




|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|||||
Implant Placed in the Septum
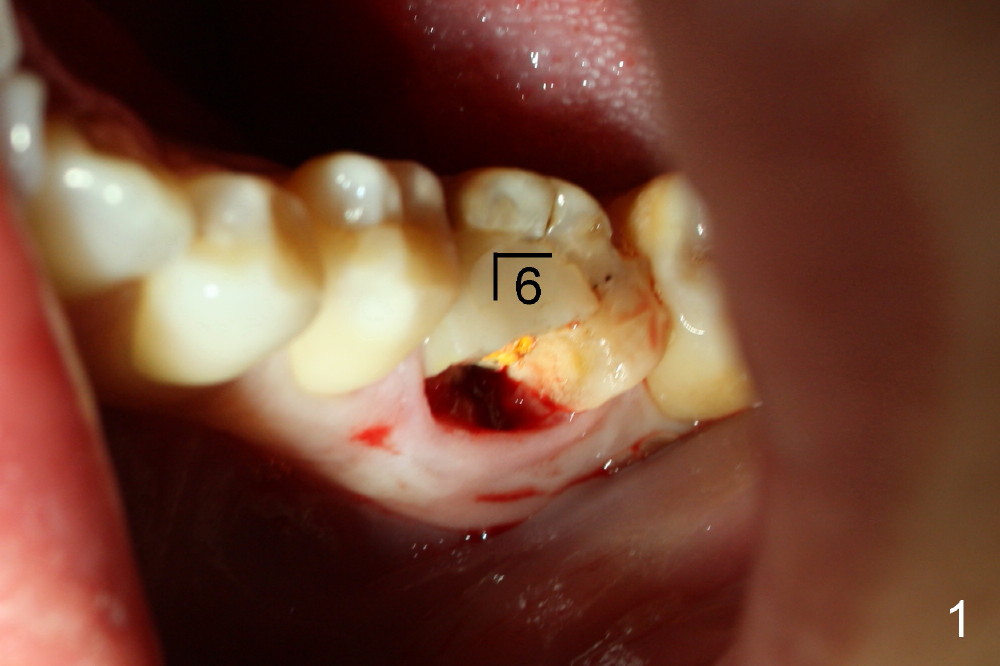
There are two methods to place an implant in the septum of the lower 1st molar: remove the crown (use roots as guidance) and remove the whole tooth. Today the 1st method is introduced.
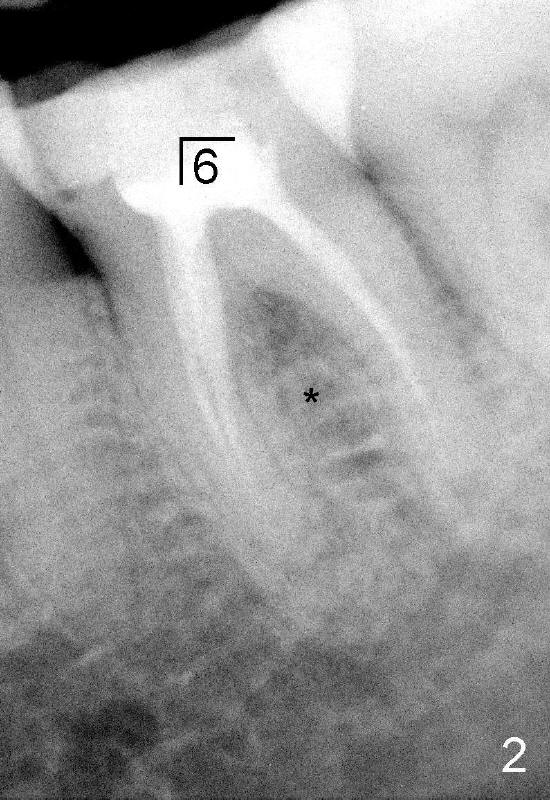
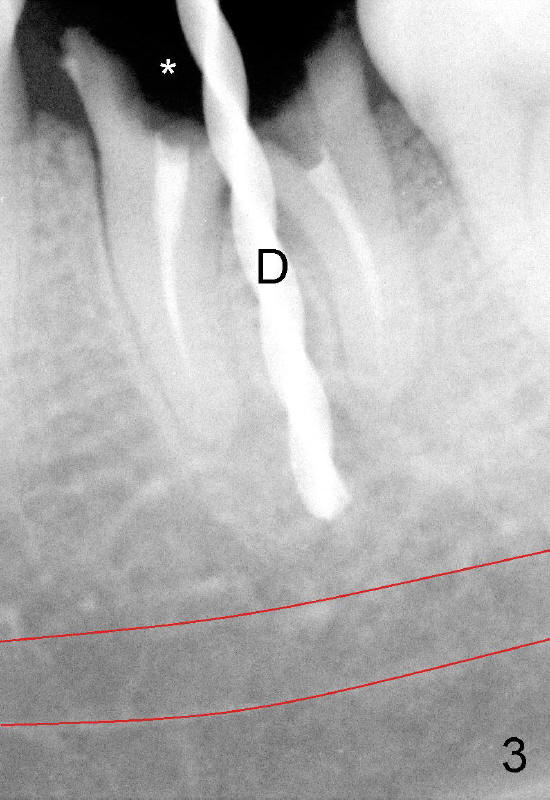
