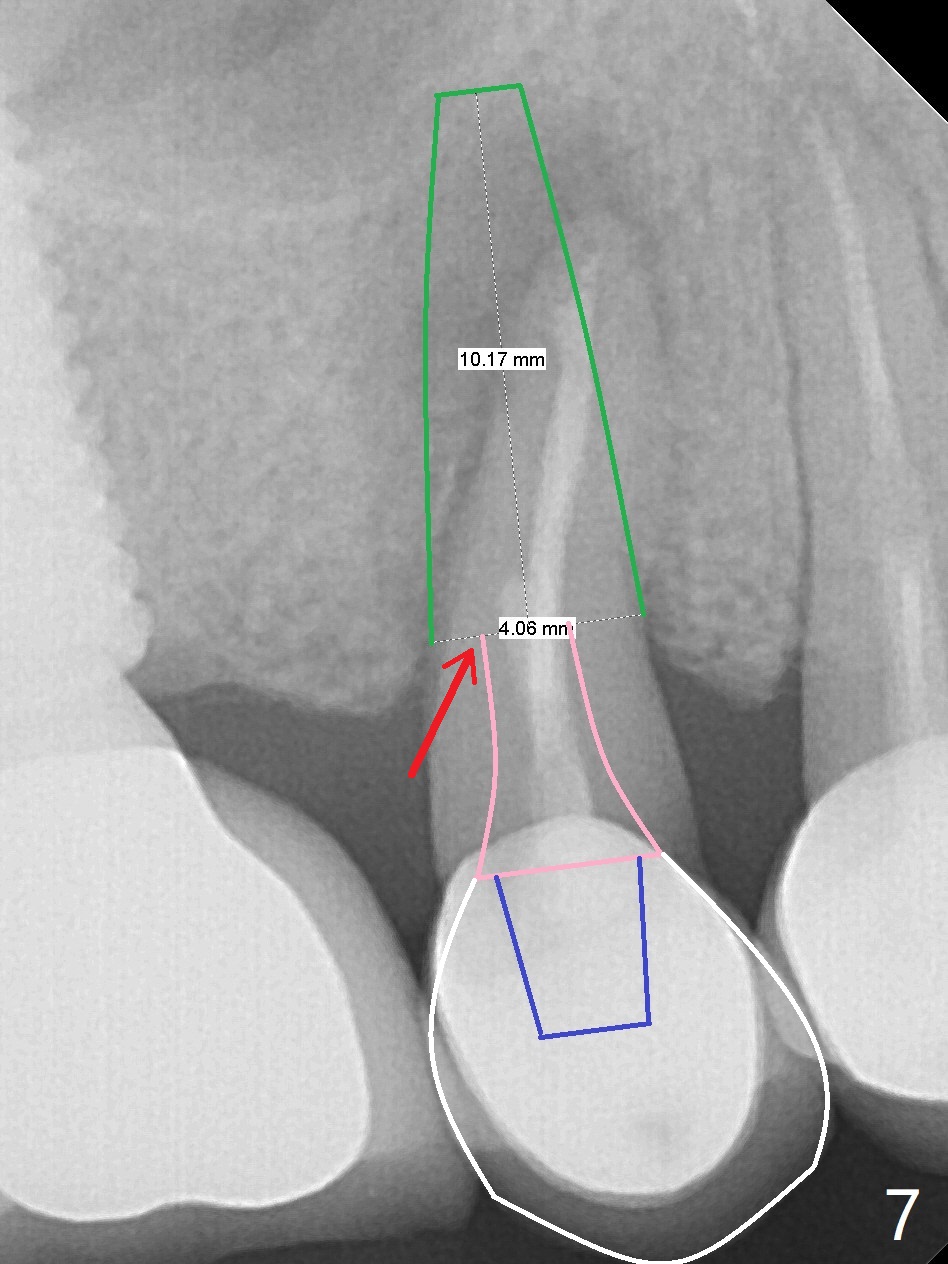
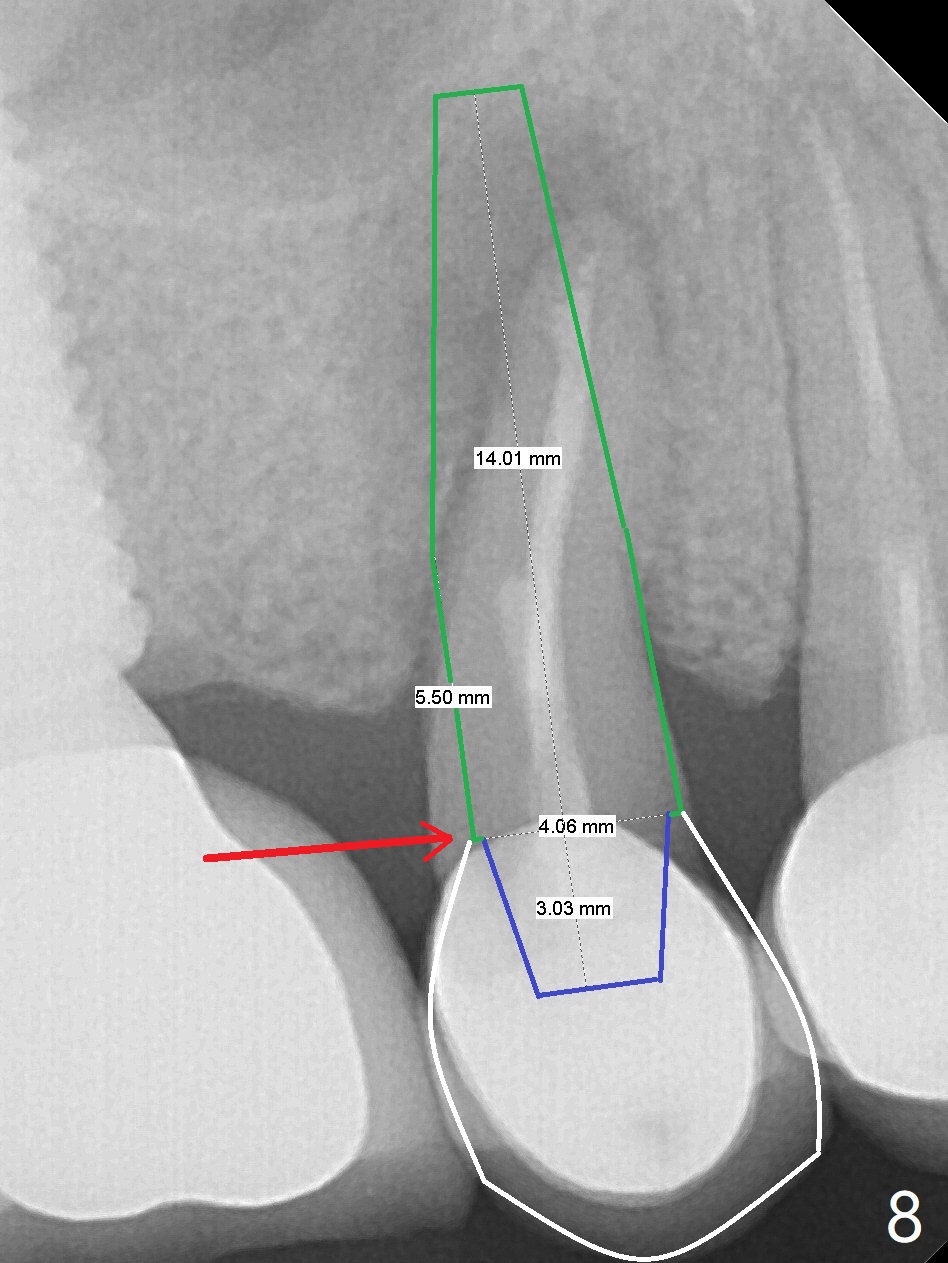
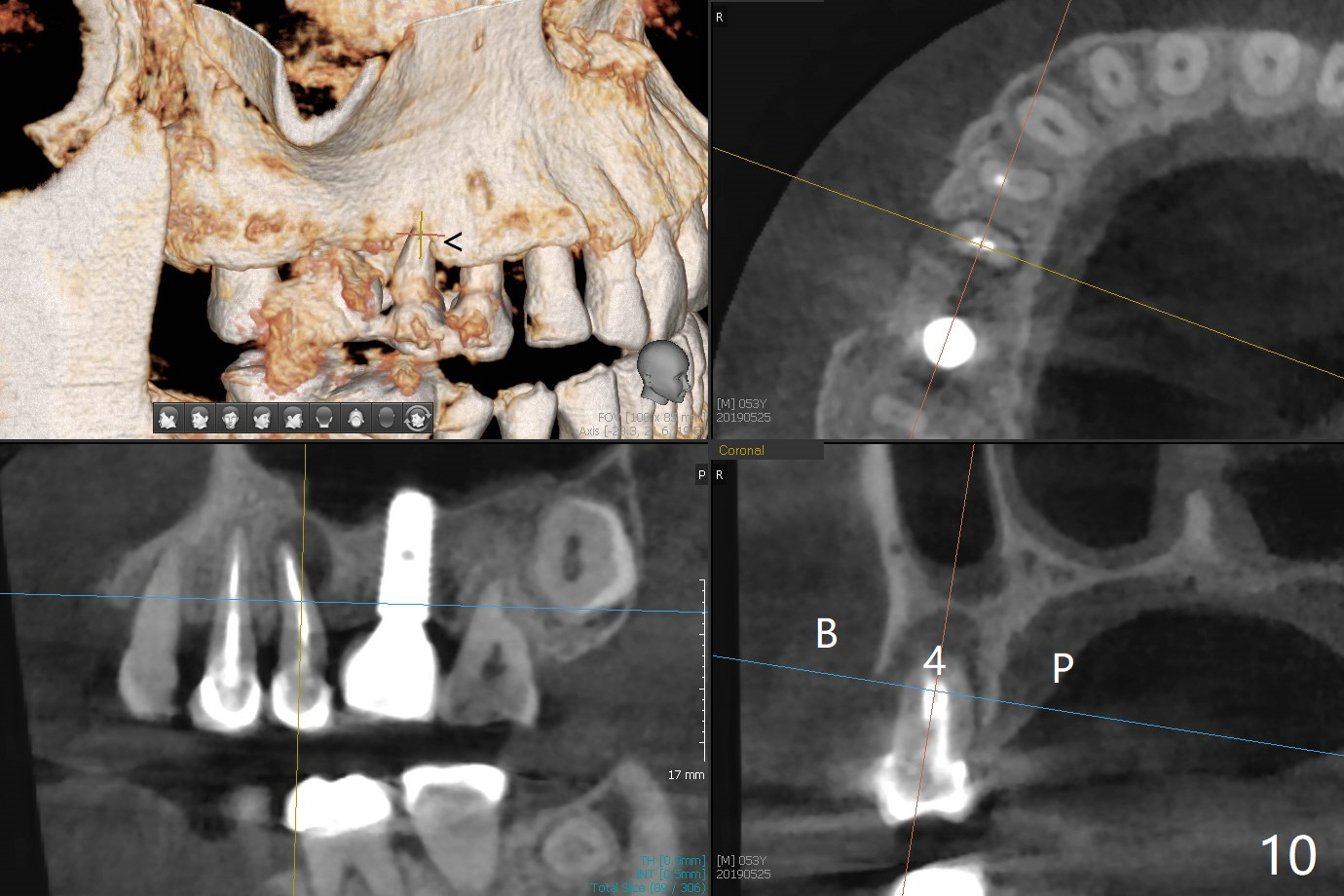
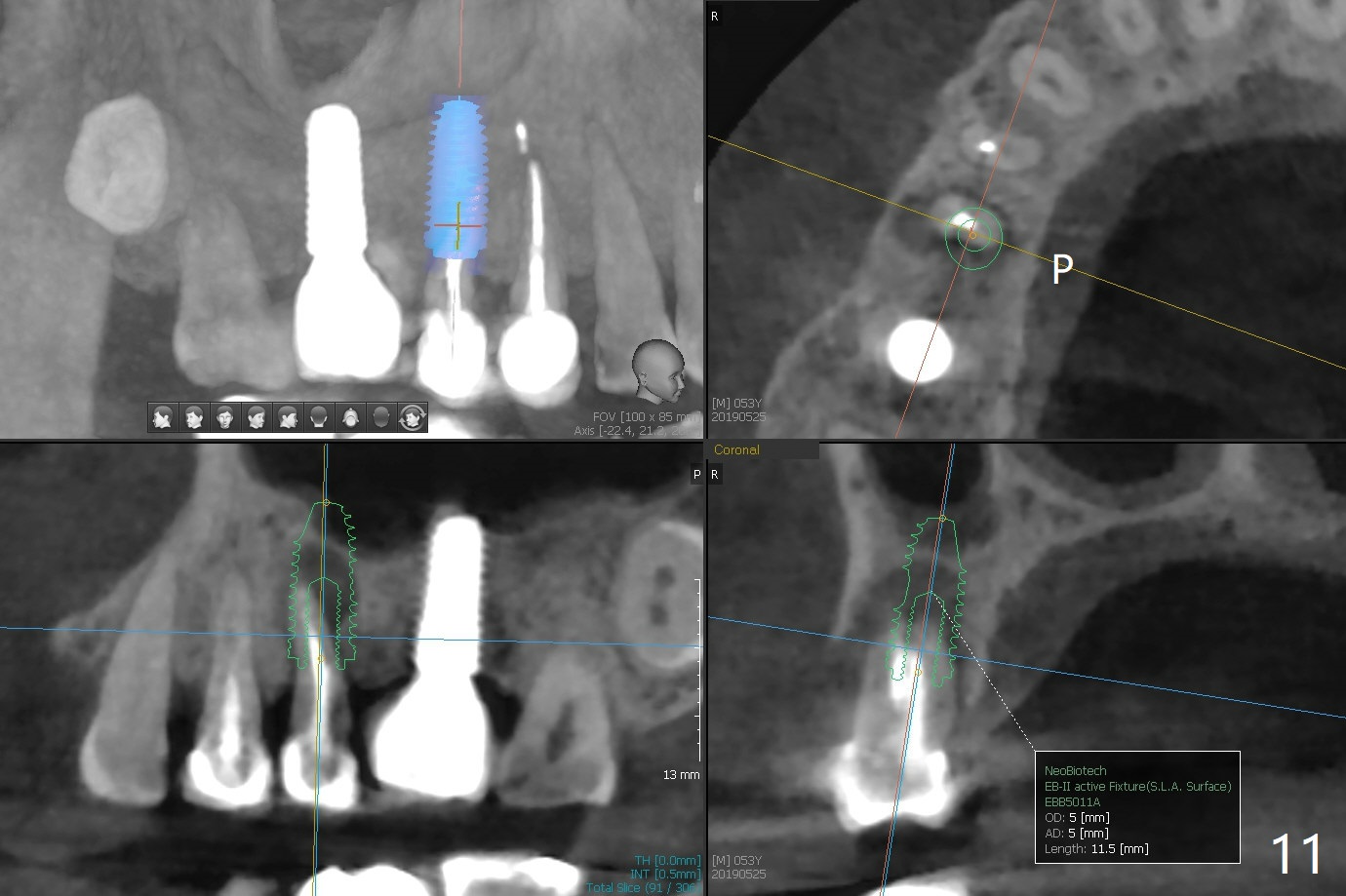
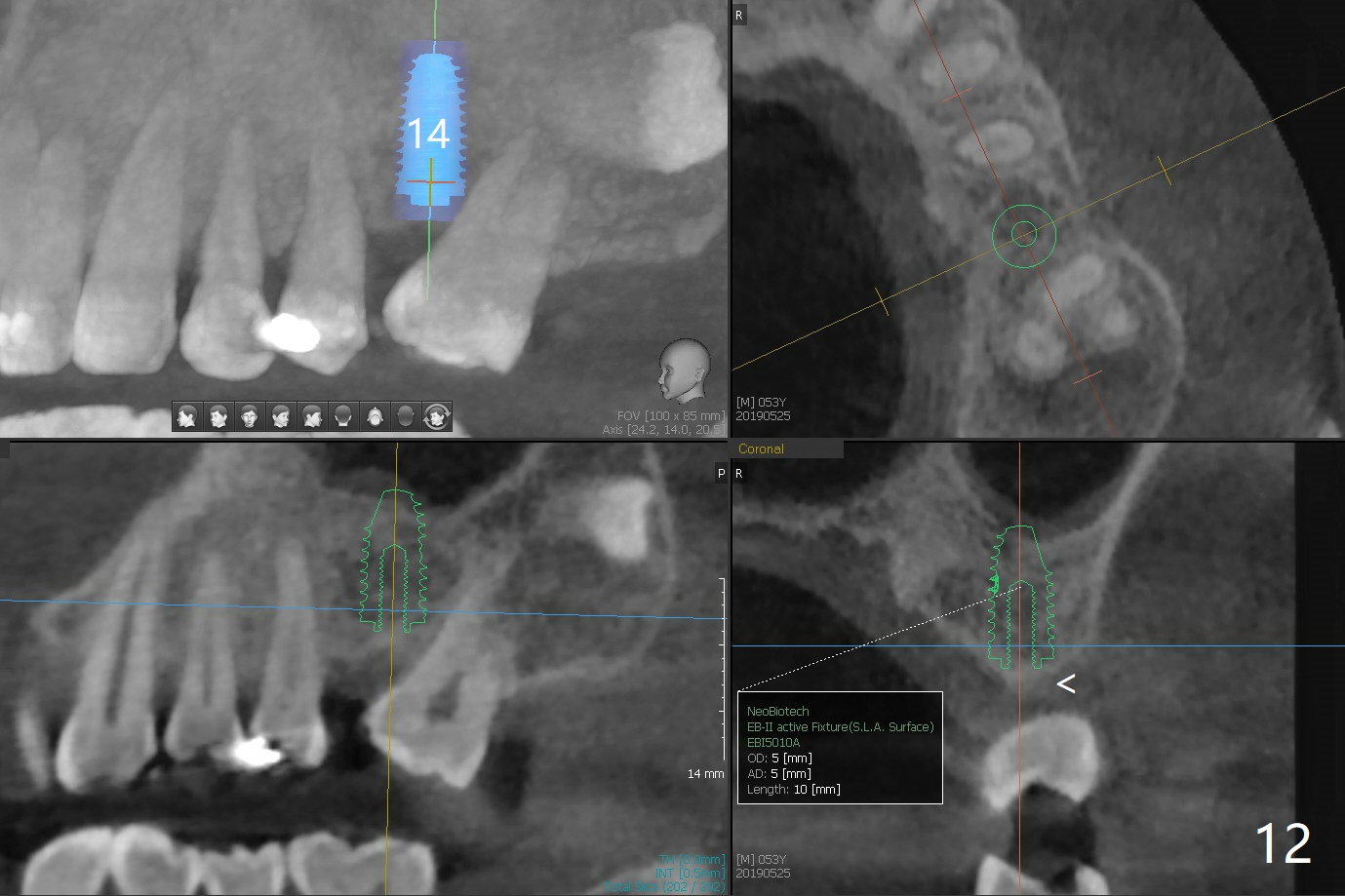
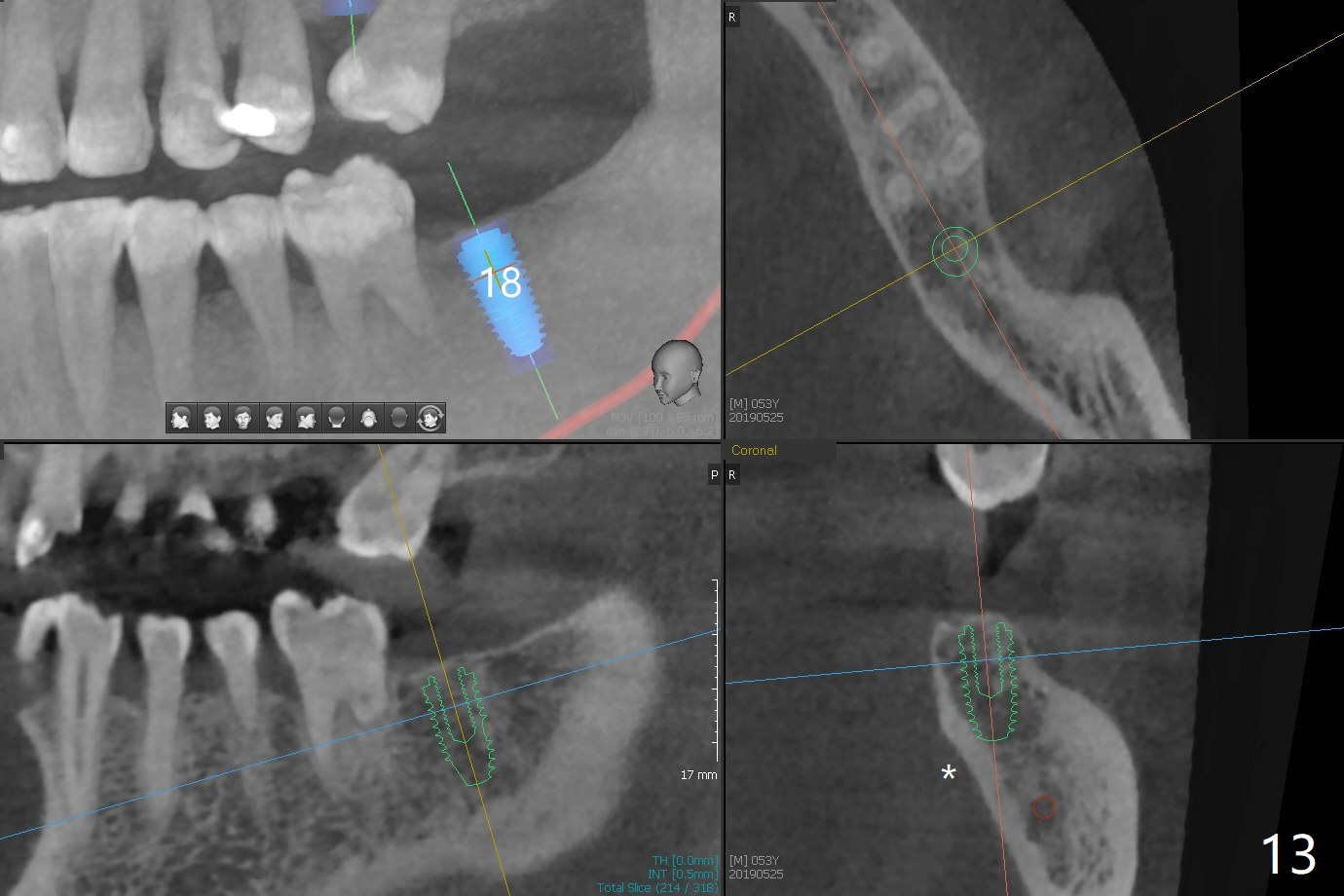
A 53-year-old man has signs of bruxism (Fig.1 diastema *) and root fracture or RCT failure at #4 (Fig.4 (large PARL *)). The