|
|
|
||
|
|
|
|
|
|
|
|||
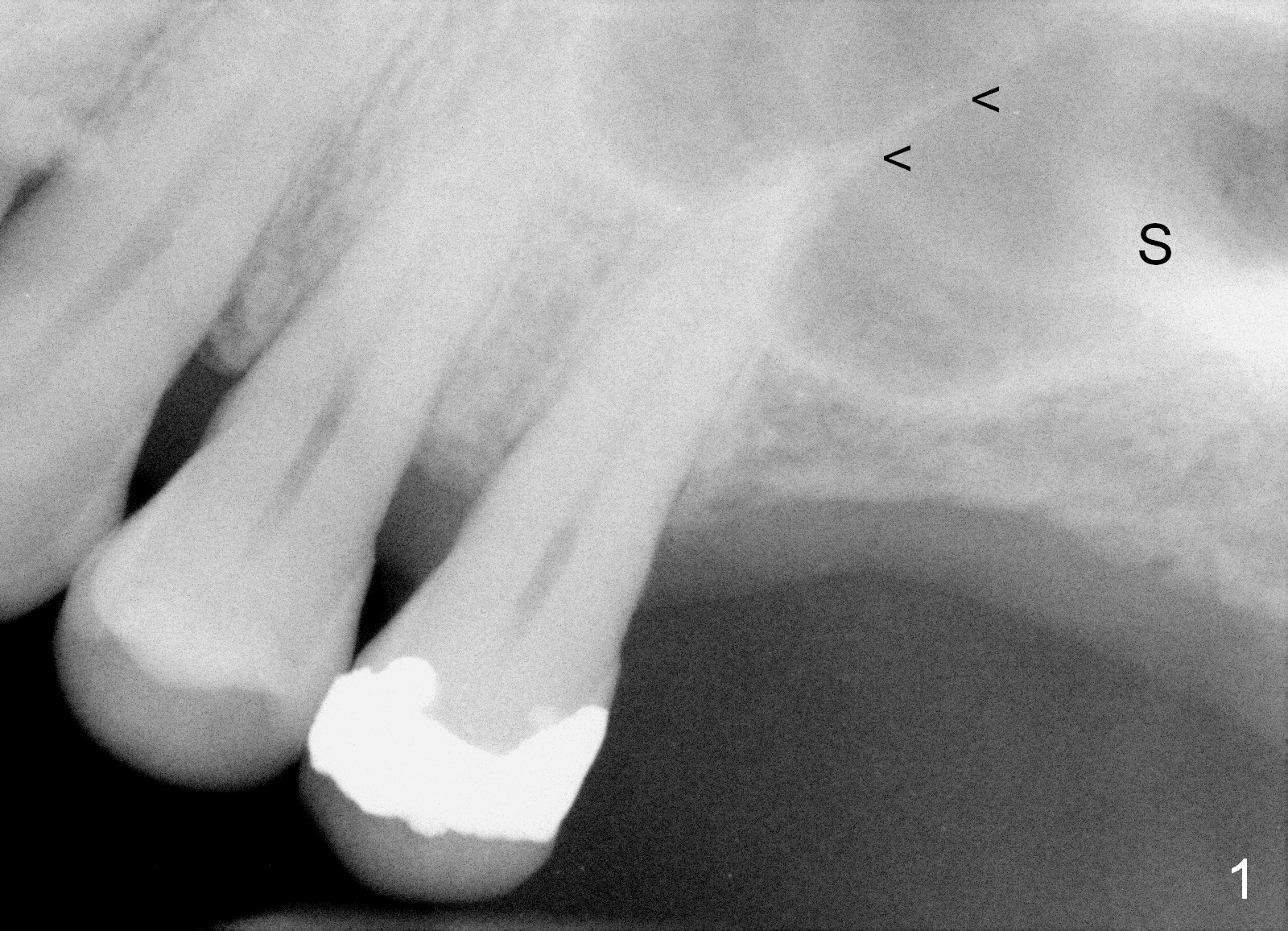
