









|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|||
|
|
|
|
|||
|
|
|
|
|||
|
|
|
|
|||
|
|
|
||||
Rebuild Buccal Plate
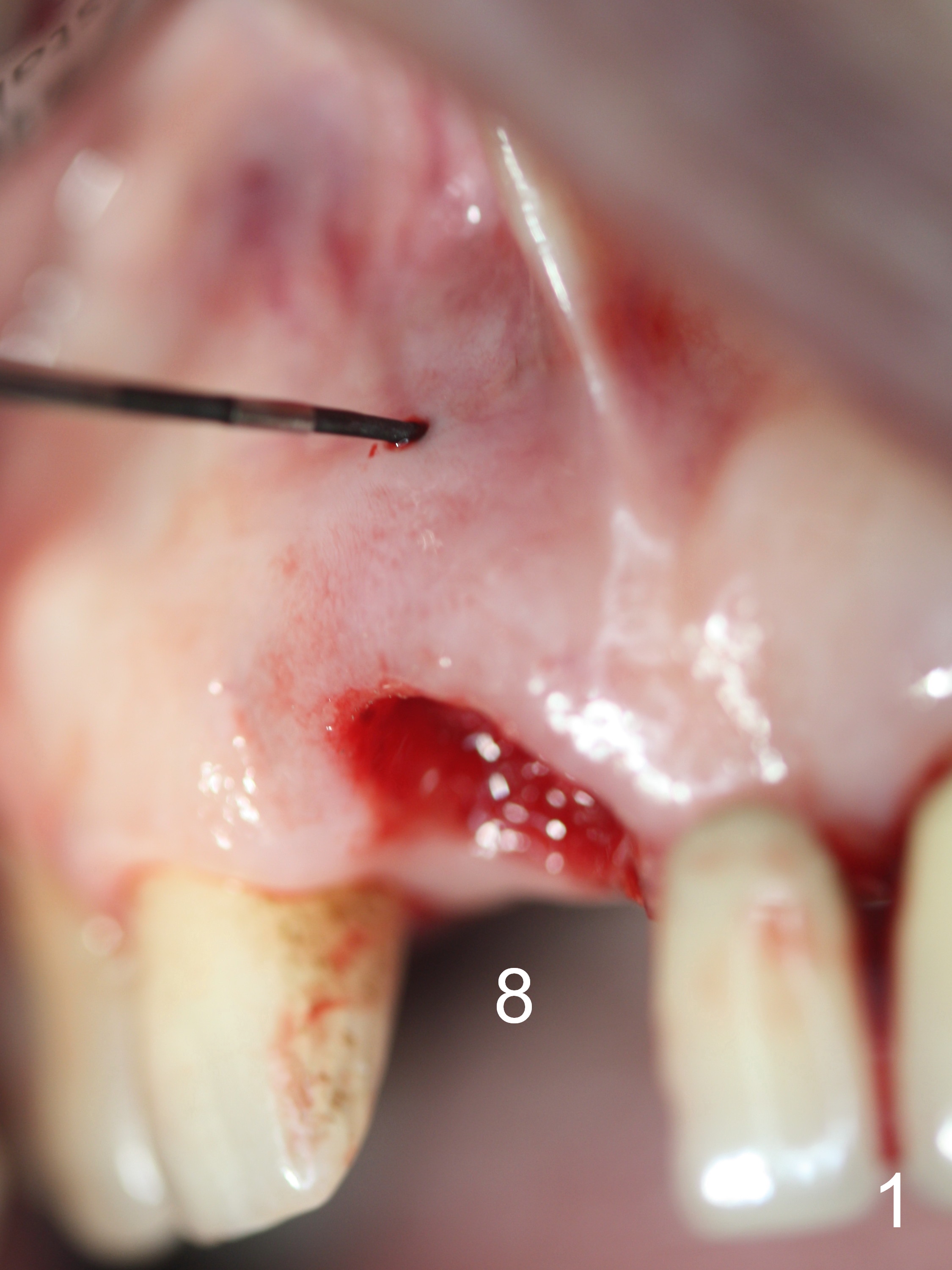
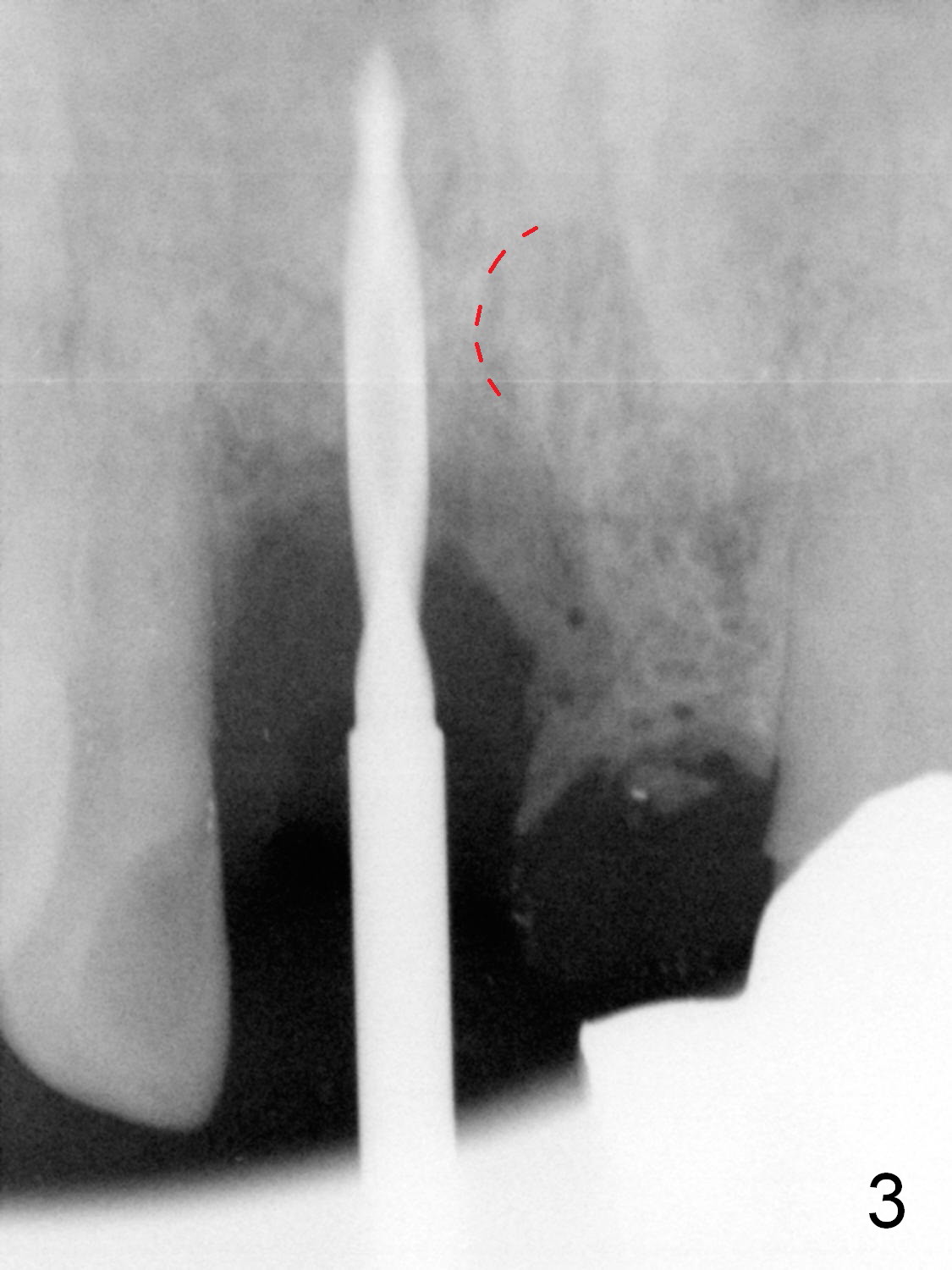
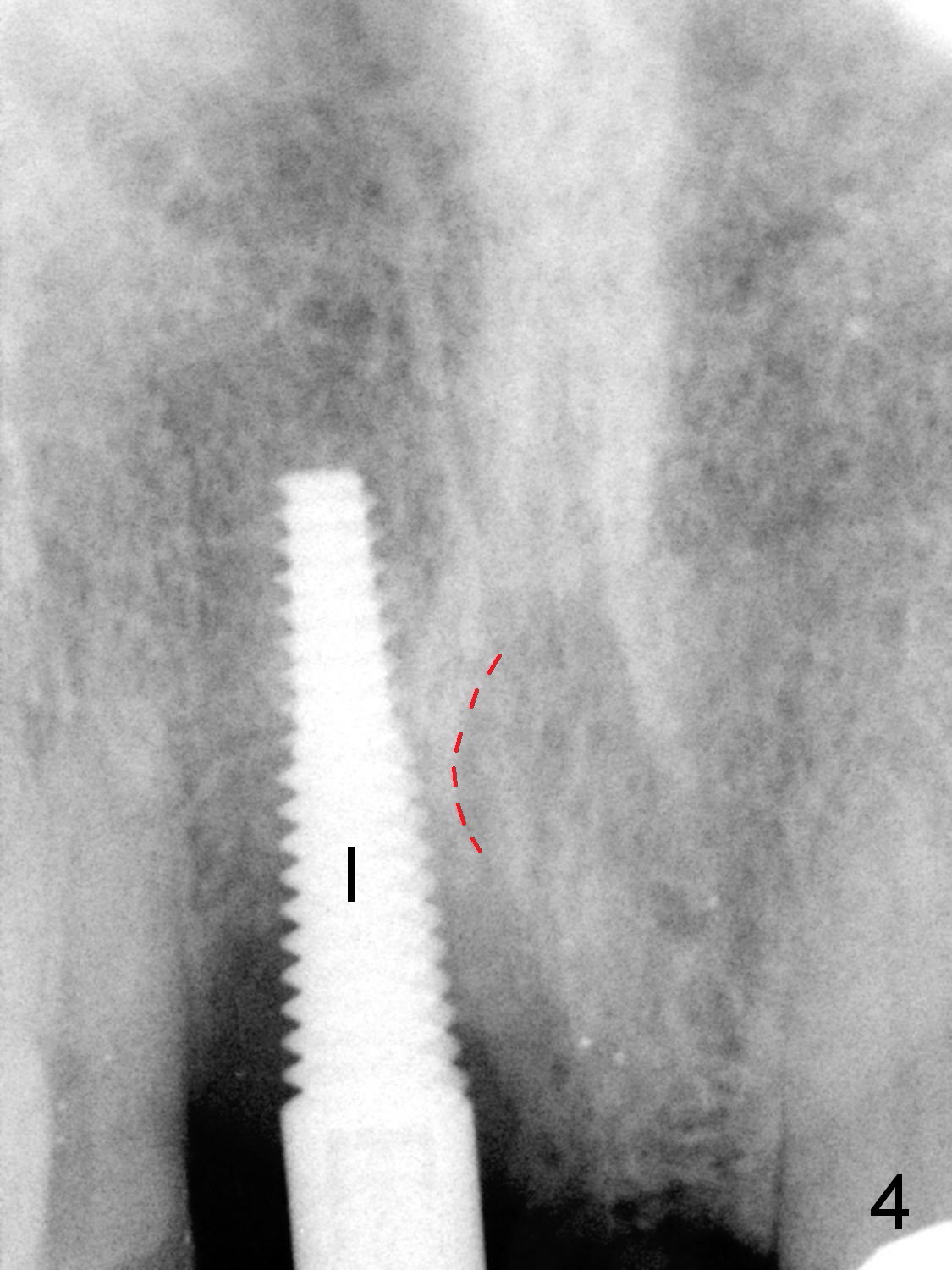
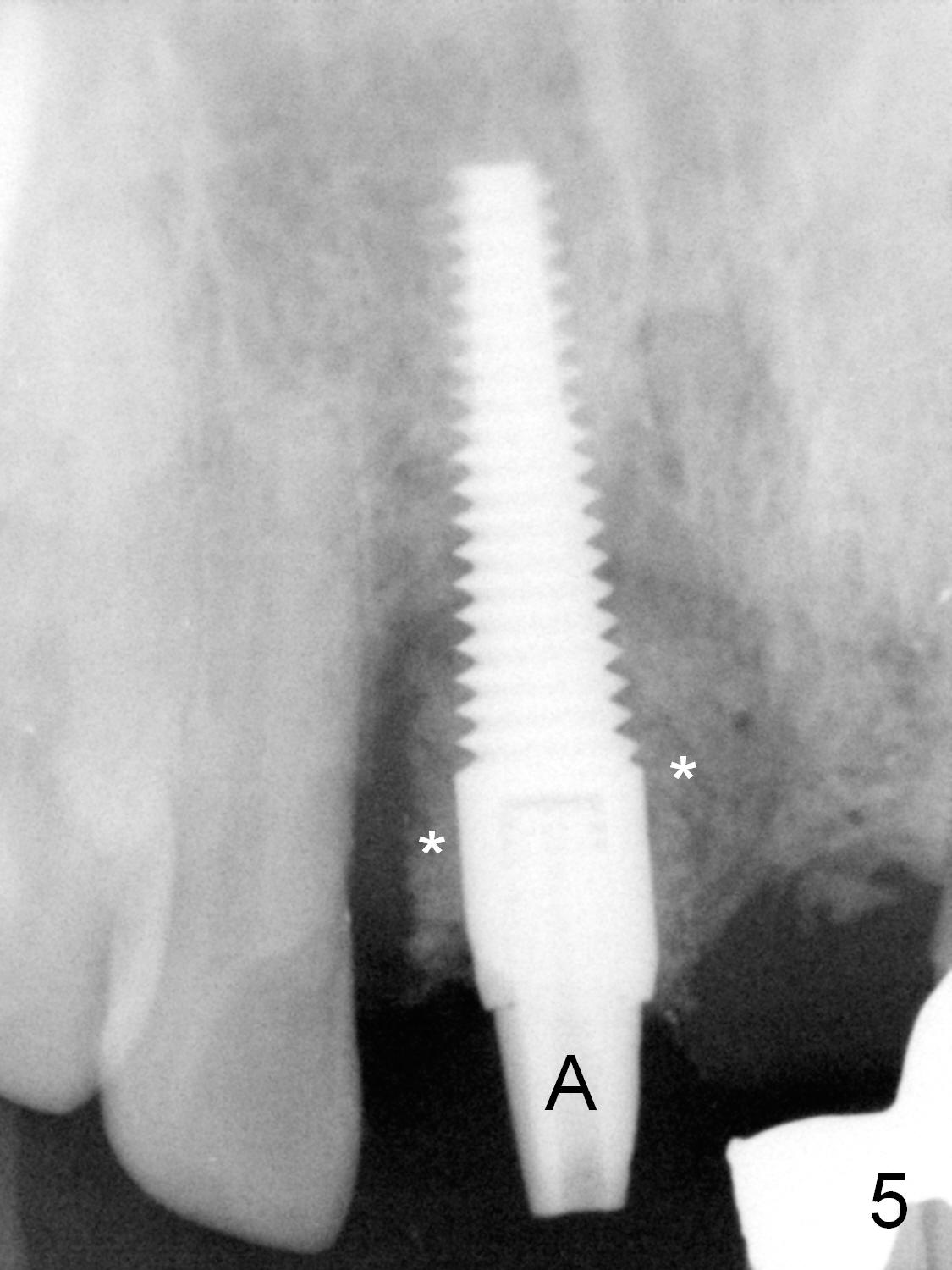
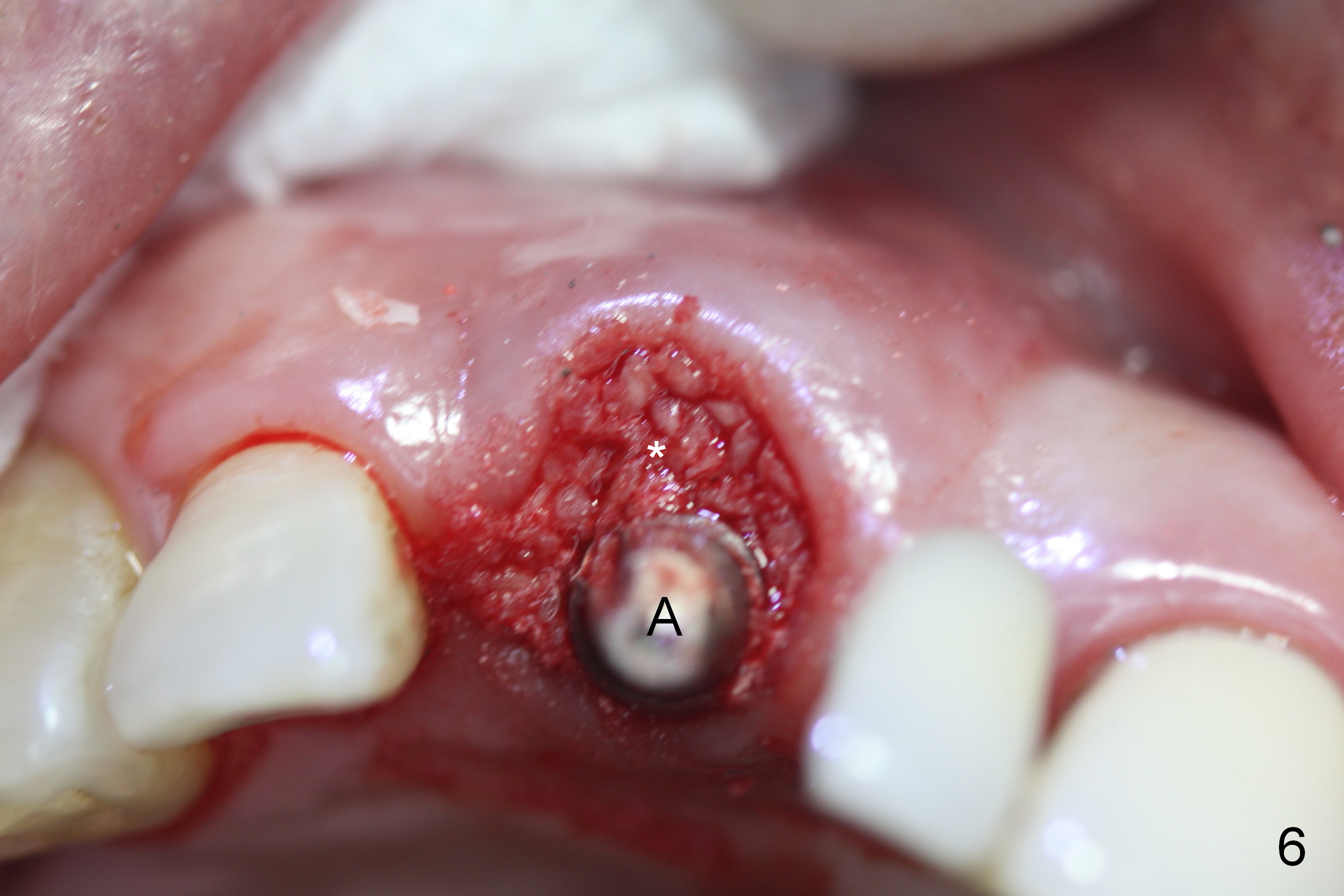
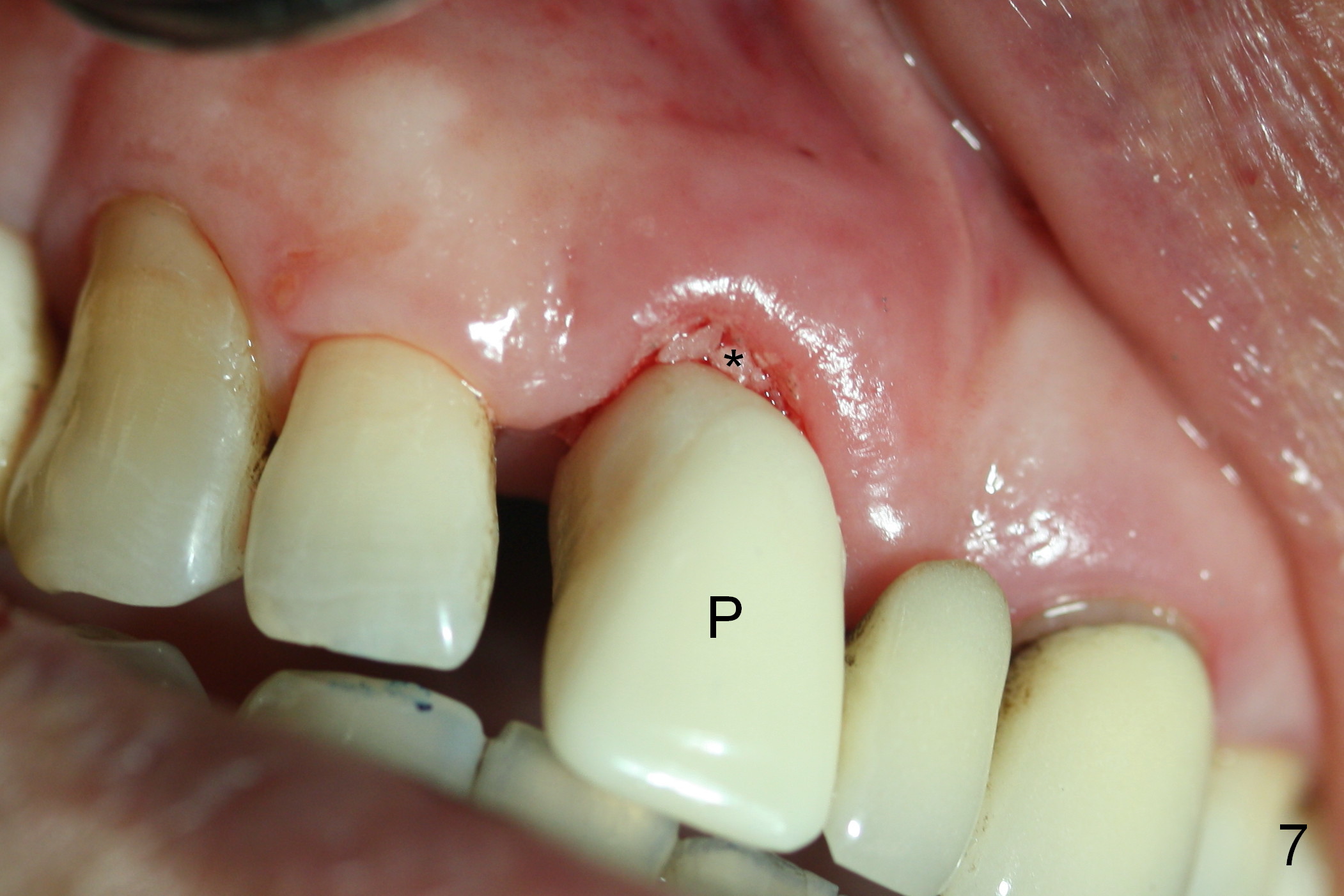
