





|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
How to Prepare 2nd RCT Procedure?
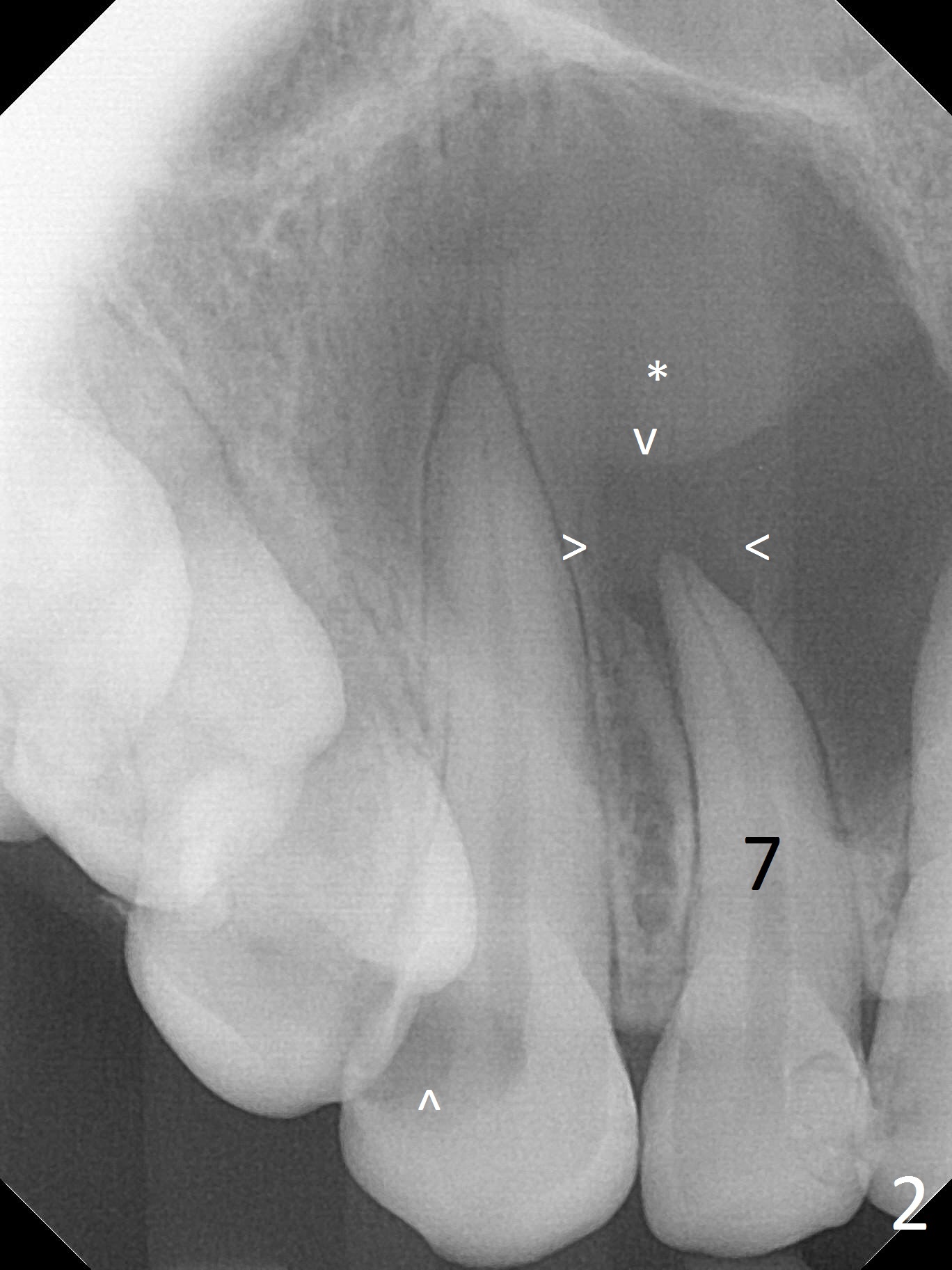
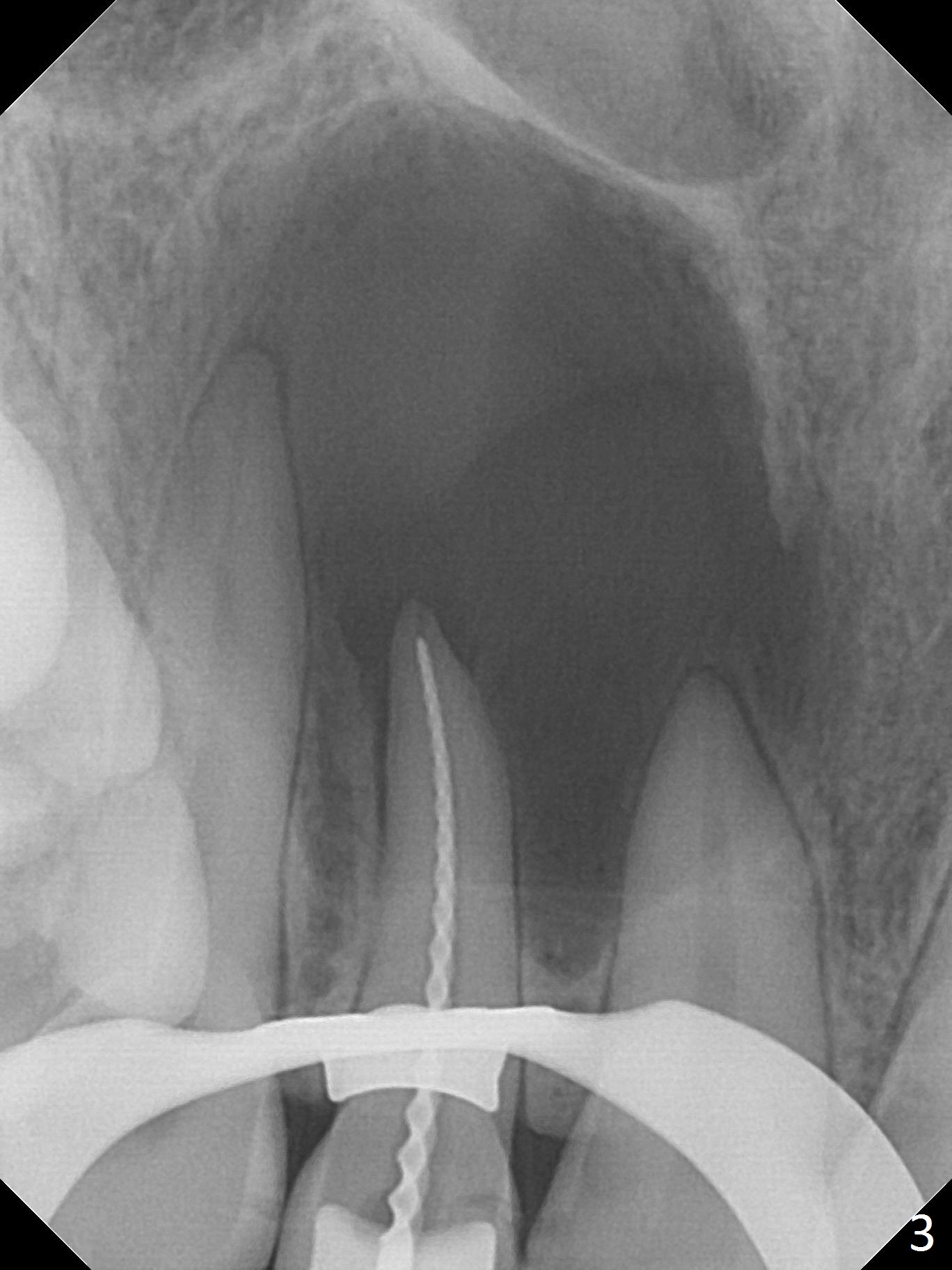
A 30-year-old woman presents to clinic with a large palatal swelling (Fig.1,2). In fact the tooth #7 is necrotic with a periapical radiolucency (Fig.2 arrowheads). RCT is initiated; note the curved canal and file (Fig.3). To reduce the large lesion, Calcium Hydroxide paste is placed in the enlarged canal (Fig.4 *). In a month, the palatal lesion decreases (Fig.5). After re-debridement of the canal, Calcium Hydroxide paste is re-applied.
Since the tooth is nonvital, the 2nd RCT procedure does not require local anesthesia for rubber dam placement. Prepare the largest size of hand file used last visit (read the note). In this case, remind the busy doctor of prebending the file and of the working length. Prepare Calcium Hydroxide paste with a large gauge needle.