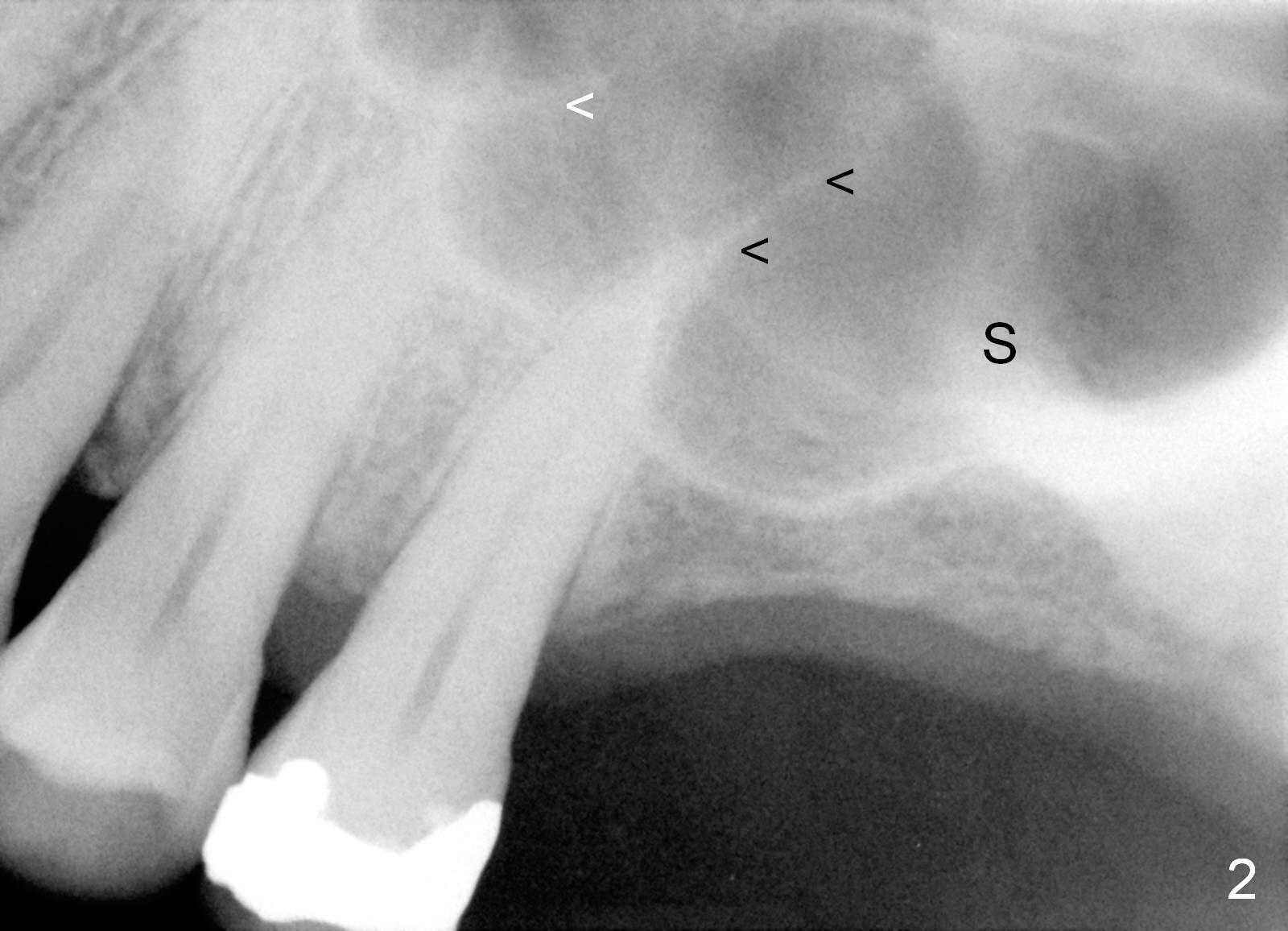
Crestal or Lateral Approach for Limited Bone Height?