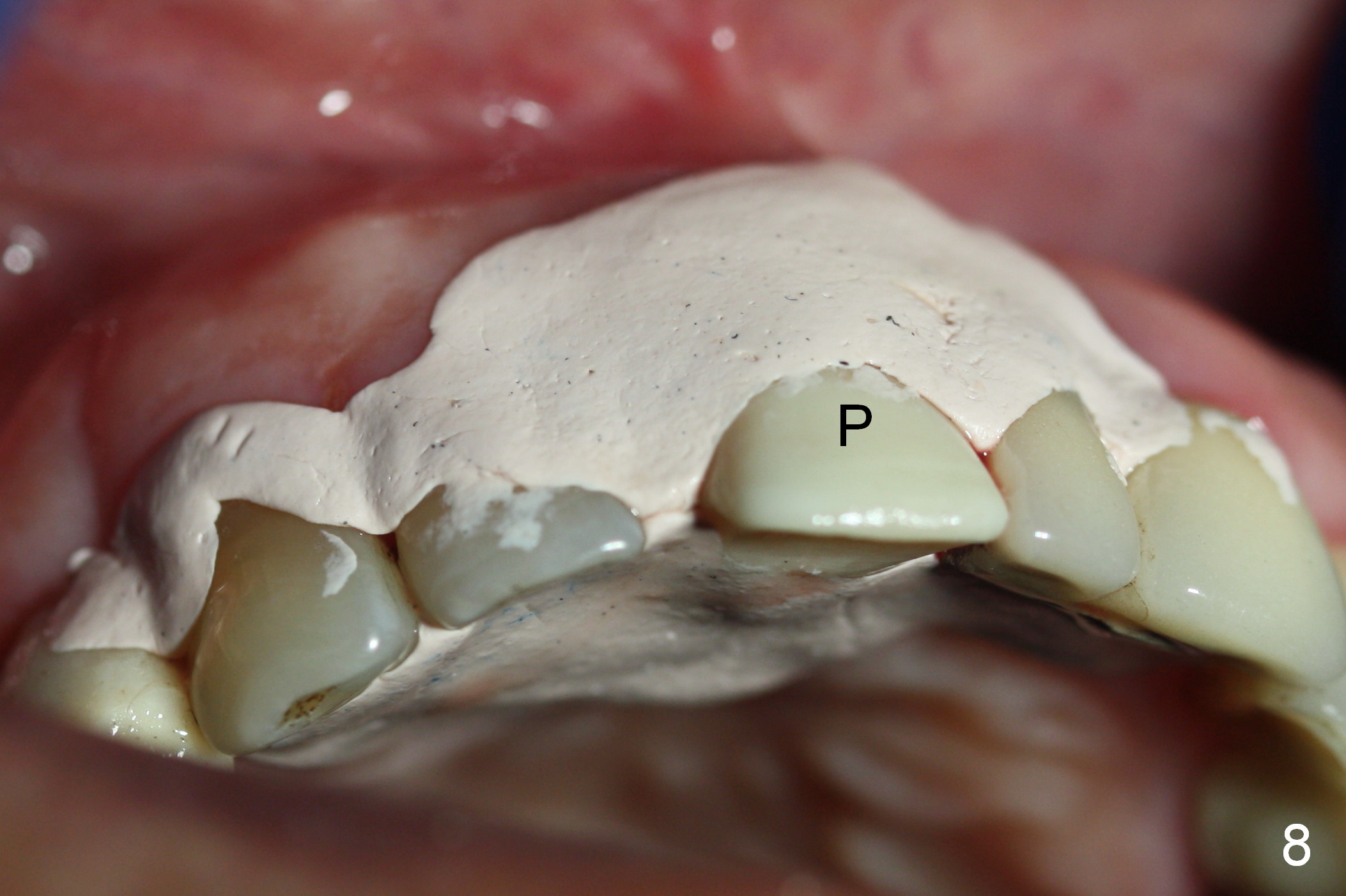
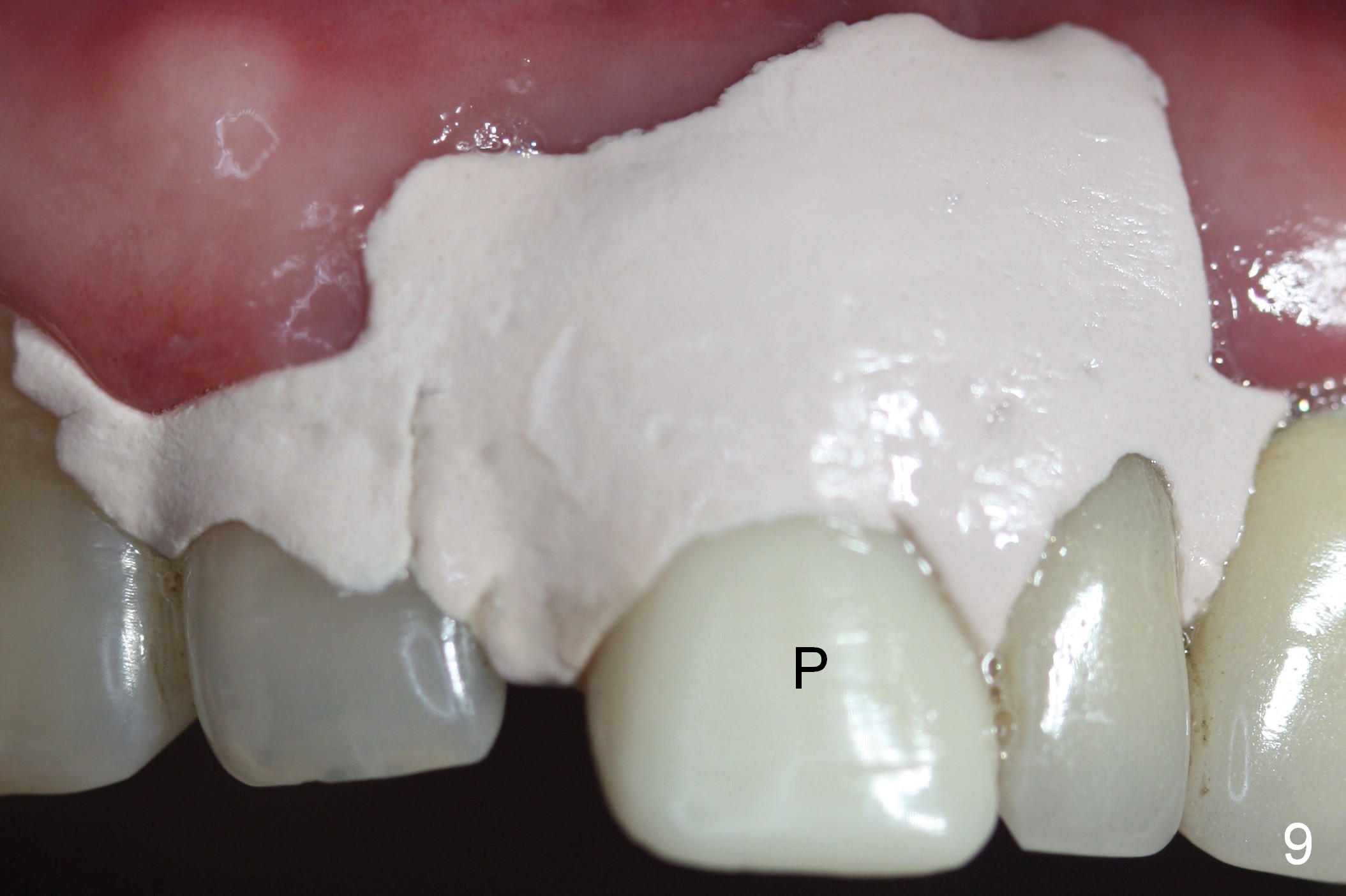
When the tooth #8 is extracted, two types of pathology are noted: fistula (Fig.1) and loss of the buccal plate (Fig.2). After thorough socket debridement and Clindamycin soaking, a 2 mm pilot drill, which is used to initiate osteotomy in the palatal wall for 20 