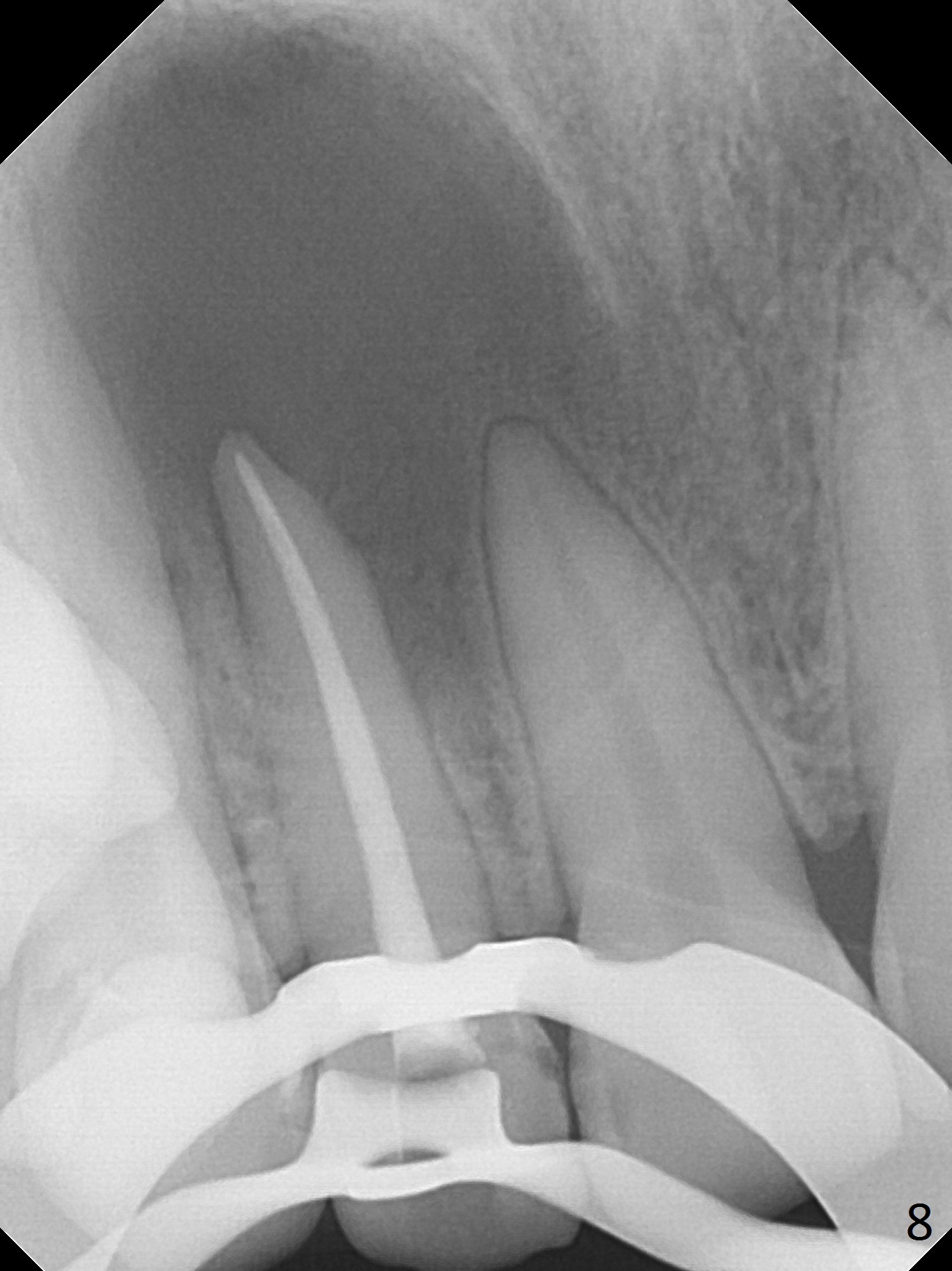
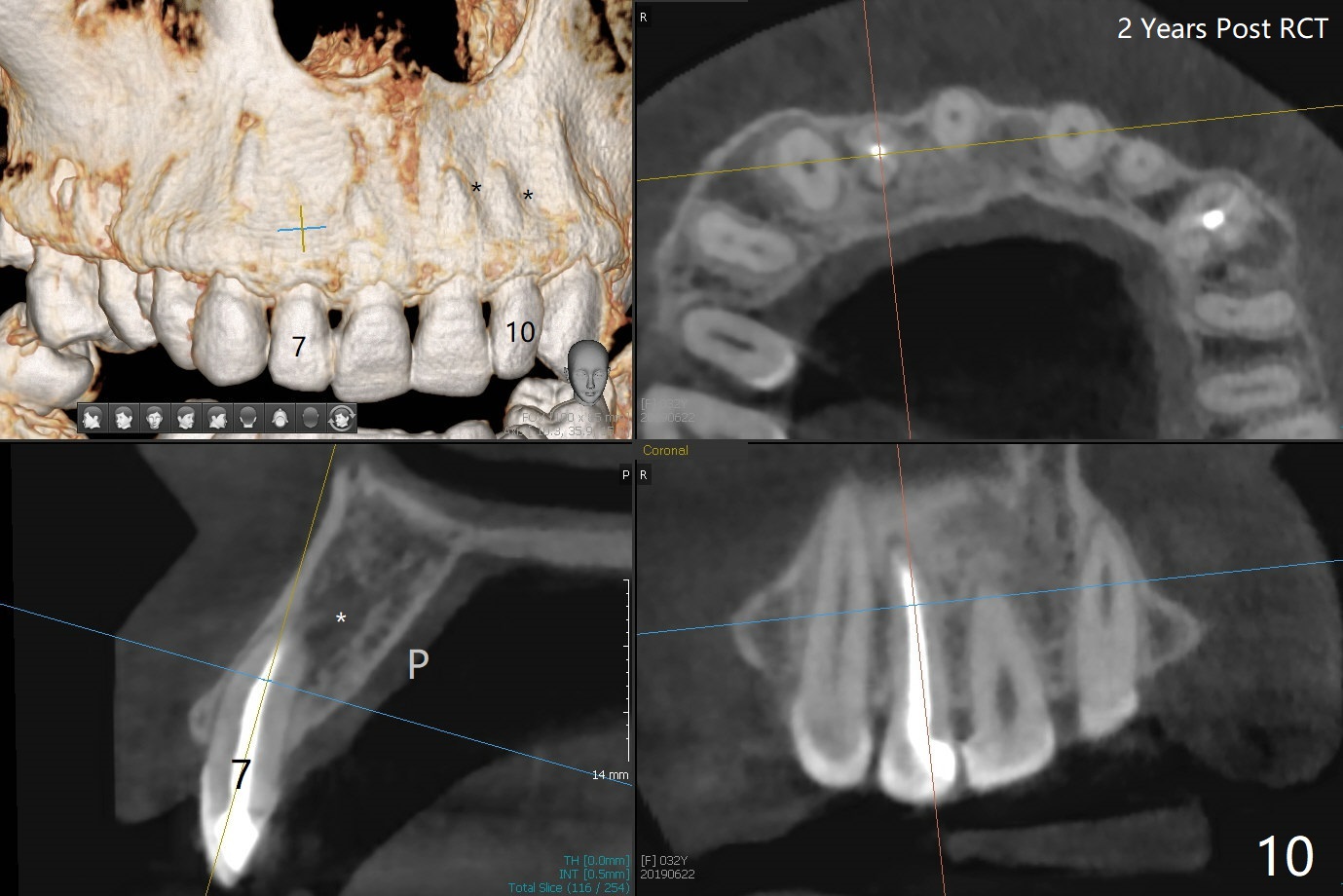
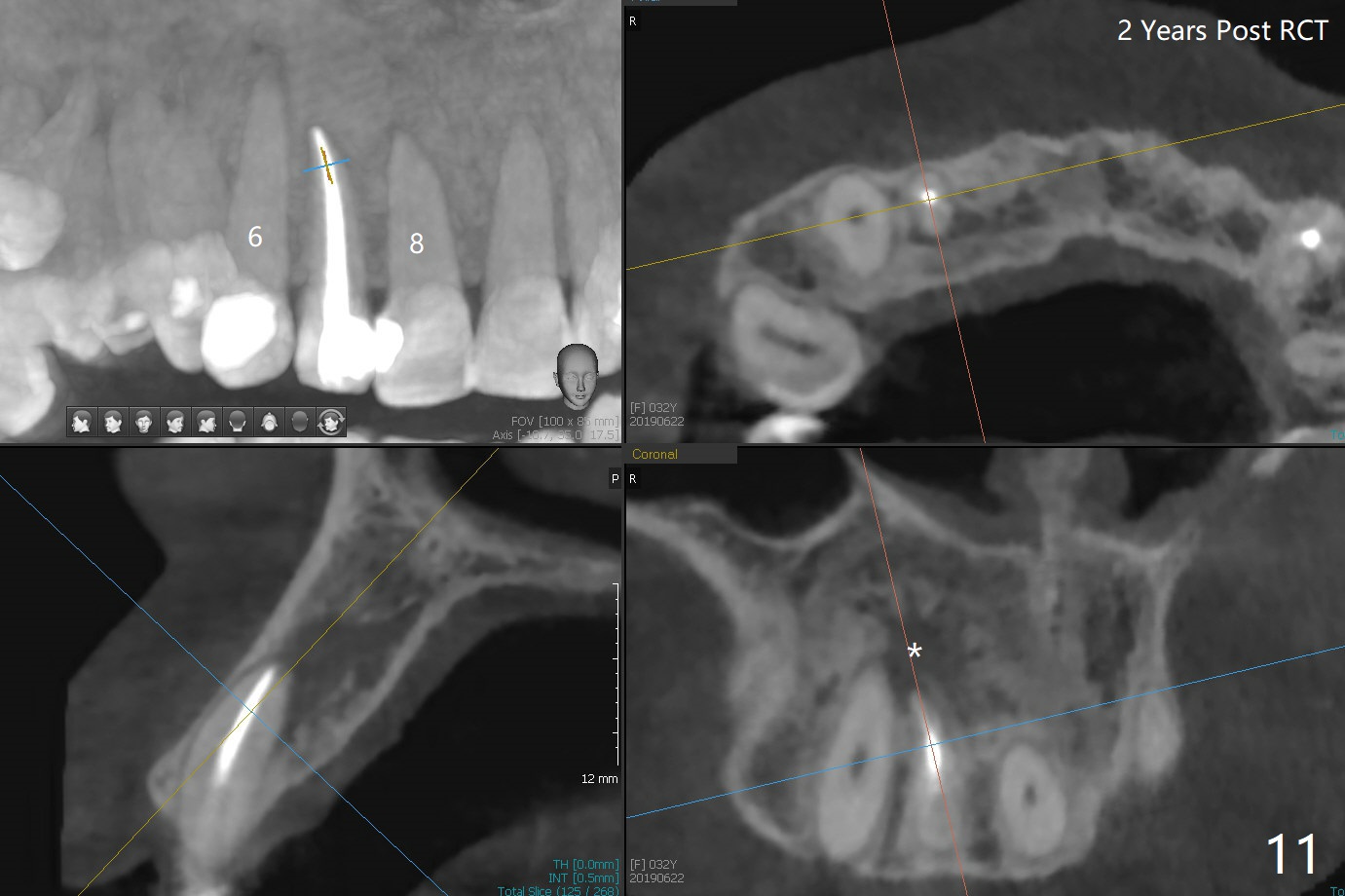
When this patient returns with improvement of symptoms, RCT will be finished. In fact the swelling relapses a month later (Fig.6). After discussion of possible cyst enucleation and increase in debridement from 30/.04 to 40/.06, a master cone of 40/.06 is inserted (Fig.7) and RCT is finished (Fig.8). Although the patient reports relapse of swelling, the palate looks normal and bone density increases 7 months postop (Fig.9). For 14 implant placement, CT is taken 2 years 1 month post RCT (Fig.10,11). Radiolucency is confined to the apex of the tooth #7 (white *). The labial concavities mesial and distal to the left lateral incisor makes radiolucencies (bone loss) look more radiolucent, creating globumaxillary cyst image. The globumaxillary cyst is a terminology for its shape. It does not mean congenital in nature. The treatment is dependent upon vitality test of the involved teeth.
Return to Professionals 2nd Case Xin Wei, DDS, PhD, MS 1st edition 04/14/2017, last revision 03/01/2021