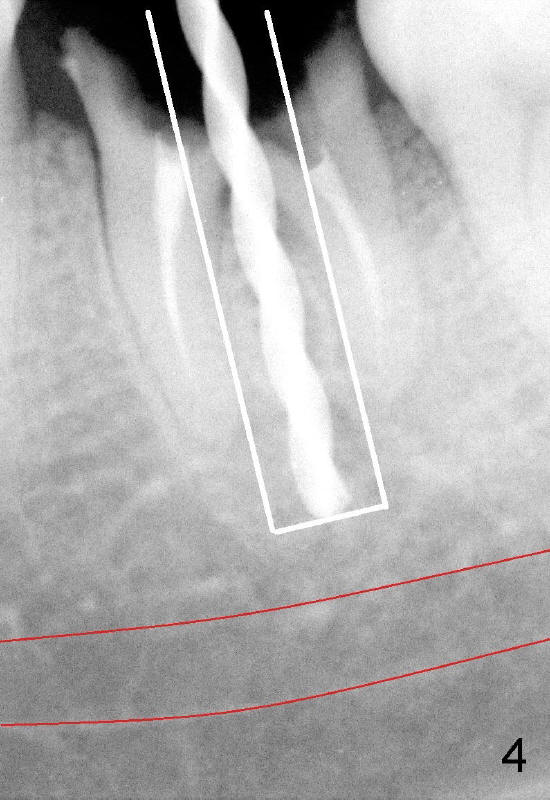
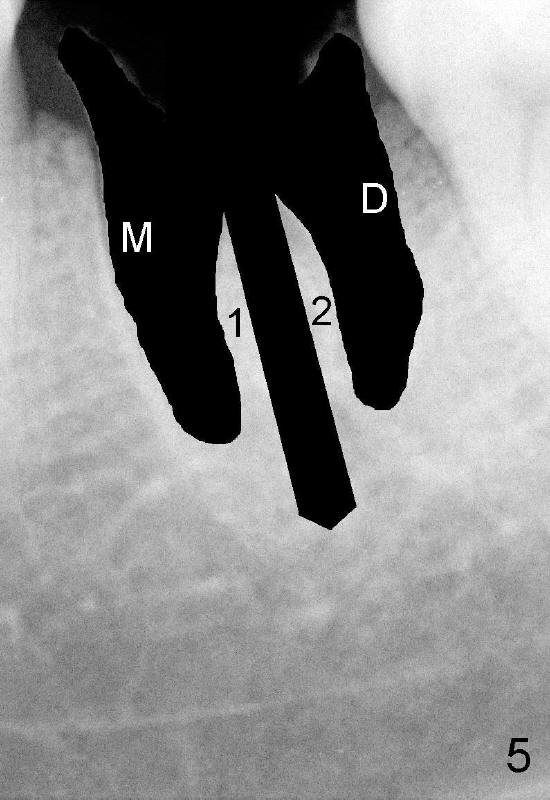
A 41-year-old lady fractures the crown of the lower left 1st molar (Fig.1.2). After removal of the remaining crown (Fig.3*) and exposure of the top of the septum, a pilot drill (D, 1.5 mm) is used to initiate the osteotomy. Drills with increasing diameters could be used to enlarge the osteotomy while the roots are in place (Fig.4: white rectangular outline).
