




|
|
|
|
|
|
|
|
|
|
Why does RCT Fails in Abutment Tooth?
Fifty-four-year-old lady has a three-unit FPD involving #30-32 for 20 years. An acute infection develops in #32 abutment tooth with periapical radiolucency (Fig.1 *). Mesial and distal root canal fillings are short (black <). The pulpal chamber is not filled (white >). At higher magnification, the mesial margin is open. Additionally, the tooth #1 is missing. It appears that the tooth #32 has guarded prognosis. Treatment plan is to extract #32 and place an implant at #31.
In fact, the retainer is separated from #32 abutment when the FPD is being sectioned between #30 retainer and #31pontic. The mesiobuccal open margin of the tooth #32 is evident (Fig.2,3 yellow <). It appears that the crown was seated on the composite-like material, instead of sound tooth structure. There is void around the post (Fig.2 white >). Furthermore, the mesial canal seems to be not well condensed (curved void, Fig.2 black <).
The void in the mesial root turns out to be a missing mesiobuccal canal (Fig.4,5 black <). Initially, RCT filling material is difficult to remove from apical portion of the distal and mesiolingual canals (Fig.4 white >), while the apical portion of the mesiobuccal canal is obliterated.
The most apical portion of the distal canal is found to be blocked (Fig.5 white >) when filling material is removed. The blockage is pre-existing, since it is present in Fig.2 and 4. The mesiobuccal canal (Fig.5 black <, #10 hand file) fuses with the mesiolingual canal (*, 30/.06 rotary file) before exit at apical foramen.
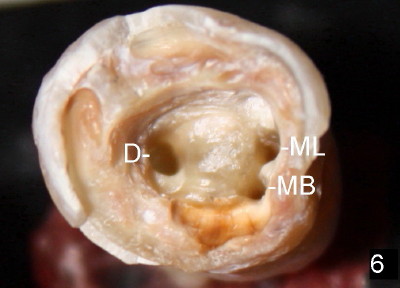
Fig.6 show the pulpal chamber with three orifices: MB (mesiobuccal), ML (mesiolingual) and D (distal) near the end of canal debridement.
In brief, RCT failure in this case is both endodontic (short fill, and missing MB canal) and restorative (coronal leakage: crown open margin, no filling material/cement in pulpal chamber and around the post).
Xin Wei, DDS, PhD, MS 1st edition 09/20/2011, last revision 10/02/2011