mm, has distance from the Incisive Canal (Fig.3 red dashed line). Then the initial osteotomy is moved more palatal by using a Lindamann bur, followed by 2.5 mm reamer at 17 mm (leaning as palatal as possible; underprep). For the same manner (preventing buccally drifting), 4.5x20 mm tap and implant (Fig.4 I, >56 Ncm)) are placed. After inserting a 3.5x5 mm abutment (Fig.5,6 A) and fabricating an immediate provisional, two pieces of Osteotape is placed against the buccal gingiva (inside the socket), followed by placement of allograft and Osteogen in the remaining socket (Fig.5,6 *). When the immediate provisional is cemented securely (Fig.7 P), the bone graft (*) is not completely covered. Perio dressing (Fig.8) is applied for complete bone graft coverage and patient comfort (physically and psychologically). Before this procedure, the patient has made an appointment for an immediate implant at #30.
The perio dressing remains in place around the immediate provisional (Fig.9 P) 2 weeks postop. For cosmetic reason, the dressing is removed with difficulty; the bone graft (Fig.10,11 *) appears adherent. The perio dressing appears to have been removed prematurely.
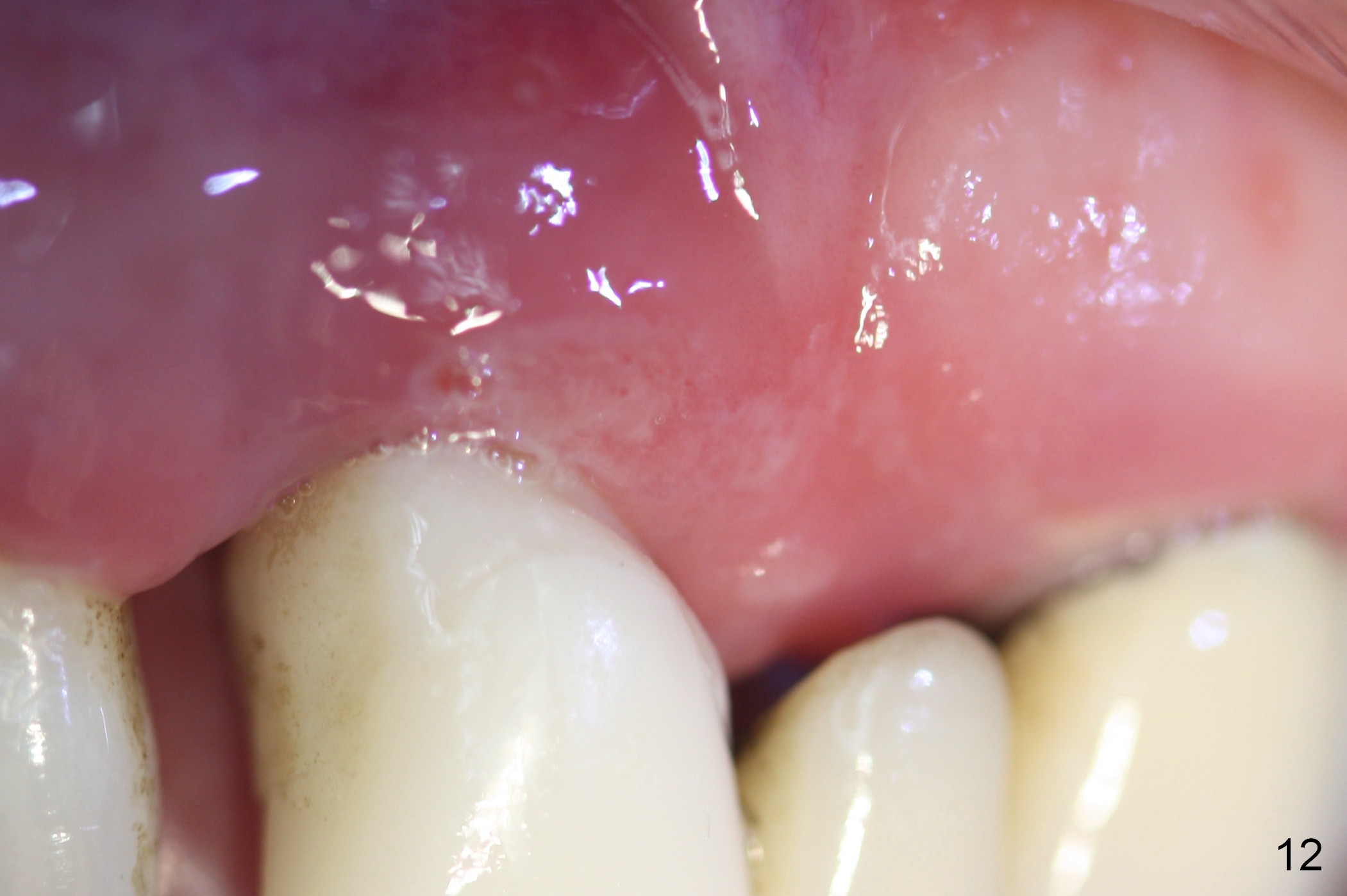
The patient returns 4 weeks postop. The margin of the provisional is higher than that of the other central incisor (Fig.12). The provisional is removed (Fig.13) for revision (Fig.14,15). It is expected that the gingiva will grow downward.
