


|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Size Difference between Bone Expander and Implant
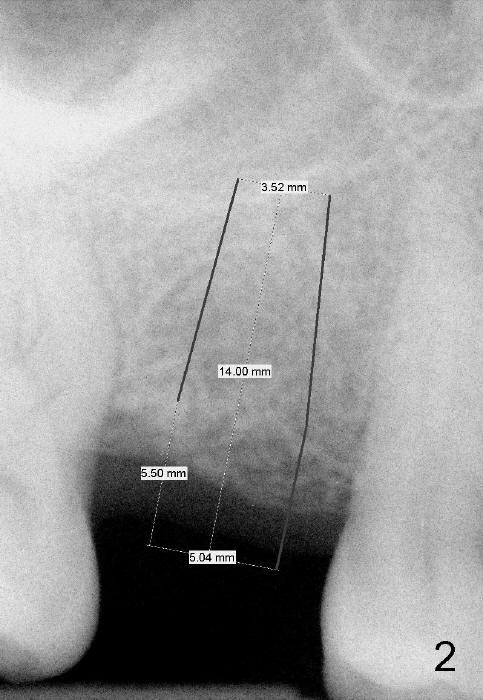
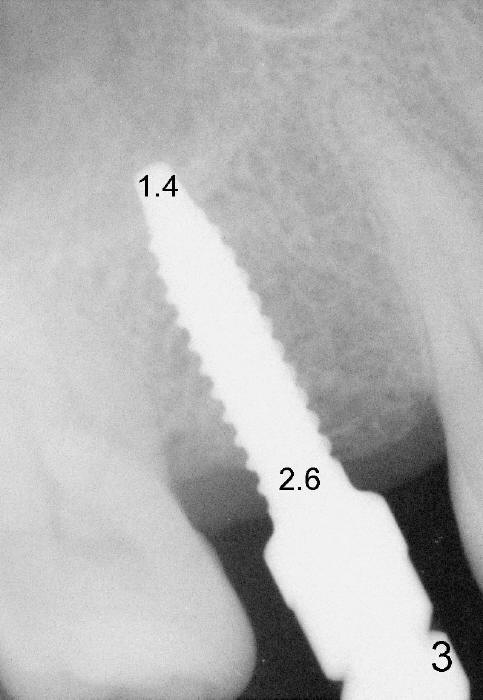
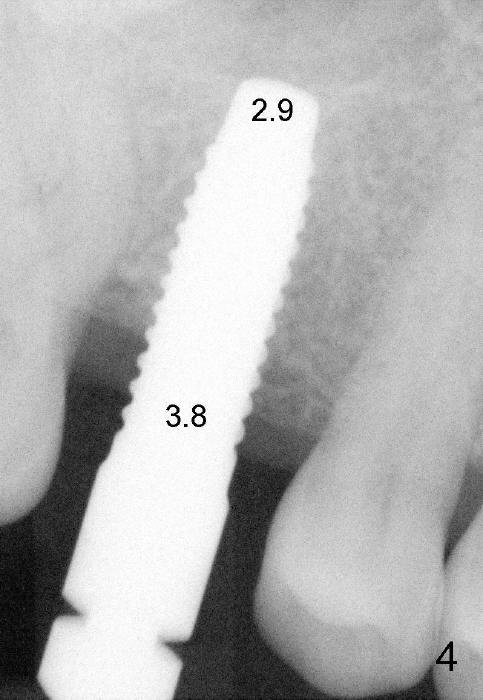
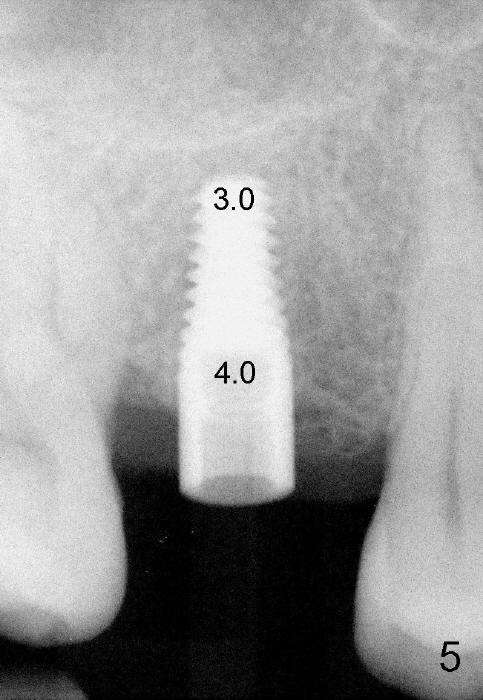
The 42-year-old lady is a dental phobic. The tooth #3 (residual root) is extracted 3.5 years ago. Finally she returns for implant (Fig.1). The mesiodistal space allows to place a 5x14 mm implant (Fig.2). Bone density is felt low when a 1.6 mm pilot drill is used. Bone condensation proceeds with bone expanders 2.6 mm (Fig.3) to 3.8 mm (Fig.4) 12 mm deep. Bone density is felt to increase with each larger expanders. When a 4x11 mm implant is placed (Fig.5), the insertion torque is 15 Ncm. When the diameter and length of the implant increase (Fig.6), the insertion torque is >60 Ncm. To have primary stability, the implant should be two sizes larger than the last expander (compare Fig.4,6)! In addition, the majority portion of the expanders is cylindrical (Fig.3,4), whereas the implant is tapered (Fig.5,6).