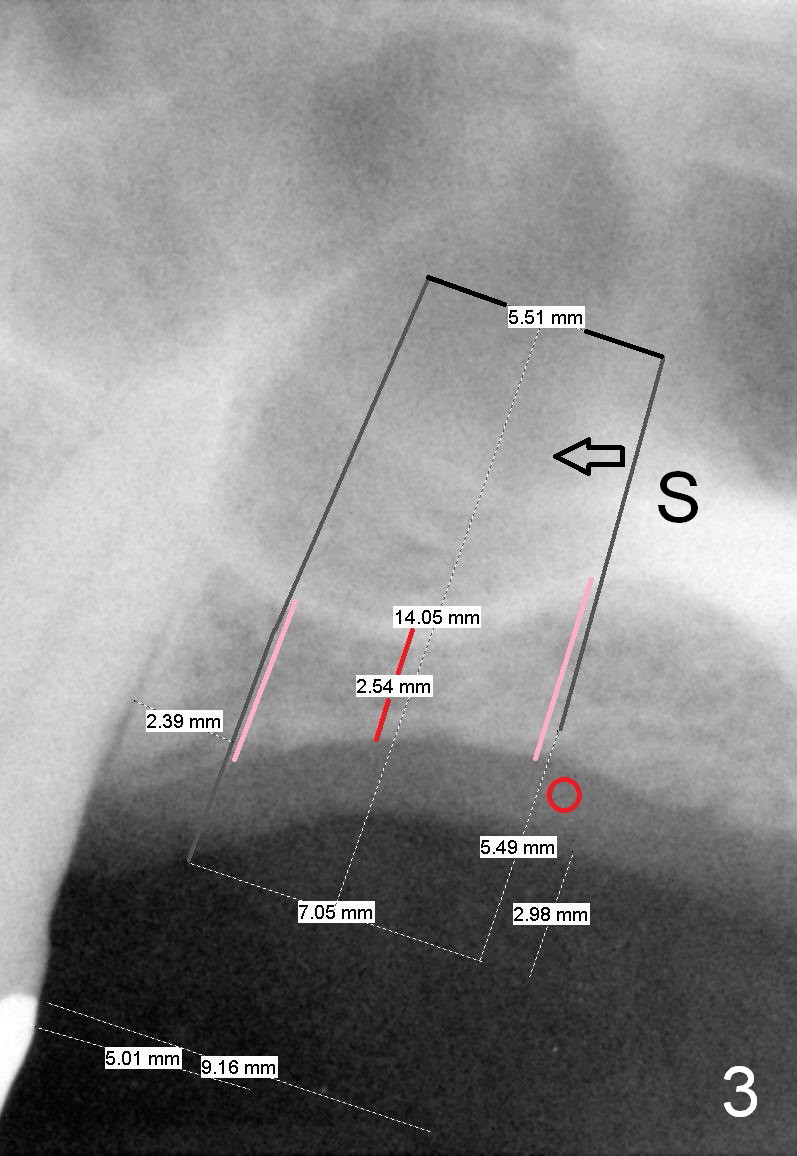
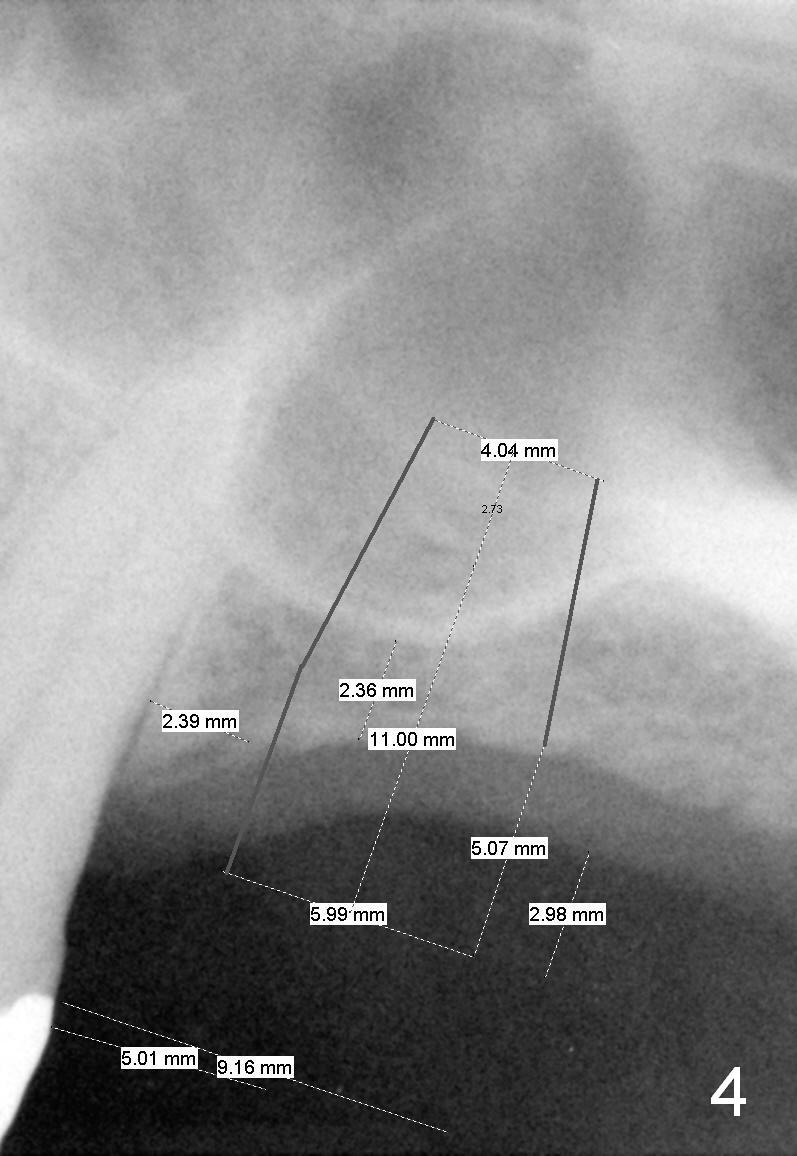
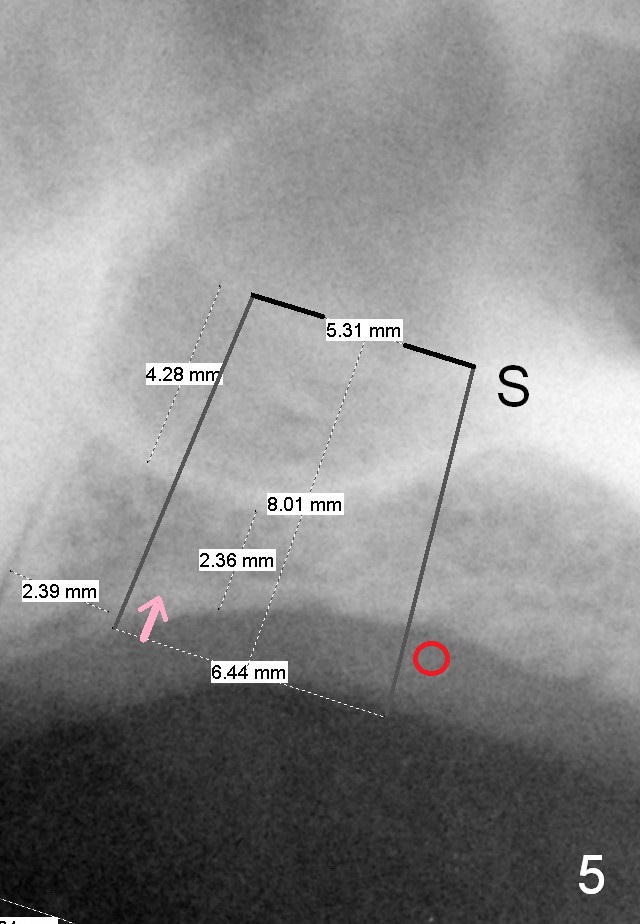
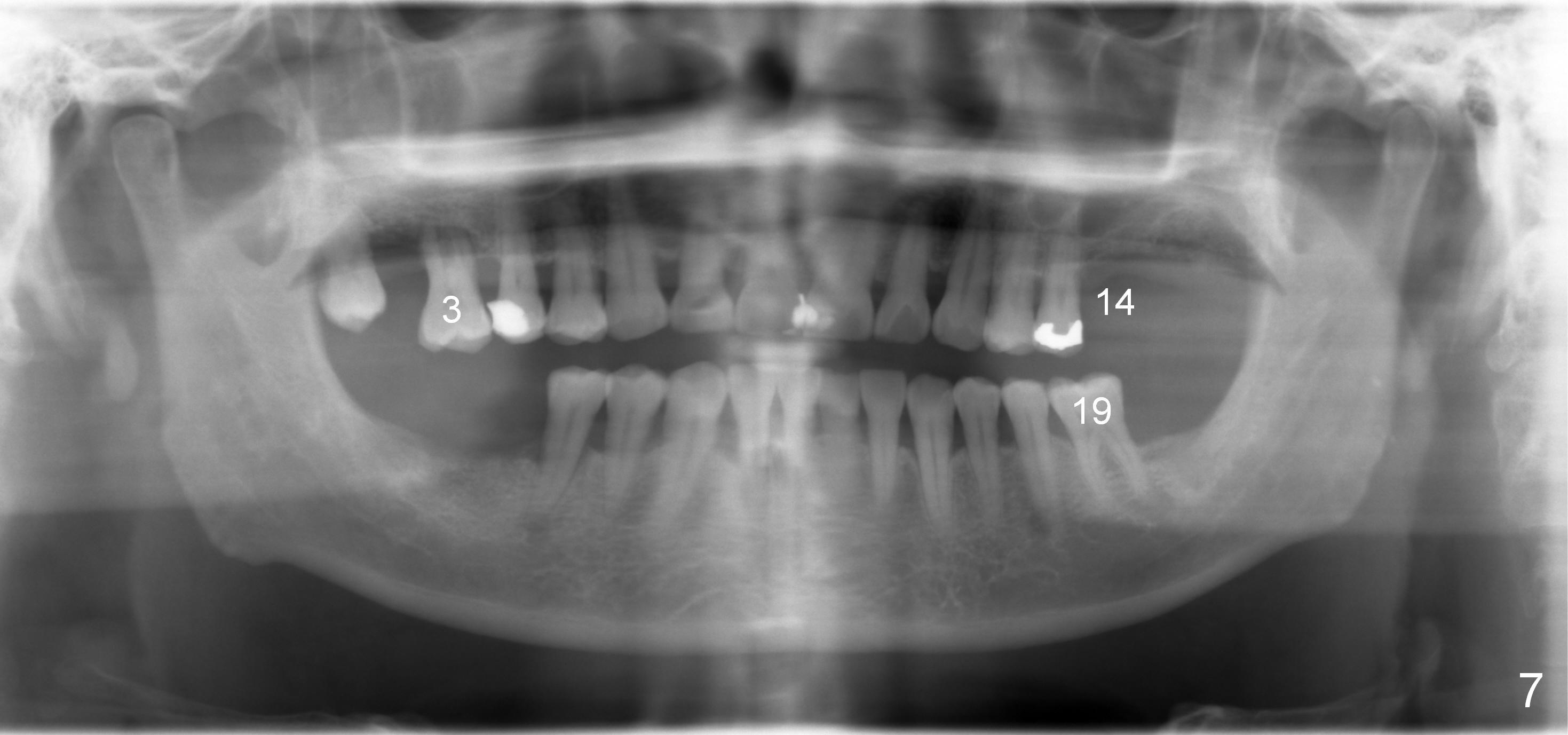
A 60-year-old man requests implant at the site of #14 (Fig.1,2, opposing a natural tooth (Fig.7)). Although bone height is limited, bone density appears high with sinus septi (S and arrowheads). The ridge seems to be wide clinically; implant will be as wide as