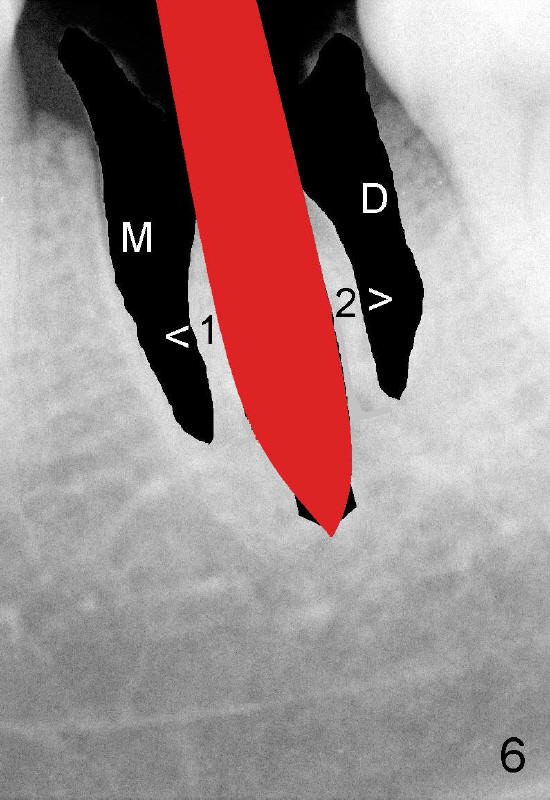
Instead, the roots are extracted (Fig.5). Using a variety of osteotomes (Fig.6: red) causes the mesial and distal segments of the septum (1,2) to be pushed into corresponding sockets (M,D).
Alternating with osteotomes, reamers (Fig.7: red) are used to enlarge the osteotomy and save the bone at the same time. Finally the harvested bone can return the shrinking sockets (1',2') prior to or after implant placement.
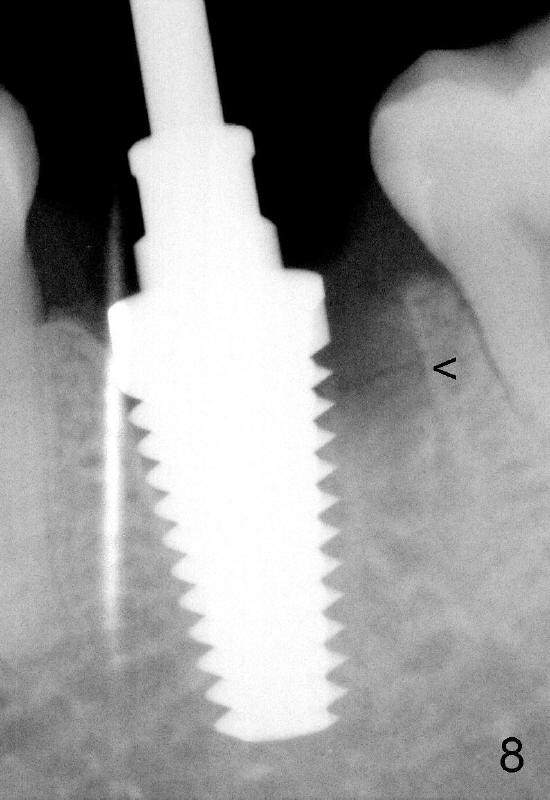
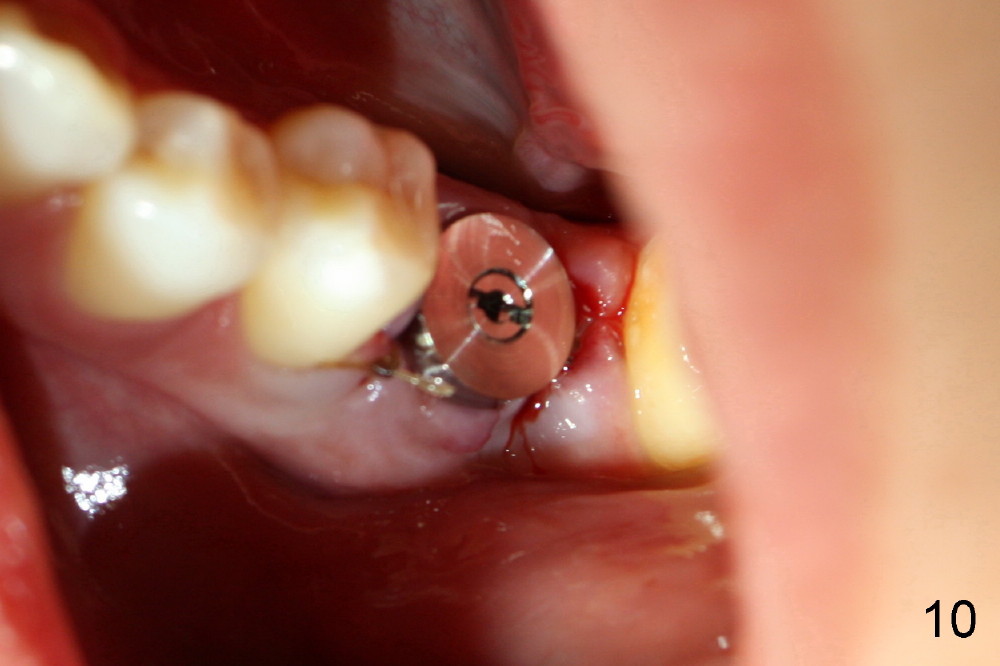
