


|
|
|
|
|
|
|
|
|
|
|
|
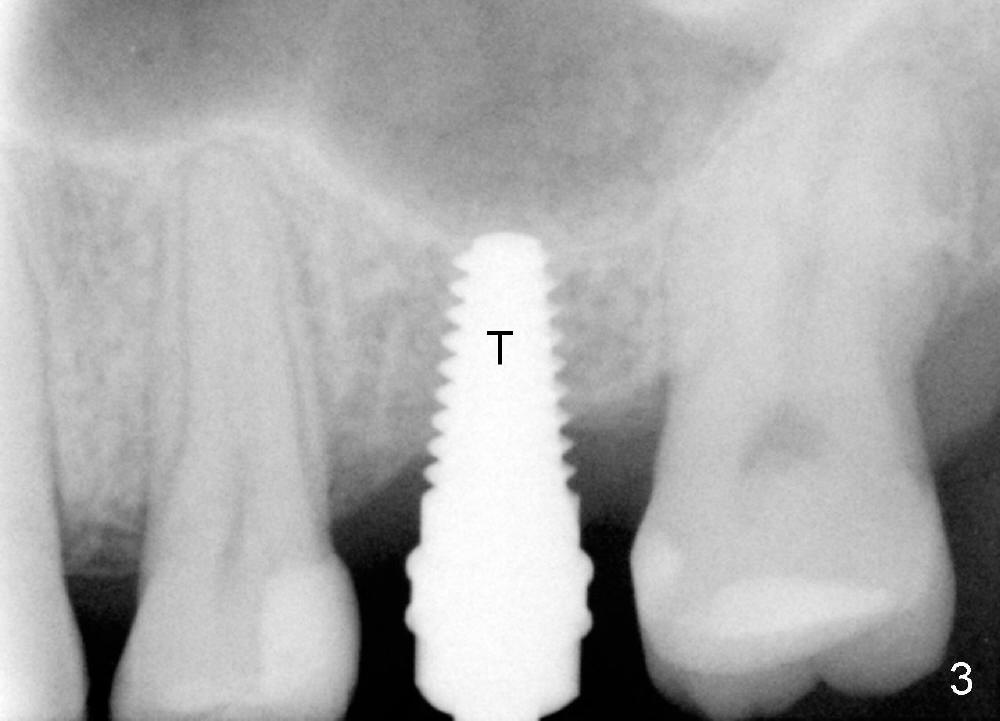
Sinus Lift When Bone Density is High
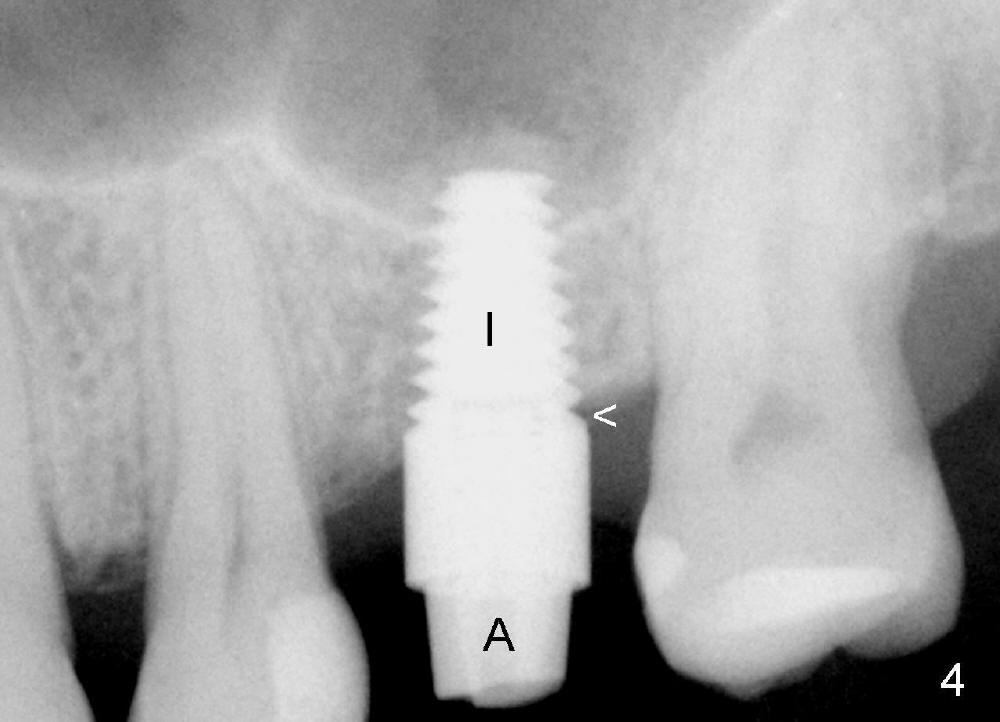
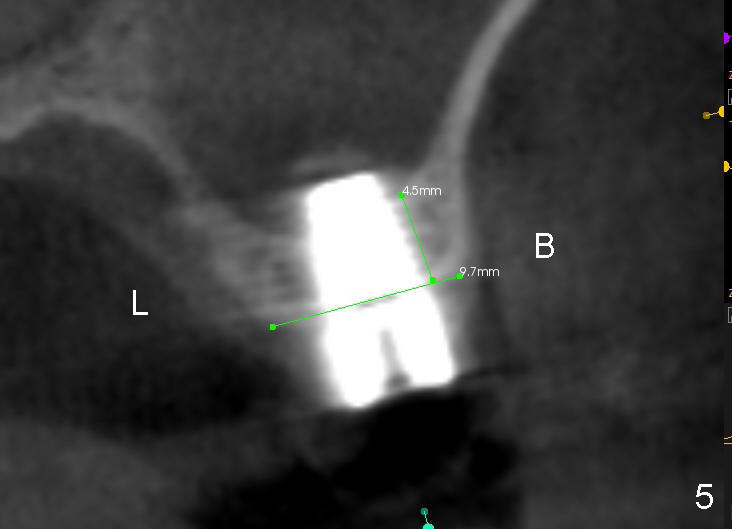
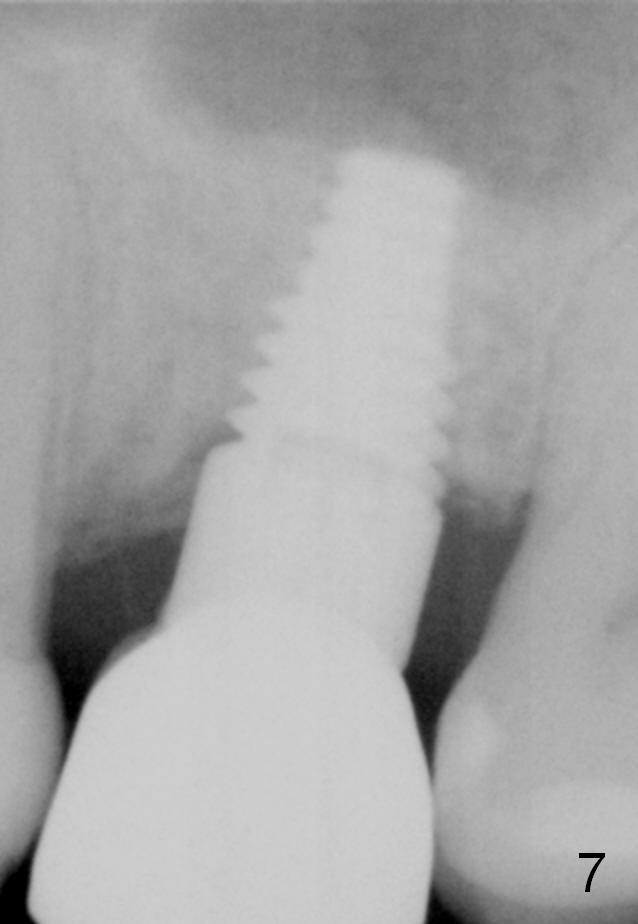
A 48-year-old lady has lost #14 for a while (Fig.1). It looks that bone density at the site of #14 is lower than that mesial to the 2nd premolar. The buccolingual width is wide clinically, although the mesiodistal distance is short (8 mm, Fig.2). A 4-mm tissue punch is used for access. When 1.5 mm pilot drill is used to start osteotomy, it feels that bone density is not low. The first bone expander (2.6 mm) cannot penetrate the bone. Therefore reamers 2.5-3.5 mm are used to increase osteotomy at the depth of 6 mm from the gingival margin. A 4.5x11 mm tap drill is inserted ~ 7 mm with resistance (Fig.3). After 5x11 mm tap, autogenous bone mixed with Osteogen is pushed into the osteotomy and upward. A 5x11 mm implant is placed with > 60 Ncm (Fig.4). After the last X-ray, the implant is torqued 5 more times so that the distal last thread may be able to be fully engaged to the bone. Fig.5 is CT coronal section at the site of #14 5 days postop (B: buccal; L: lingual). Fig.6 is taken 5 months postop with maintenance of sinus lift (*). The crown dislodges 16 months post cementation. In fact the abutment is also loose. The latter is resin bonded, followed by crown cementation (Fig.7). It appears that when the implant is 5 mm or less, the unipost should be permanently cemented in order to prevent crown displacement, particularly for a patient with bruxism and partial edentulism.
Return to
Sinus Lift,
Instruments,
#2-4,
#7,
CT F-U
Xin Wei, DDS, PhD, MS 1st edition 10/30/2014, last revision 08/05/2018