RCT failure is related to overload of the affected tooth, which is in turn partially due to infraocclusion of the neighboring implant crown (Fig.1 arrows (implant positioning not ideal)) and partially to due to partial edentulism (Fig.2 missing teeth #14 and 18). For long term, limited ortho will be performed to upright and distalize the tooth #15 (Fig.3 arrow), followed by implants at #14 and 18. For now, the tooth #4 will be extracted (Fig.5), followed by osteotomy in the distal slope of the socket with guide (Fig.6 to get good trajectory). To place a bone-level implant (Fig.7 green), an abutment (blue) with long cuff (pink) is to be used. With poor implant/crown (white) ratio, stress occurs at the junction of the implant/abutment (red arrow), resulting in easy abutment screw loosening. In contrast, stress may be applied to directly to a tissue-level implant (Fig.8 arrow) with less likelihood of abutment screw loosening. The implant/crown ratio improves by approximately 5.5 mm. The roots of the teeth #15 and 16 are so close to each other that interference may occur when the tooth #15 is being uprighted (Fig.9). The empty socket of the tooth #4 is wide buccopalatal (Fig.10); the buccal plate is resorbed coronally (Fig.10 <) so that a 4.5 or 5 mm diameter implant should be placed palatal (Fig.11). Use sticky bone to repair the buccal plate defect and PRF membrane or plug for sinus lift. Following #15 uprighting and distalization, a 5x10 mm implant will be placed at #14; the ridge is triangular (Fig.12 <) so that bone trimmer is needed. A 10 mm long implant will be placed at #18 (Fig.14) to avoid perforating to the submandibular fossa (Fig.13 *).
Return to Upper Premolar Immediate Implant, Trajectory, No Antibiotic Open Margin Limited Ortho 矫正,糖尿病,种植水平 18 导板 Xin Wei, DDS, PhD, MS 1st edition 03/03/2019, last revision 12/11/2020