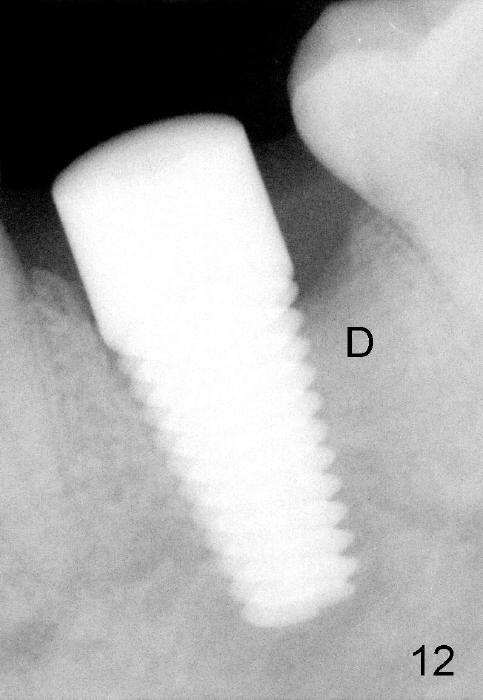
When 7x17 mm tap is placed, it drops mainly into the mesial socket (Fig.8). The septum appears to have been pushed to the distal one (<). When the 7x17 mm implant is placed with primary stability, the top portion is in the middle of the edentulous space (Fig.9). Sutures are placed mesial and distal to close the socket (Fig.10). The wound heals normally 3 months postop (Fig.11: ^). There is no bone resorption; the bone density on the top of the distal socket increases (Fig.12: D). The crown is fabricated 1 month later.
