



|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Upper 1st Molar Immediate Implant: Single Socket
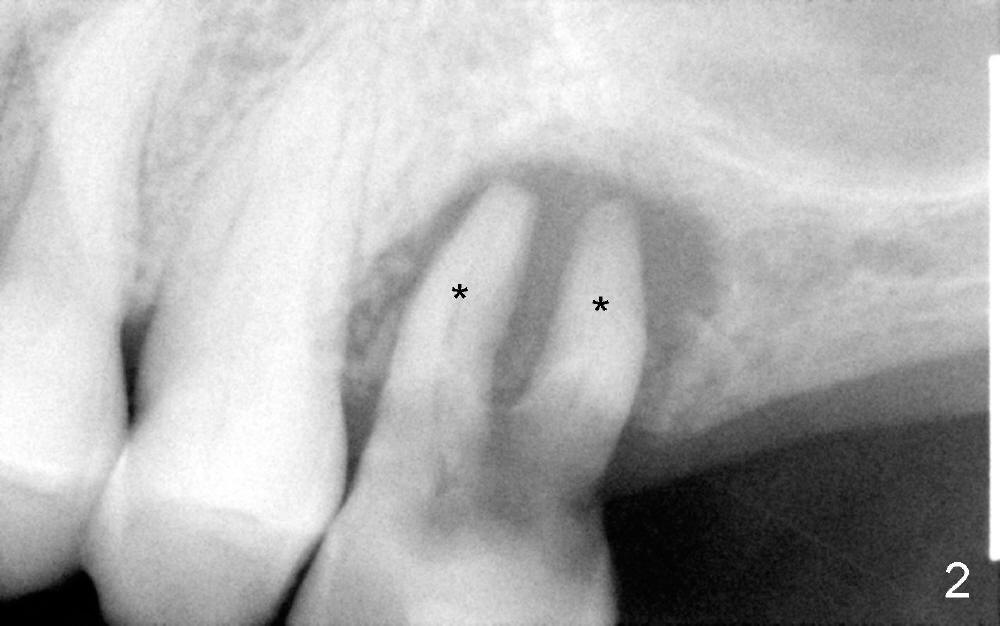
A 78-year-old lady has history of osteoporosis and history of taking Fosamax (Alendronate). Her upper left 1st molar needs extraction (Fig.1). The latter, appears to be easy, since the palatal root has lost. The remaining buccal roots have no bony support (Fig.2). Immediate implant should not produce extra trauma, leading to osteonecrosis.
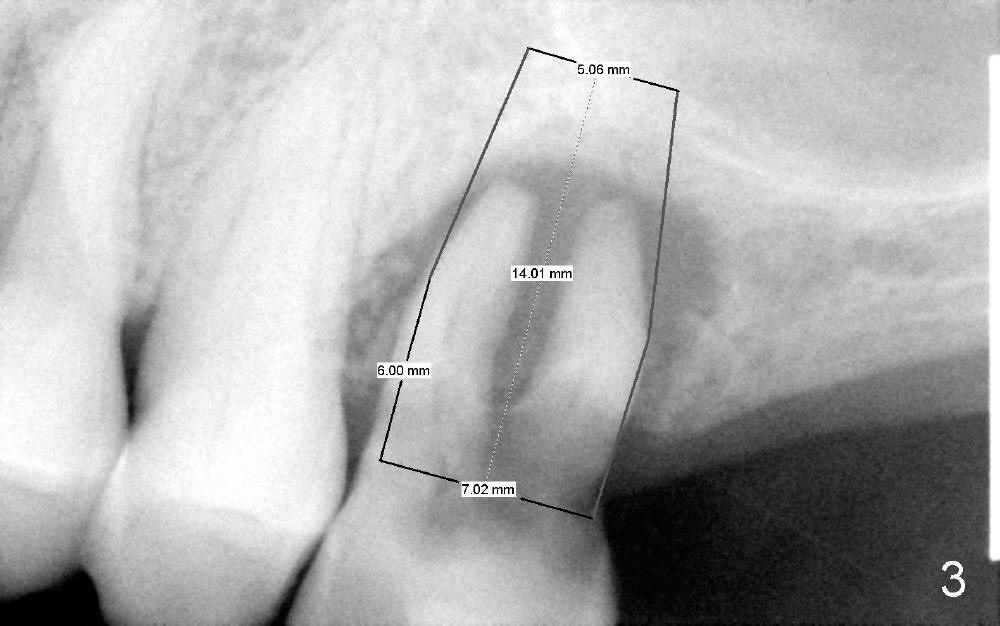
Since the socket is large, a large implant is planned to be placed (Fig.3, 7x14 mm) with sinus lift (penetrating the sinus floor for primary stability).
