





|
|
|
|
|
|
|
|
|
|
|
|
How to Treat Fistula?
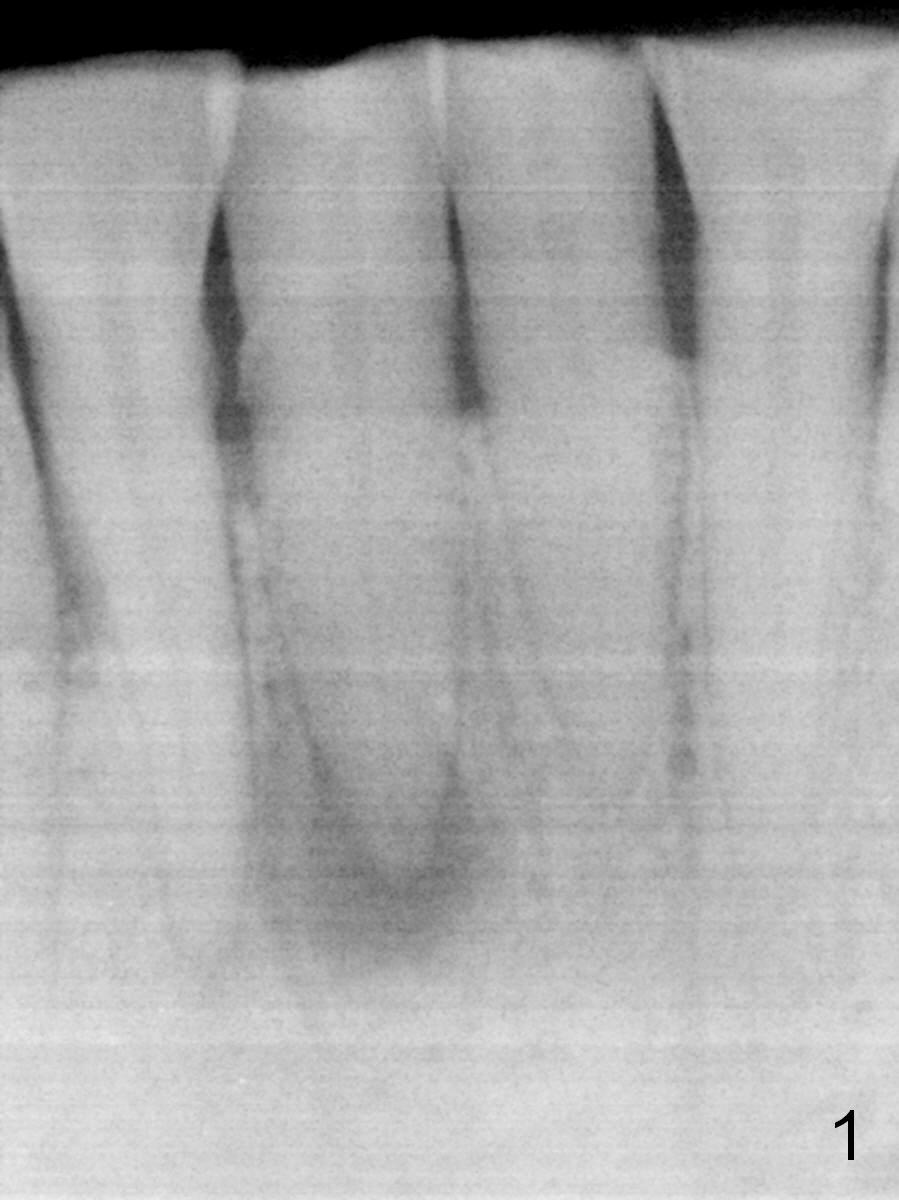
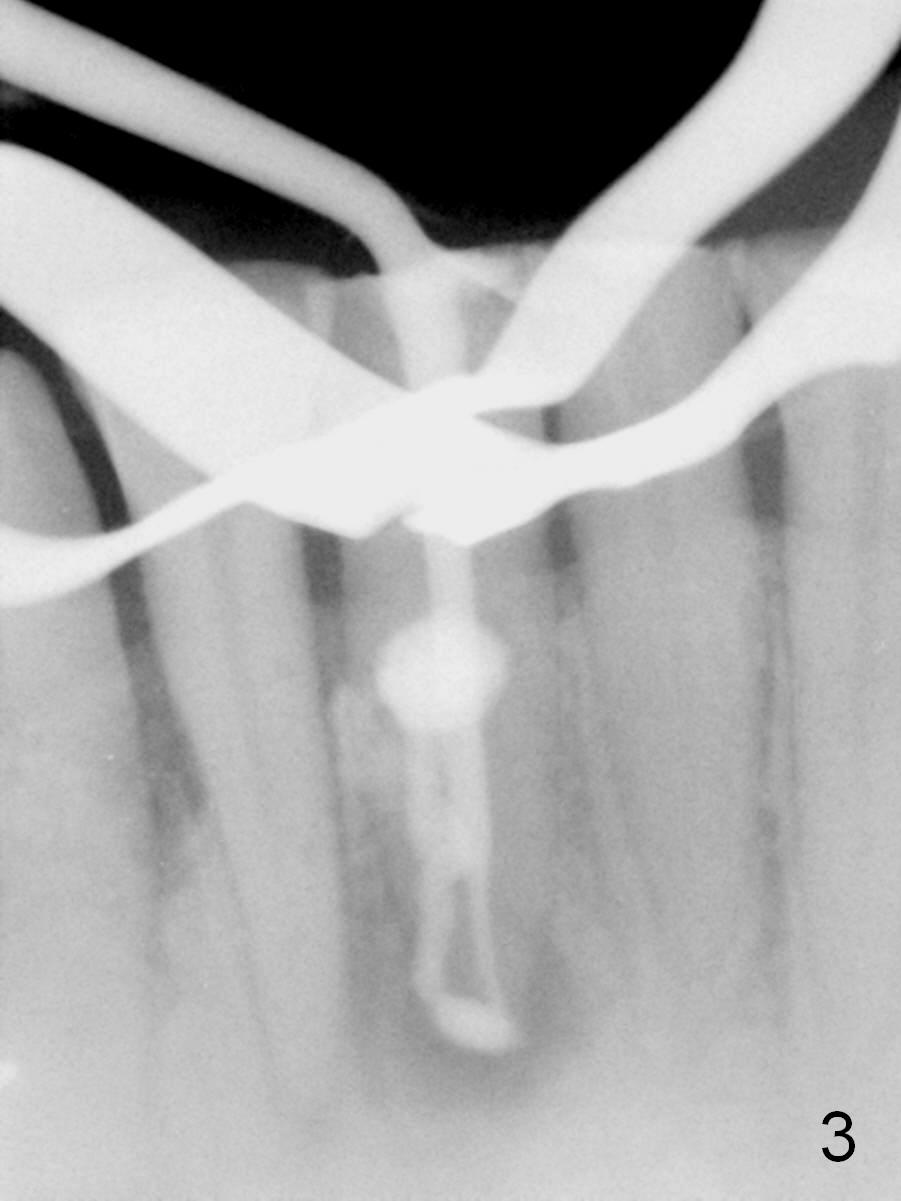
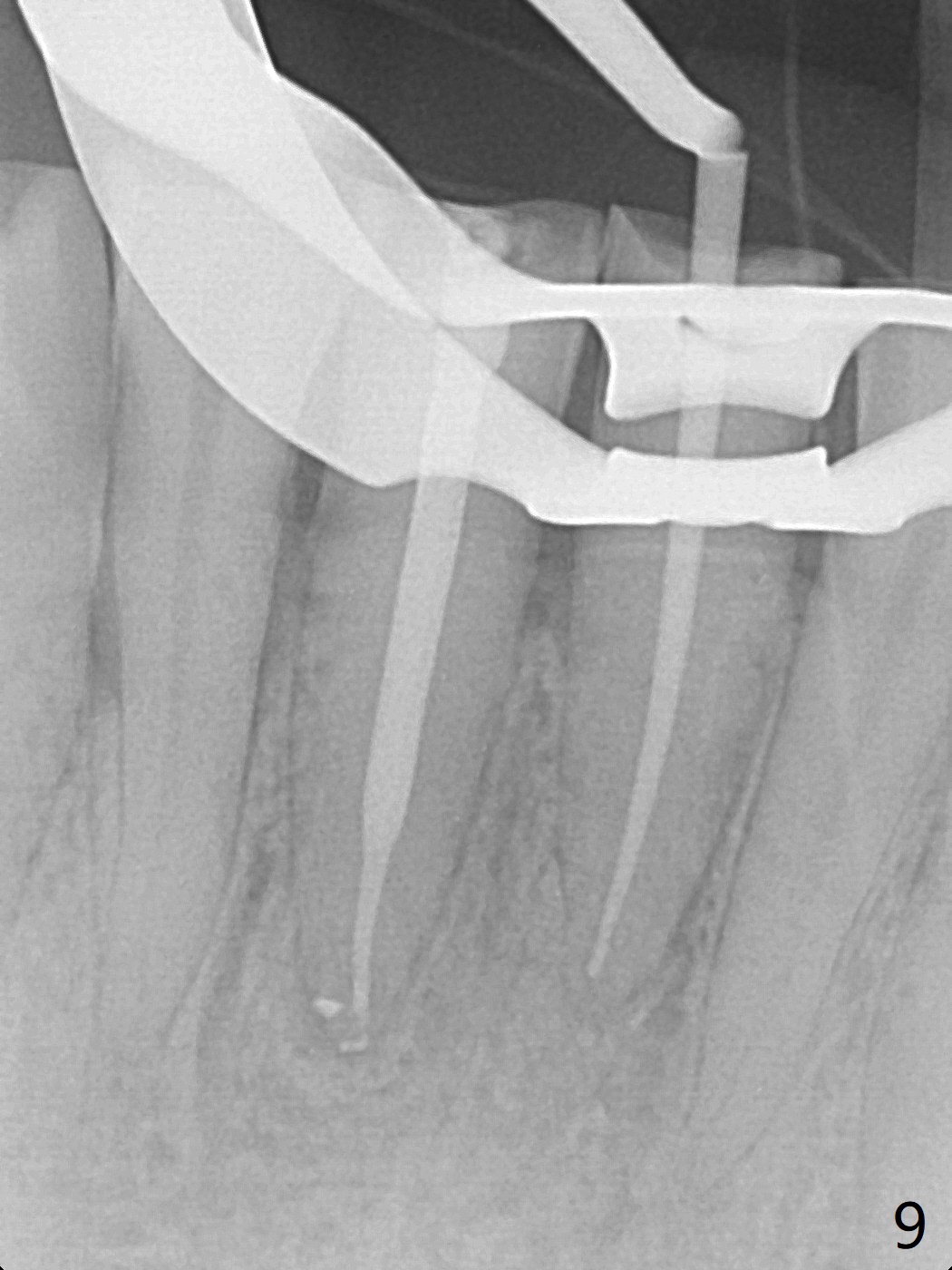
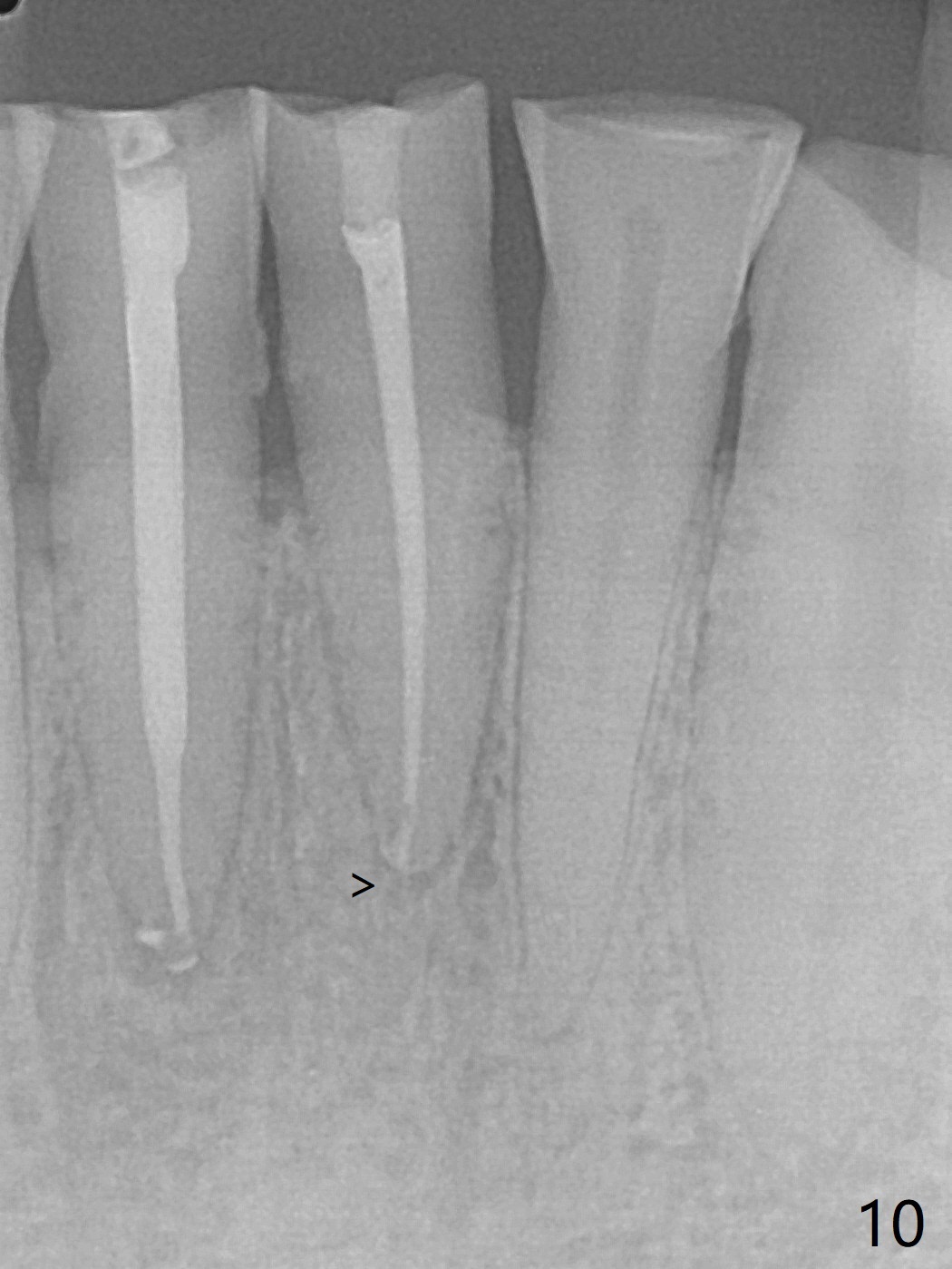
A 45-year-old man has had a chronic fistula associated with the tooth #25 (Fig.1). There is purulent discharge sometimes. After debridement with hand files #10-20 and rotary one 30/06, a master cone 30/.06 is inserted incompletely (Fig.2). After rotary files 30/.08 at 16.0 mm and 30/.10 at 15.0 mm and hand files 10-20 at 17 mm, the master cone is apparently inserted to the WL. With application of Endo Sequence Sealer (syringe), the master cone is reinserted (Fig.3). When the rubber dam is removed, the sealer is found to have expelled from the fistula. With an endo curette (Fig.5), the sealer is removed from the deepest portion of the sinus tract (apex of the tooth). What do you want to know the outcome of the supplementary surgical maneuver? The sealer is gone (Fig.6). The immediately supplementary treatment avoids a separate apicoectomy. No fistula is noted <2 weeks postop (Fig.7). The attrition is due to #8 and 9 veneers, fabricated 8 years earlier. The tooth #24 is symptomatic with loss of incisal composite nearly 4 years postop (Fig.8 <). After 30/.04 gutta percha (GP) try in (Fig.9), RCT is finished without accessory GP (Fig.10).
Return to Professionals Xin Wei, DDS, PhD, MS 1st edition 10/16/2016, last revision 09/01/2020