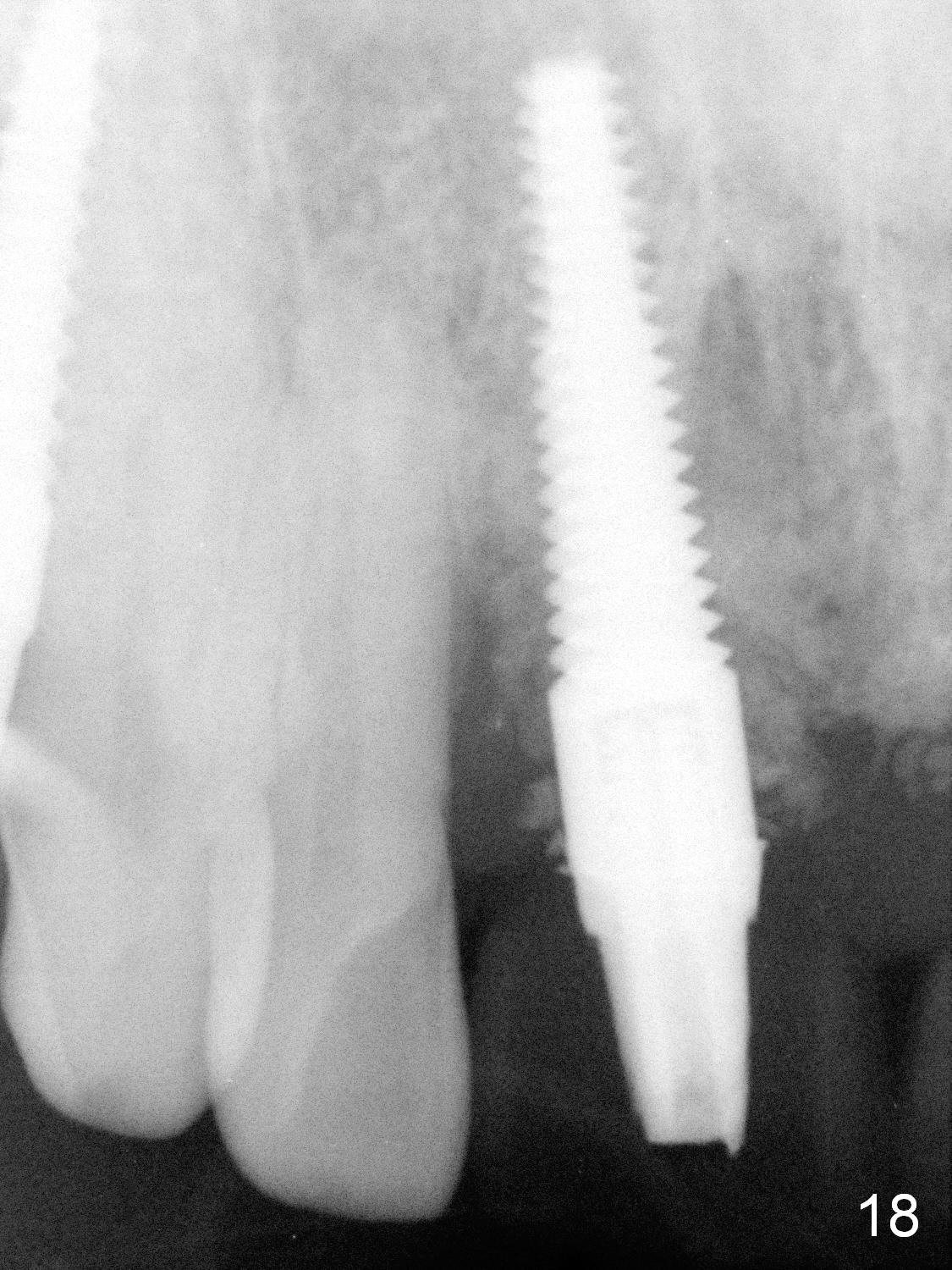
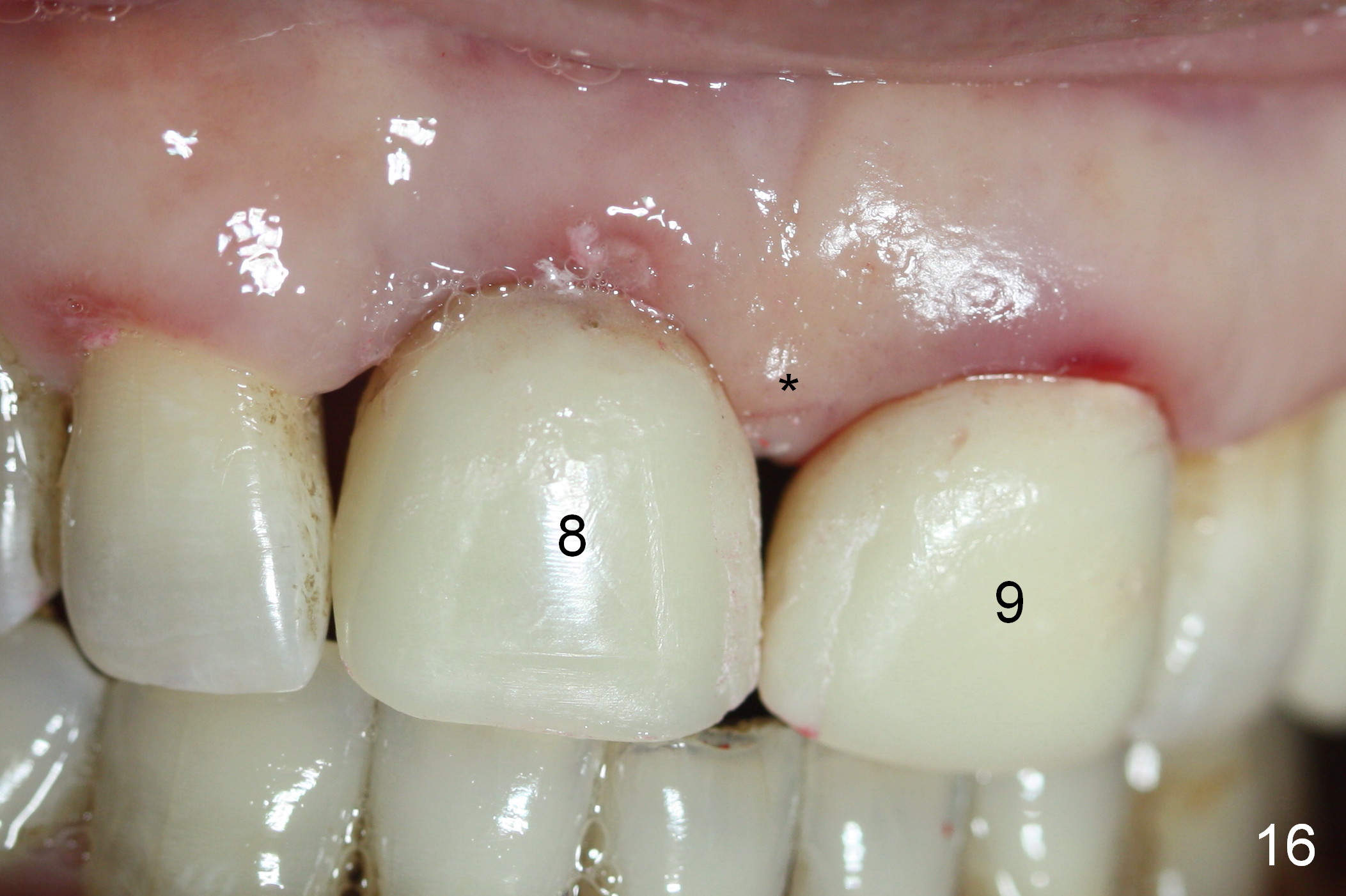
One month 20 days postop, the pontic and the retainer at #9 are removed. Two provisionals are fabricated at the central incisors (Fig.16: #8,9) to squeeze the papilla