

.jpg)

|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Trying for Ideal Occlusion
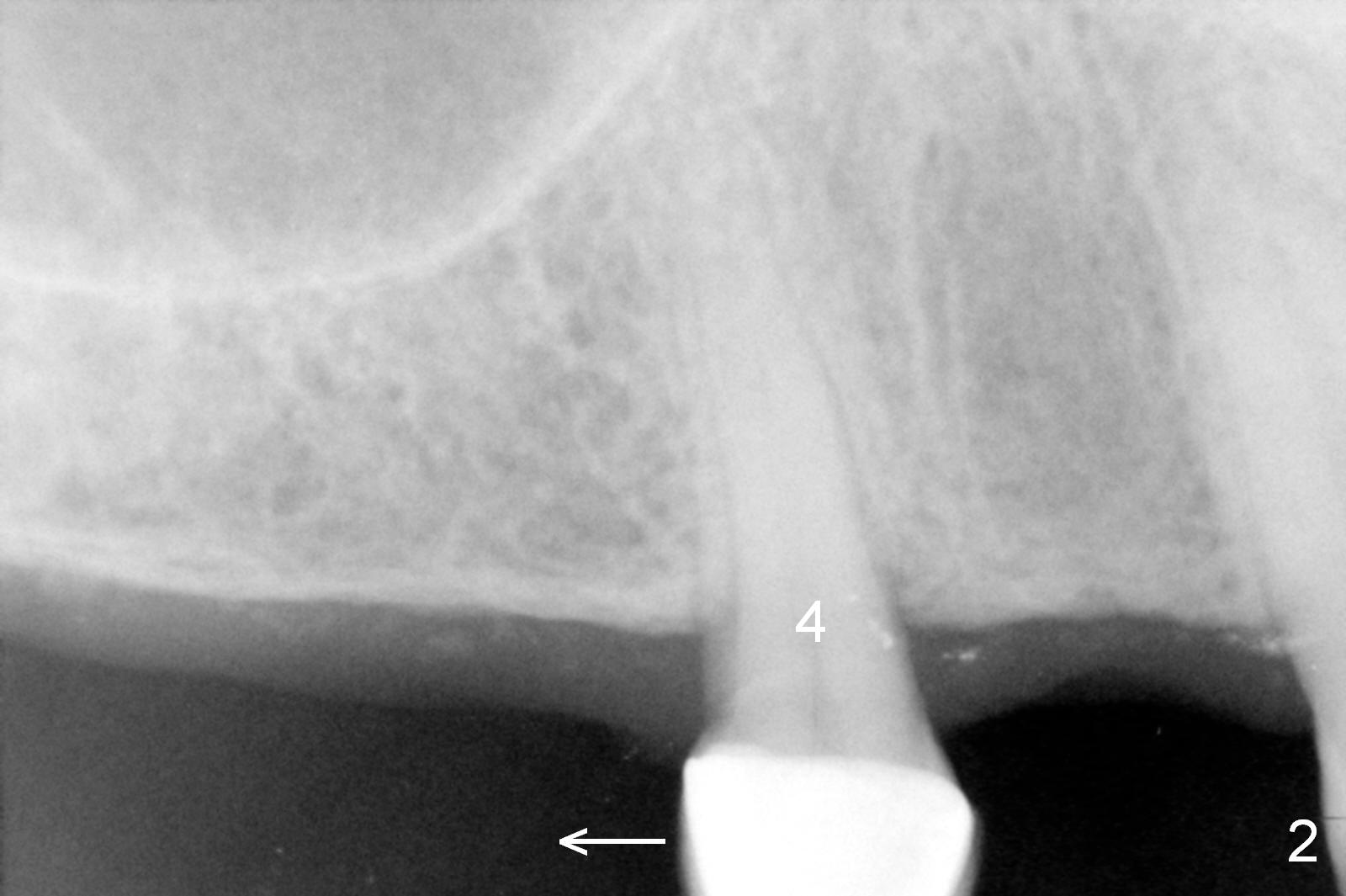
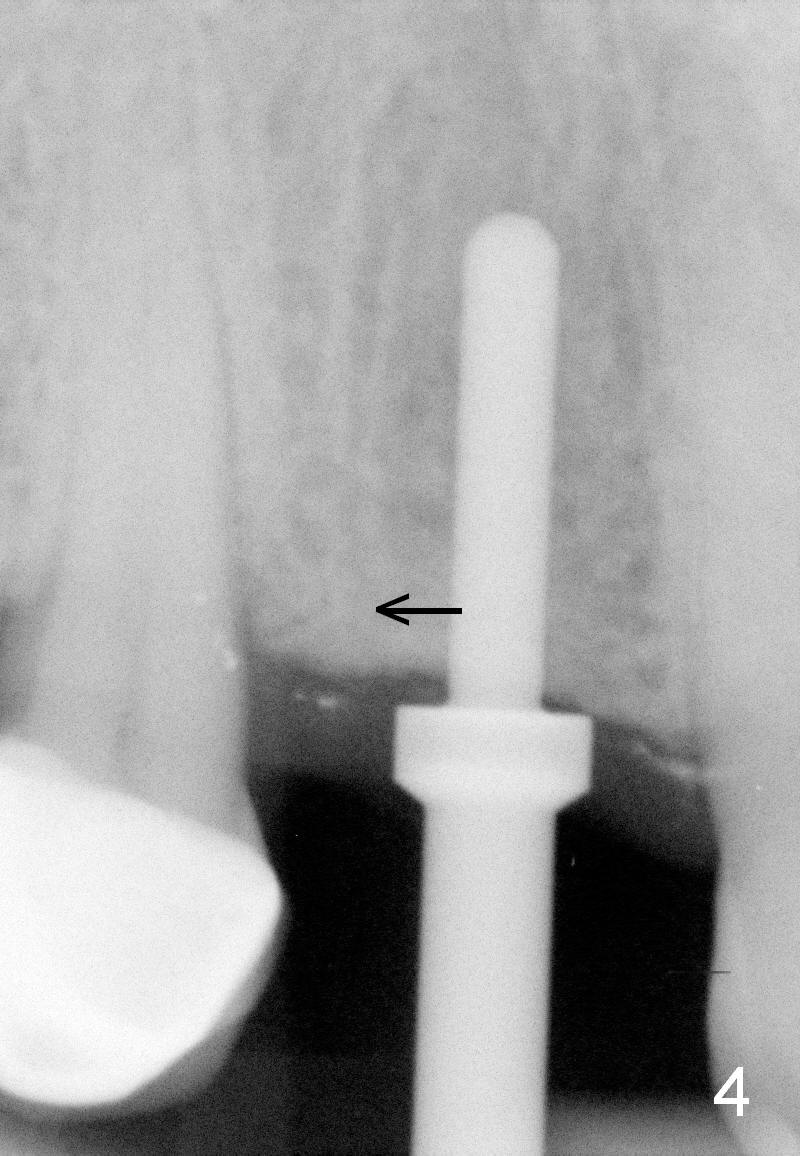
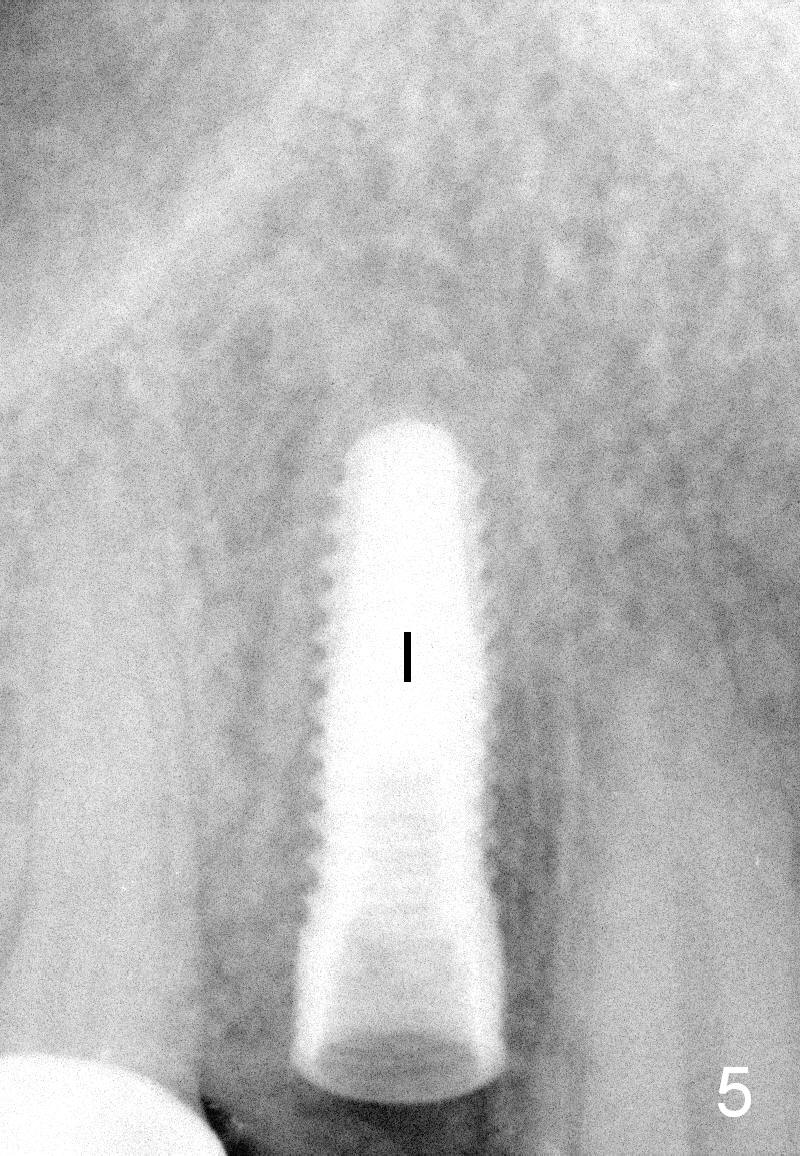