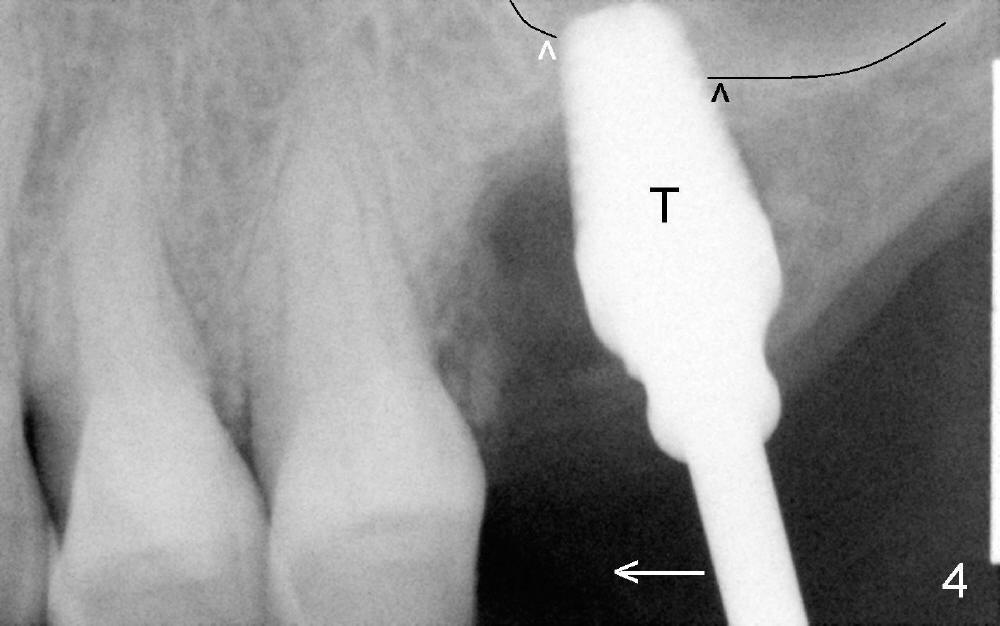
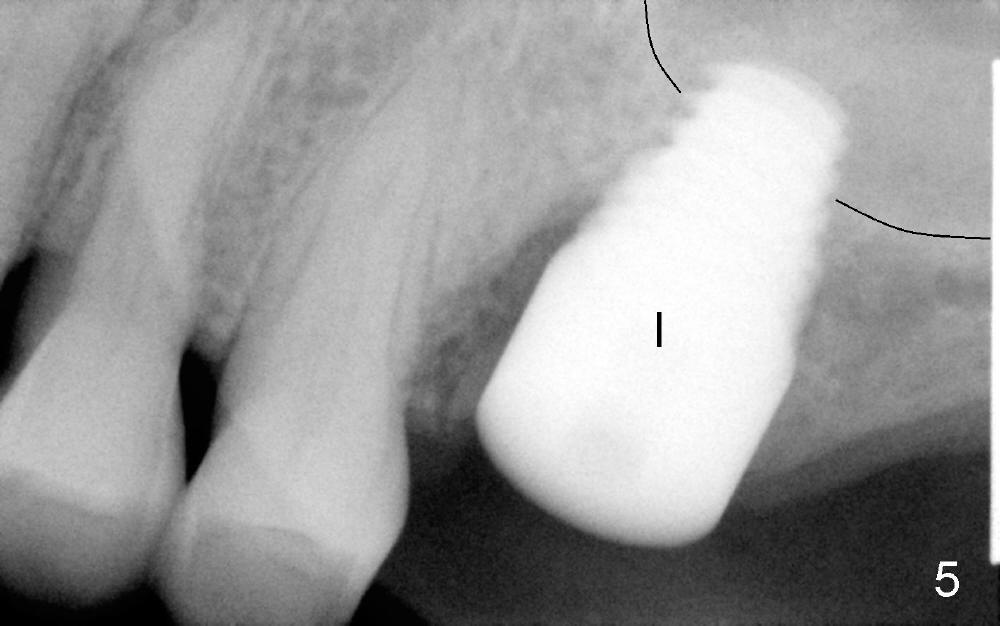
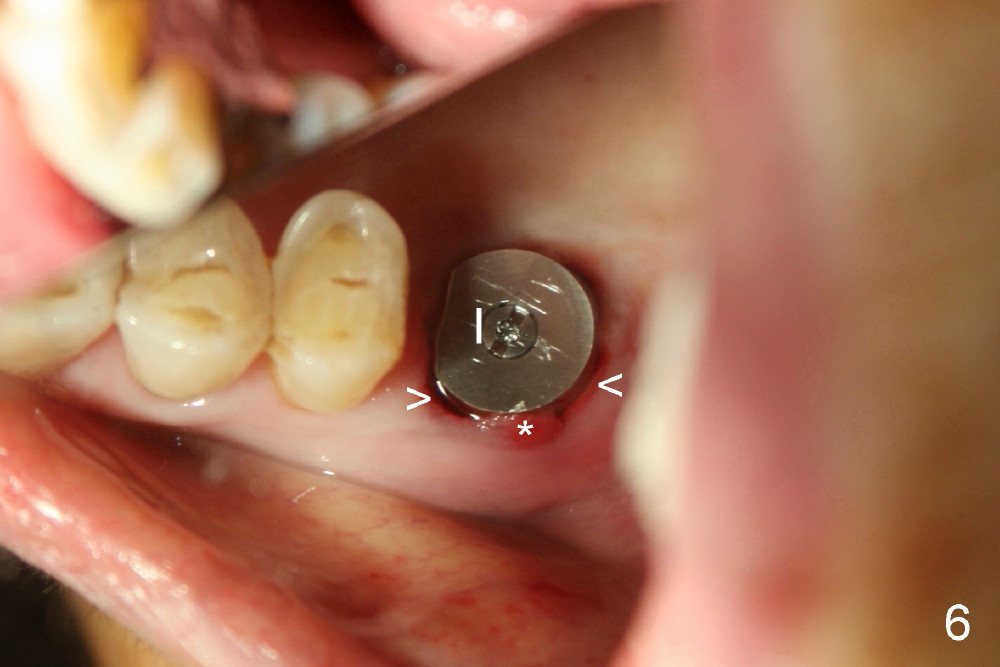
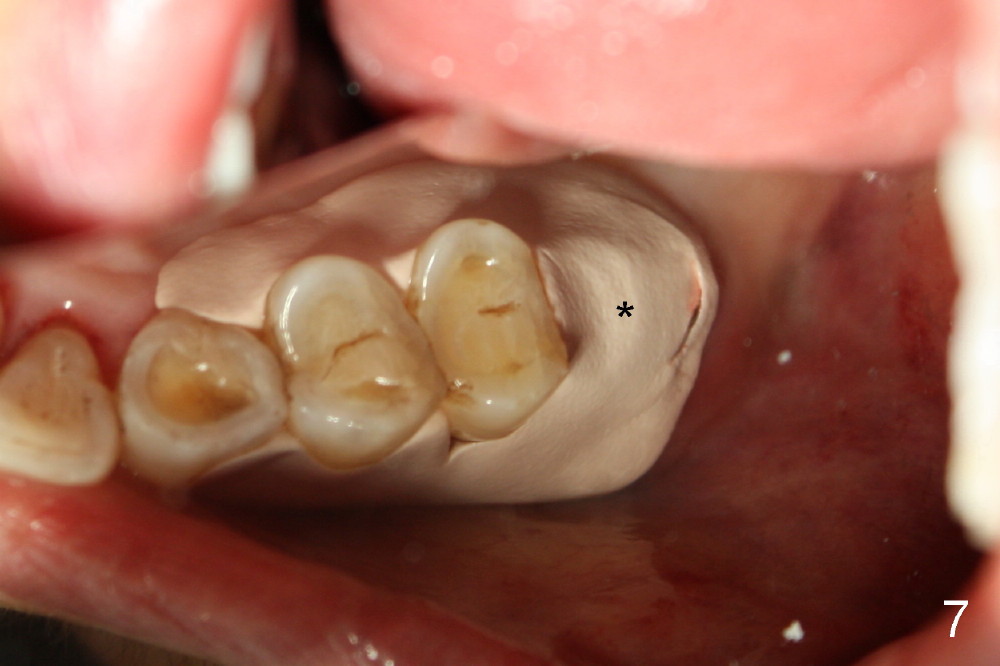
Extraction turns out to be simple with sectioning. After debridment of the socket and soaked with Clindamycin, the ostoeotomy forms using osteotomes, followed by insertion of a tap (Fig.4 T, 6x14 mm). After adjustment of the trajectory (Fig.4 arrow), larger taps are used (7x14, 8x14 mm) before placement of a 8x14 mm implant (Fig.5 I). There is small gap (Fig.6 arrowheads) around the implant. The wound is protected by perio dressing (Fig.7). The dressing is removed 7 days postop. Fig. 8 taken 2 weeks postop shows that the peri-implant gap has closed.