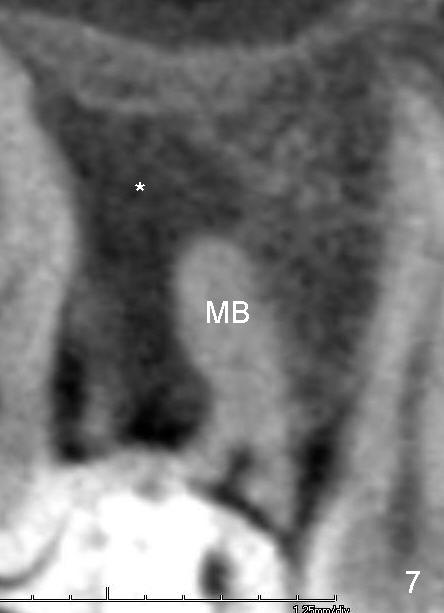
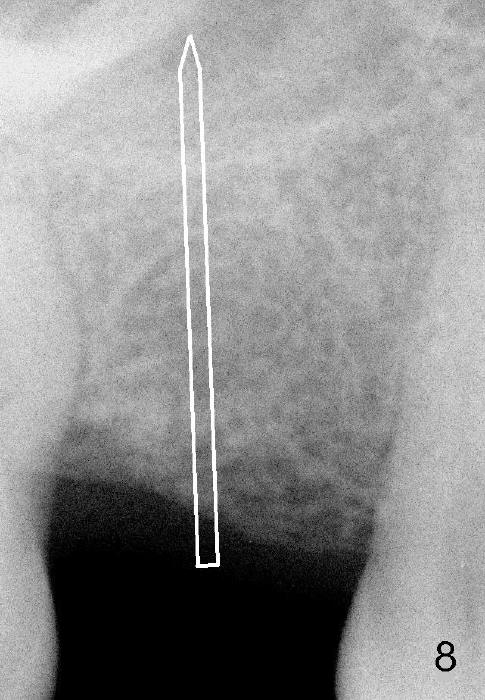
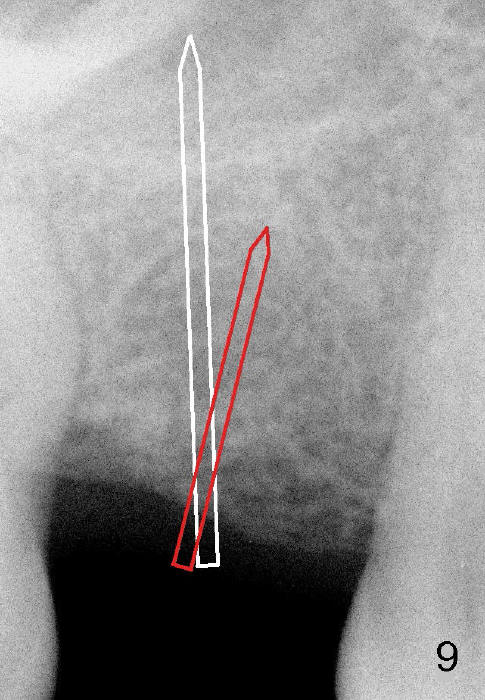
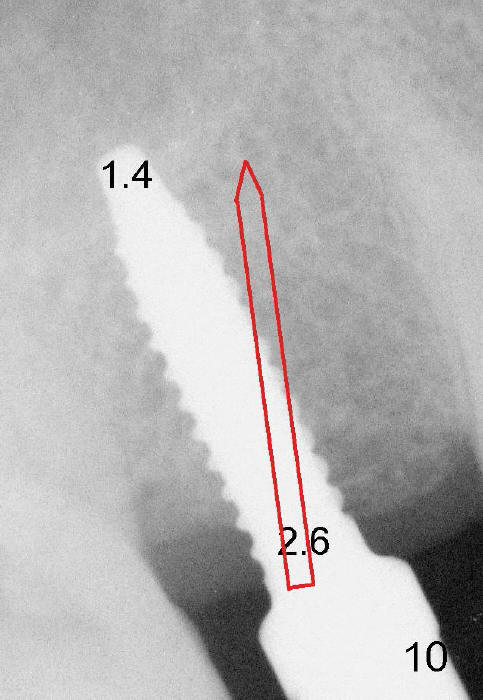
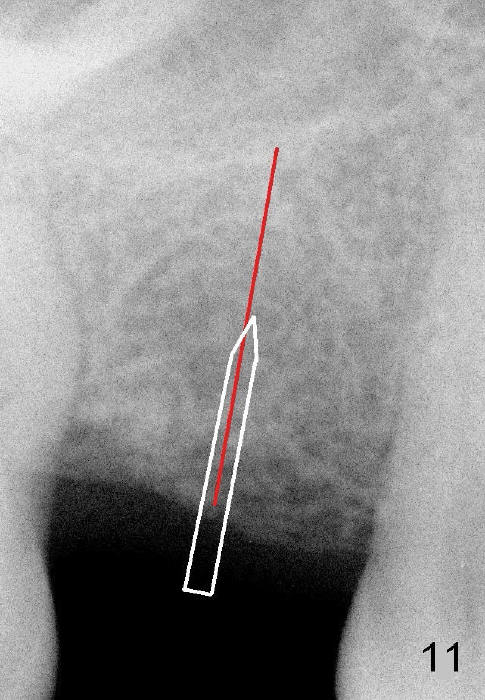
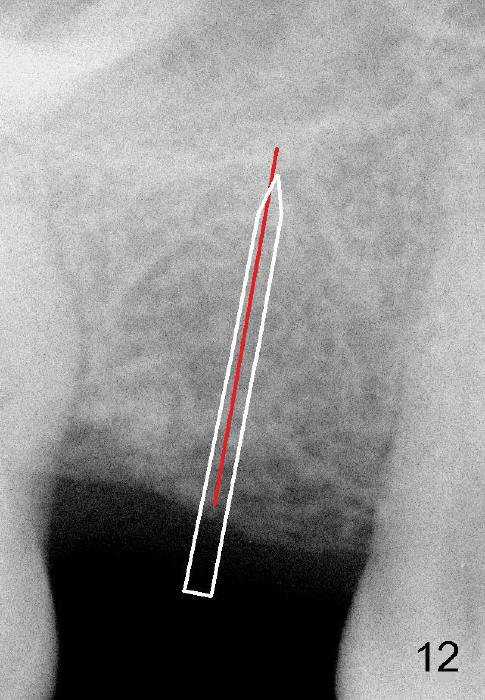
Another drawback of the implant placement is that the trajectory is off and distal (Fig.3-6), probably due to the low bone density in the distal aspect of the socket prior to extraction (Fig.7 CT sagittal section; MB: mesiobuccal root). The pilot drill must inadvertently have drifted distally and to the less dense bone (Fig.8). If it had been found, it could have been corrected early (Fig.9 red arrow). The trajectory could have been corrected immediately after the 2.6 mm expander (Fig.10). Ideally the pilot drill (Fig.11arrow) should be placed slightly mesial to the presumably mid edentulous line (red line) and only half of the length. If the trajectory is right, continue osteotomy (Fig.12). If not, correct it immediately.
The patient returns for restoration 7 months postop; there is no bone loss (Fig.13).
Return to Sinus Lift,
Instrument, Follow-Up
Xin Wei, DDS, PhD, MS 1st edition 12/12/2014, last revision 08/22/2019