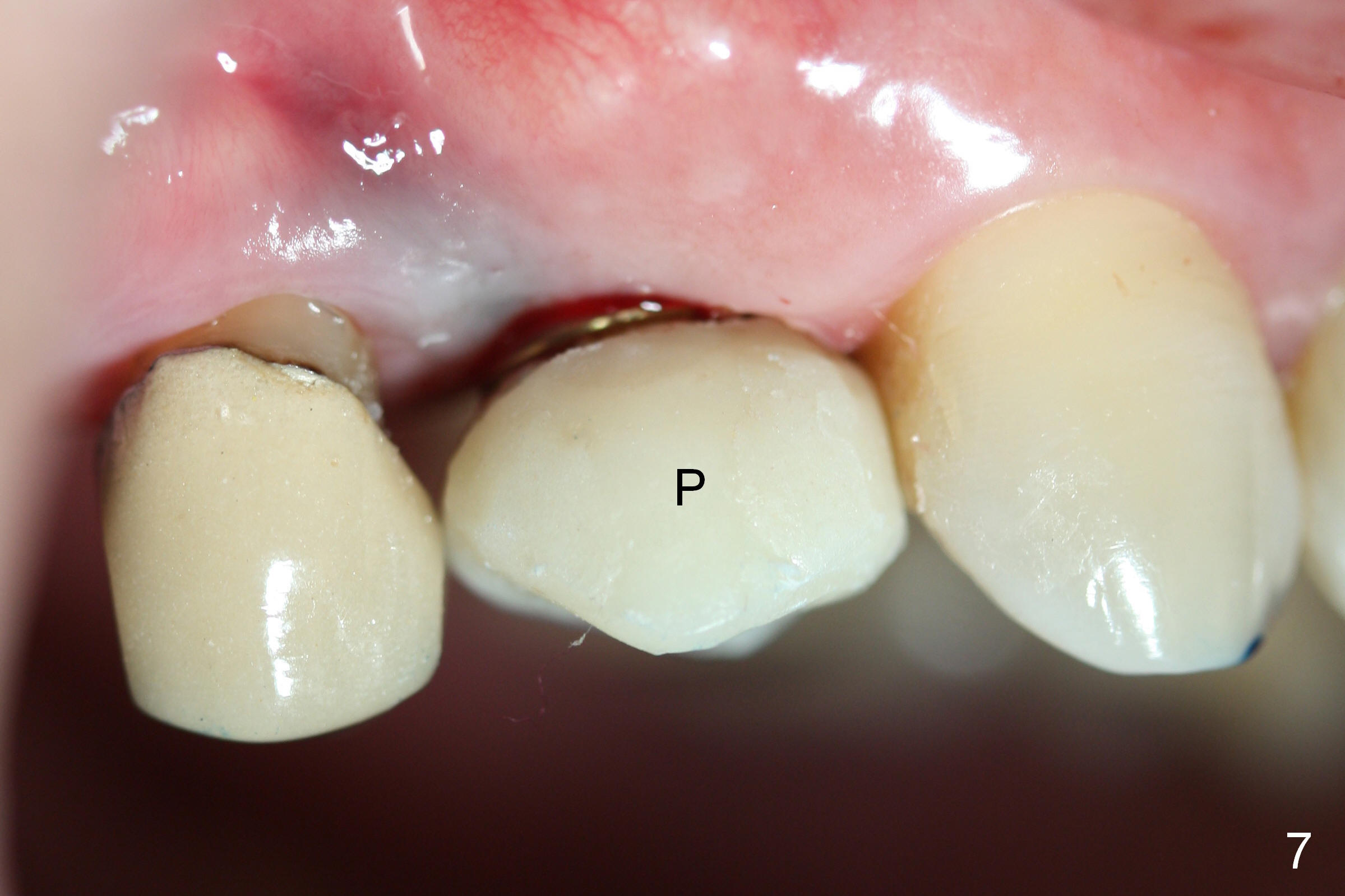
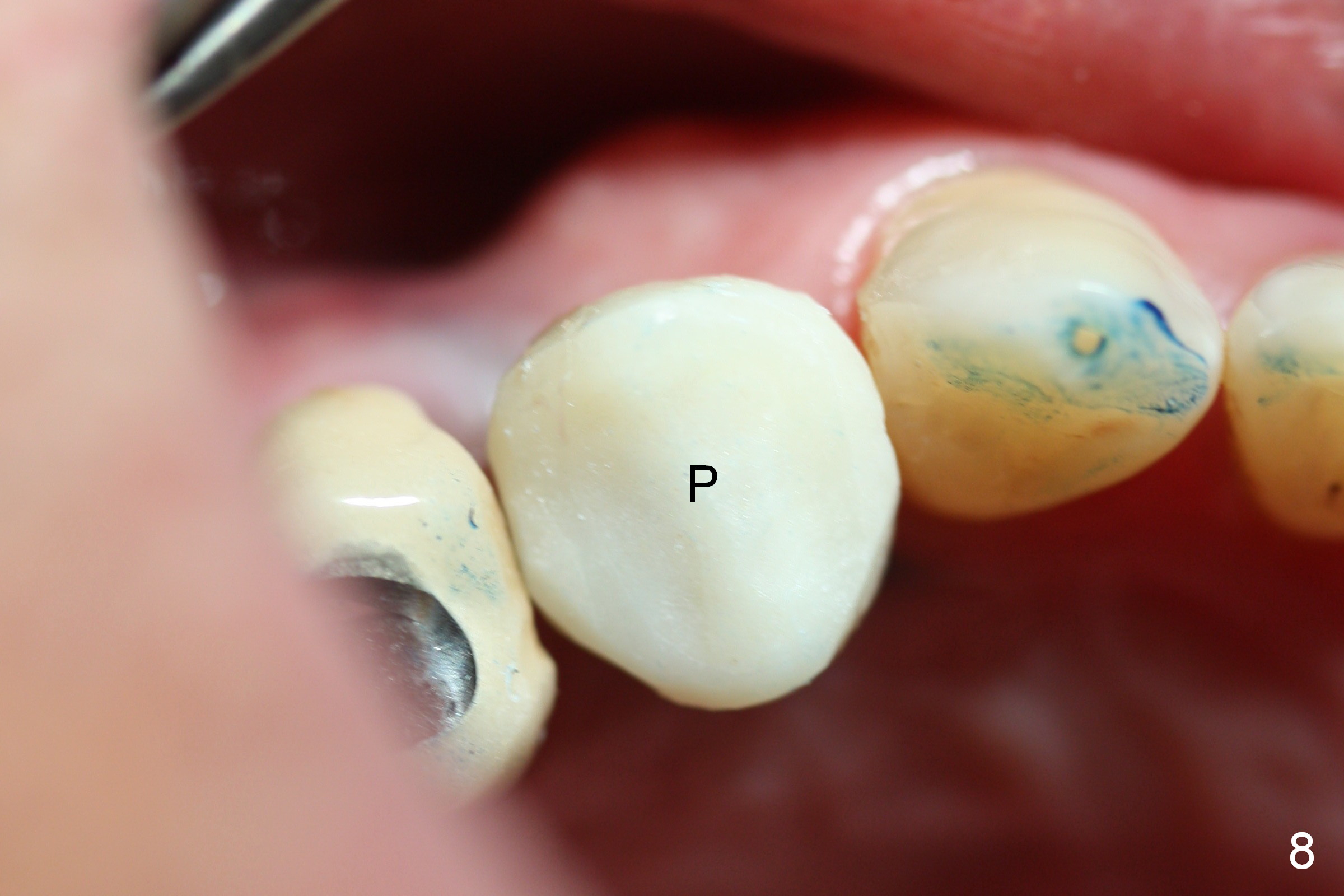
A 66-year-old man has lost several teeth (Fig.1,2). There is a particularly wide mesiodistal space for the site of #5 (Fig.1), probably due to distalization of the tooth #4 under heavy occlusion (Fig.2 arrow). A 4 mm tissue punch is used for access, followed by 1.6 mm pilot drill (Fig.3). After trajectory adjustment, a 2 mm parallel pin is inserted (Fig.4); later the osteotomy is moved distally (arrow). Finally a 4.5x14 mm implant is placed (Fig.5 I). Due to limited access, the implant is placed a little deeper than necessary; the gingival cuff of an abutment has to be longer (Fig.6 A: 5.8x4(3) mm). An immediate provisional is fabricated (Fig.7,8 P). The provisional looks wide (Fig.7). When the implant osteointegrates, limited orthodontic treatment will be done to idealize the space of #5 as follows.