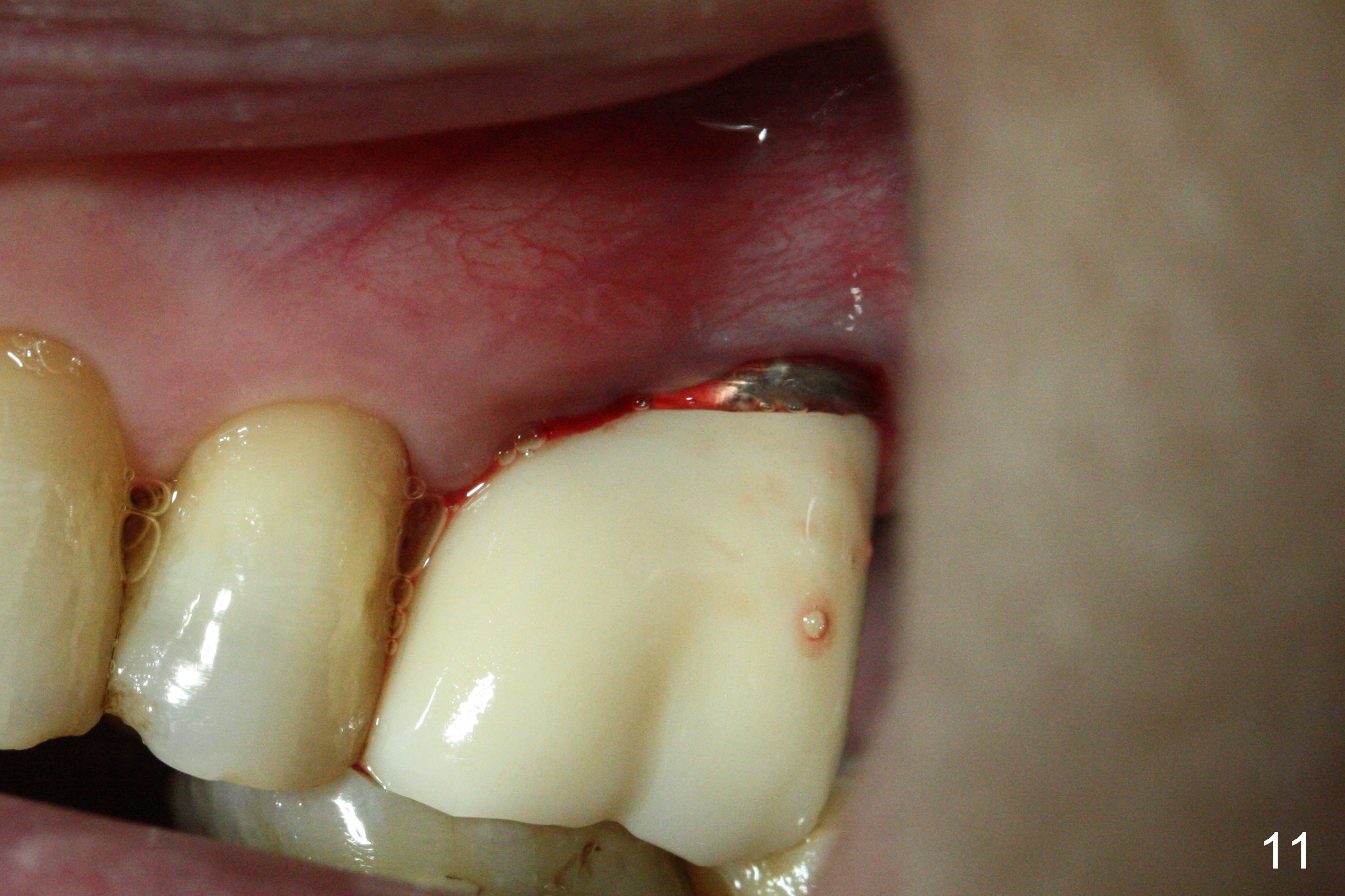
Crown is cemented 5.5 months postop.(Fig.9) and has been in function for more than 34 months (Fig.10,11).
Return to Upper Molar Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 05/31/2013, last revision 10/04/2016