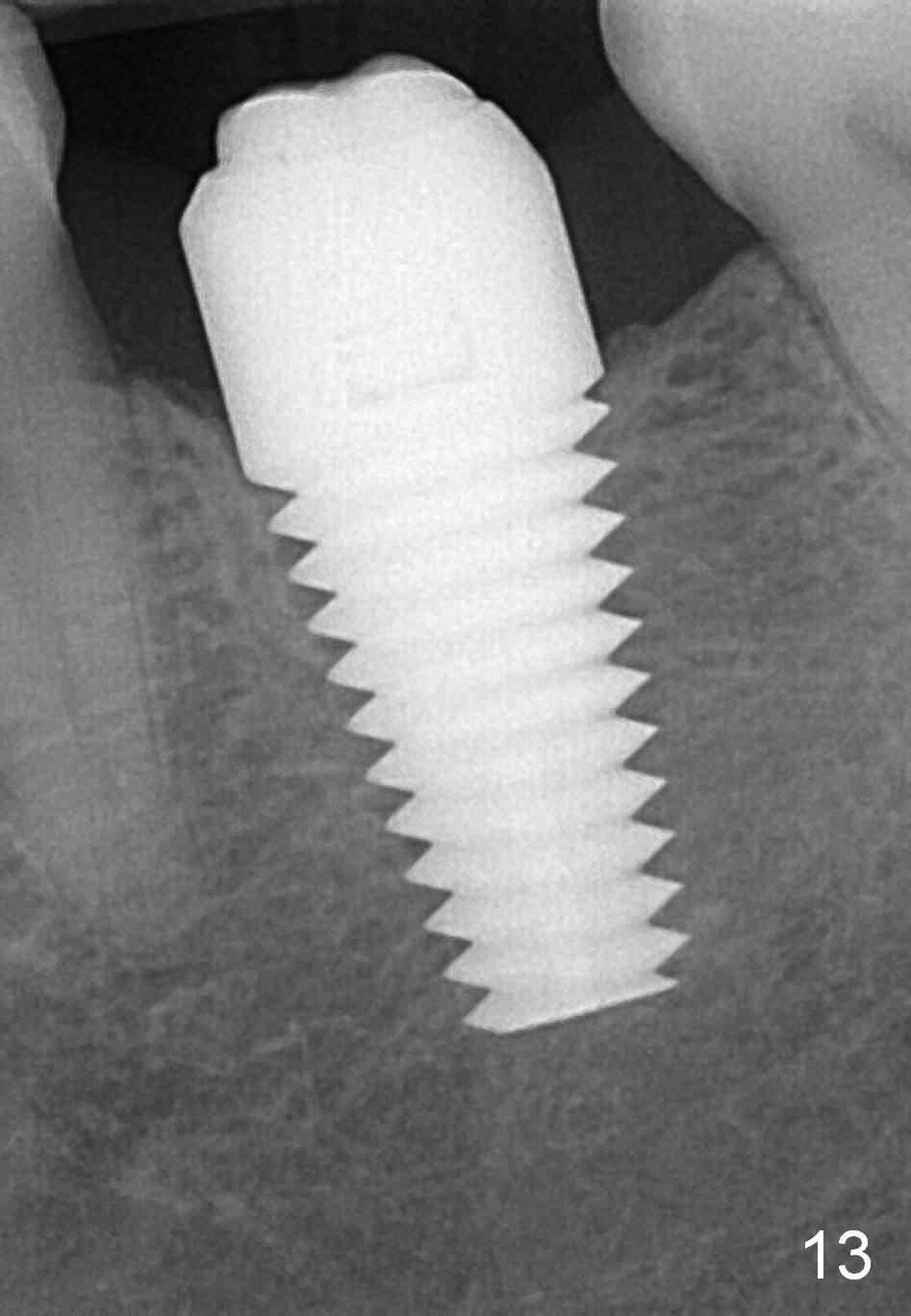
The Emax crown fractures 3.5 years post cementation; there is formation of the apparent lamina dura around the implant (Fig.13). There is no atrophy of papillae when the new crown is cemented (Fig.14 *). There is no bone loss nearly 4 years post cementation (Fig.15).
Xin Wei, DDS, PhD, MS 1st edition 03/24/2013, last revision 12/09/2017