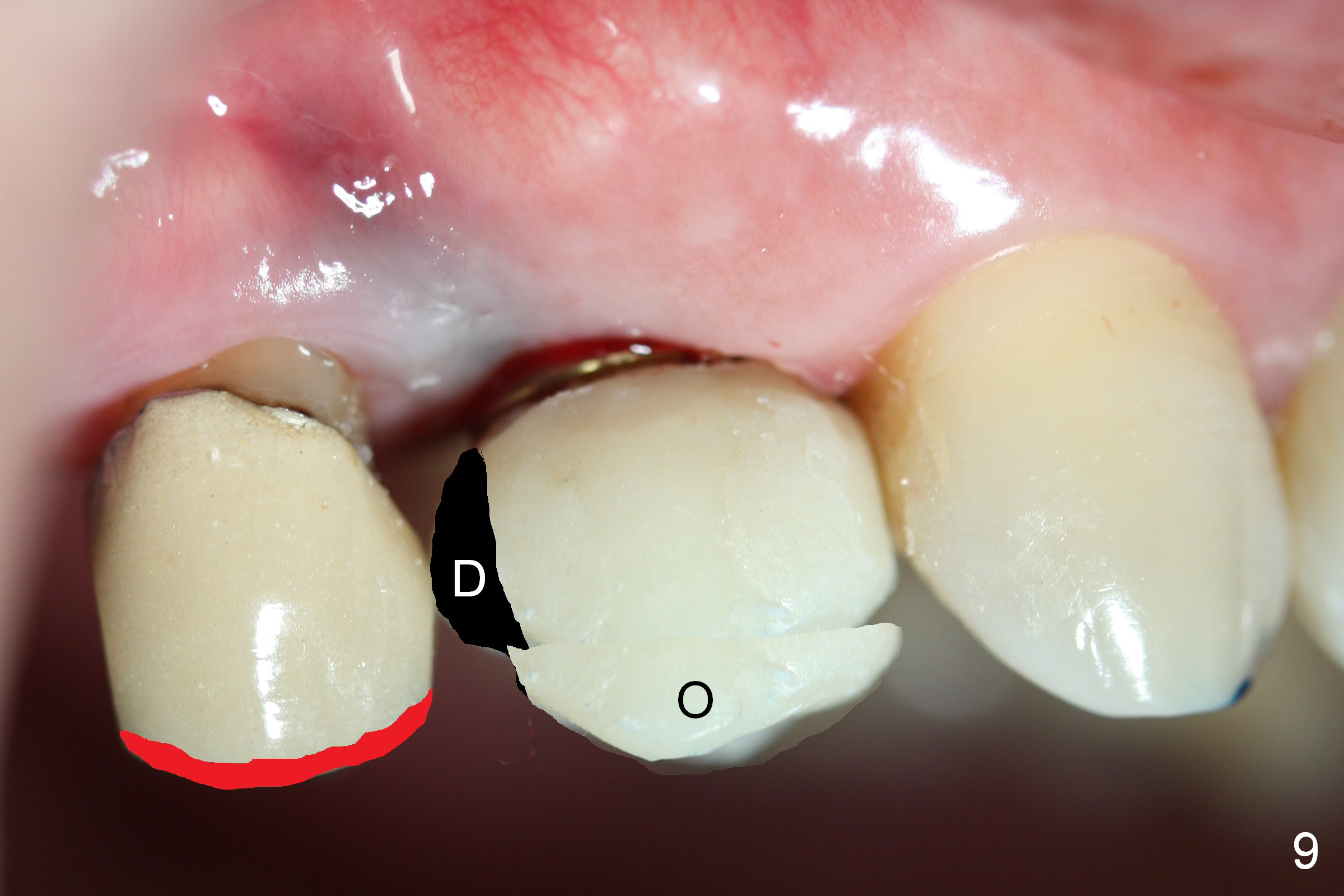
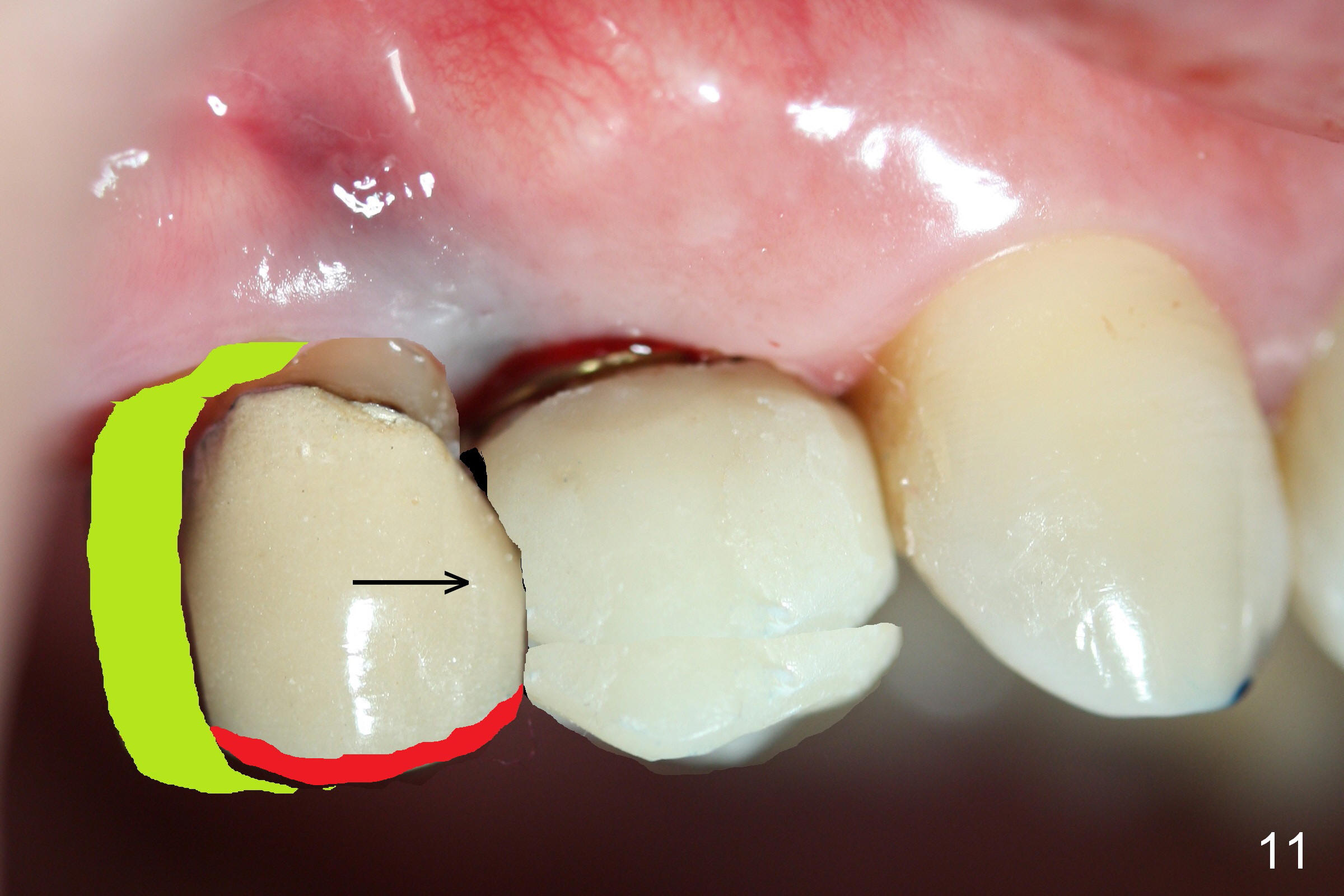
The distal surface of the provisional will be reduced (Fig.9,10 D), whereas the occlusal surface will be increased (Fig.9 O). If needed, the occlusal surface of the distalized tooth #4 will be reduced (Fig.9 red area) so that there is no interference for tooth to move. Hooks will be placed on the buccal and lingual surfaces of the provisional (Fig.10 green curved lines). Power chains will be placed on the hooks and wrapped around the tooth #4. In due time, the tooth will be mesialized (Fig.11 arrow). Implants at the sites of #2 and 3 will be placed in more appropriate positions.
Return to Professionals,
Implant & Ortho
Xin Wei, DDS, PhD, MS 1st edition 03/01/2015, last revision 03/01/2015