possible. An envelop incision will be made to get the best visibility (as compared to tissue punch). At entry point, the bone height is 2.5 mm (Fig.3 red line); as the implant or osteotomy diameter increases, bone contact enhances (pink lines). If lateral window approach is adopted, a longer implant will be chosen (14 mm in Fig.3 vs. 11 mm in Fig.4, both tissue-level). The stronger distal septum may deviate the apical portion of the longer implant (Fig.3 arrow).
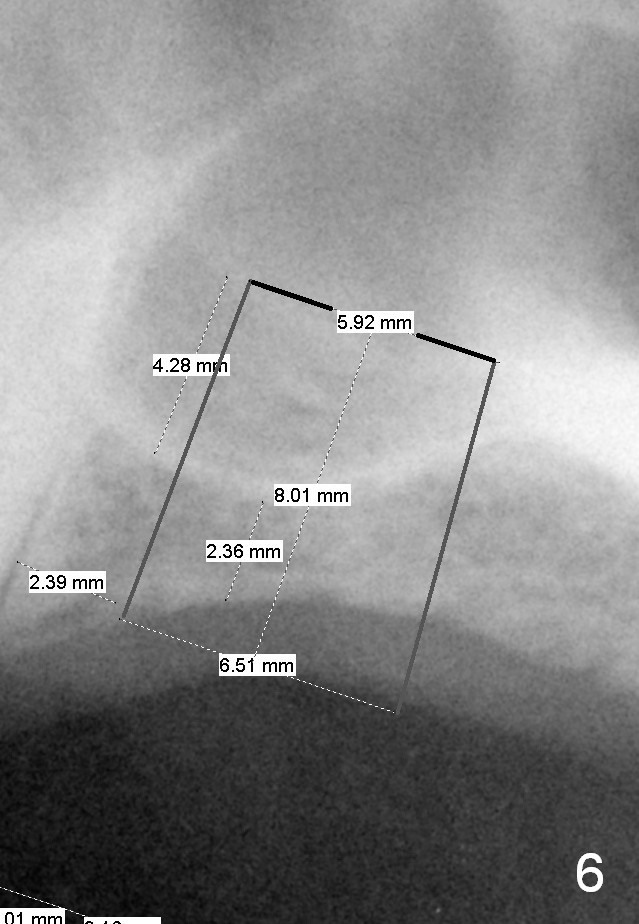
Another set of choice will be bone-level implants (SM and UF). The advantage of the former is its taper; the difference of the base and apex diameter is 1.1 mm (Fig.5 vs. 0.6 mm for UF (Fig.6)). It appears that a smaller parallel-walled drills can be used for the former (underprep) so that primary stability is more easily achievable. But according to the manufacture, the design of the latter allows the threads to be more aggressive. The surface treatment of the latter is more advanced (hybrid sand blast & acid etched vs. resorbable blast media; osseointegration occurs quicker for the latter). Which implant is finally chosen?
Return to
Professionals,
Sinus Lift,
Upper Molar Immediate Implant
,
Dr. Wu
Xin Wei, DDS, PhD, MS 1st edition 02/15/2015, last revision 11/05/2015