











|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Access to Obliterated Upper Central Incisor
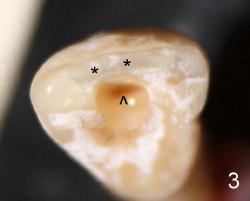
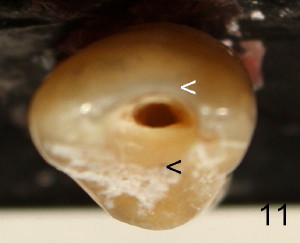
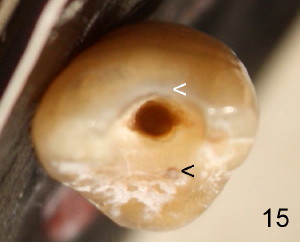
The tooth #8 of a 61-year-old man has obliterated canal probably due to trauma (Fig.1,2 (lateral view)). Initial access shows that the labial portion of the recessed pulpal horn (brown, < in Fig.3 (occlusal view) is not fully exposed, while that the most lingual aspect of the incisal edge (between **) has been removed. Further access appears to be necessary to expose the obliterated pulpal chamber (Fig.7 <) and more of the incisal edge has been violated ( between **). With good exposure, the canal is easily found around the arrowhead (<) in Fig.7. Laterally, the initial file: C6 is straight and slightly labial to the incisal edge (Fig.6). But it is somewhat bent in the front view (Fig.5). After enlargement of the coronal canal with Gates-Glidden files #2 and 3 (Fig.9<), #20 file appears to move distally (<-) and is straighter than the file in Fig.5. Laterally, the #20 file remains without much tension and around the incisal edge (Fig.10). Fig.11 shows occlusal view of the access after application of Gates-Glidden files. Before rotary files, the access is enlarged further both labially and lingually with diamond/carbide endo access burs (Fig.15). Fig.13,14 show 40/.04 file in the canal free without strain. The file seems to move distally further (Fig.13 <-).
Although the incisal portion of the labial surface of the tooth is removed for the best access (compare Fig.8,16 with Fig.4), it should be repaired with composite immediately after RCT without esthetic compromise. Traditional way to get access actually sacrifices more lingual structure (Fig.11,15 black <) than the labial one (white <) or creates a ledge labial to the orifice. With more practice and patience, the mesial aspect of the incisal edge could have been saved in this case (Fig.13, mesial (right) to the rotary file).
Xin Wei, DDS, PhD, MS 1st edition 10/02/2011, last revision 10/10/2011