between them (* (as planned), as compared to Fig.15). Eighteen days later, the papilla elongates (Fig.17 arrow). PA taken 2 months postop shows retention of majority of bone graft around the implant (Fig.18).
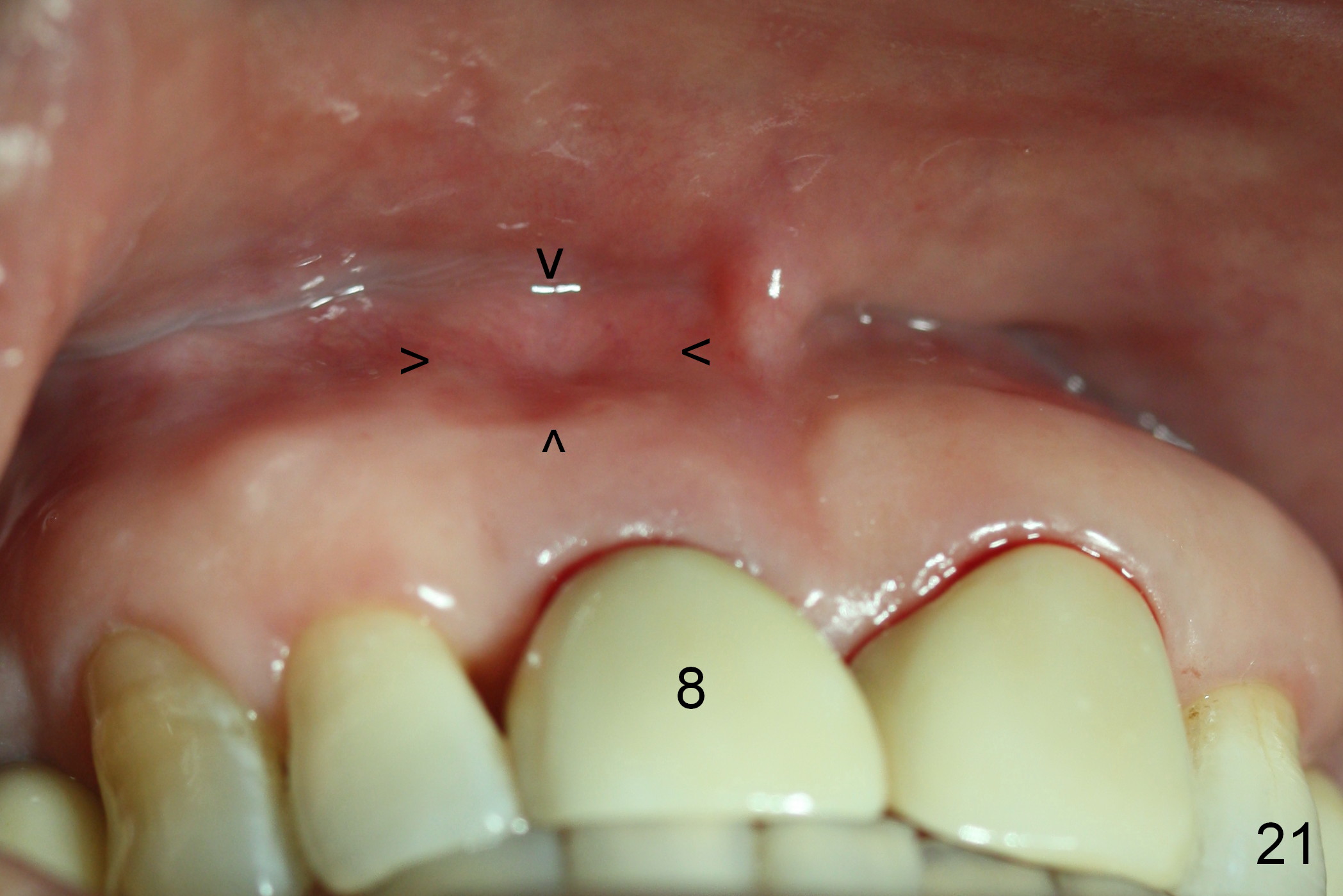
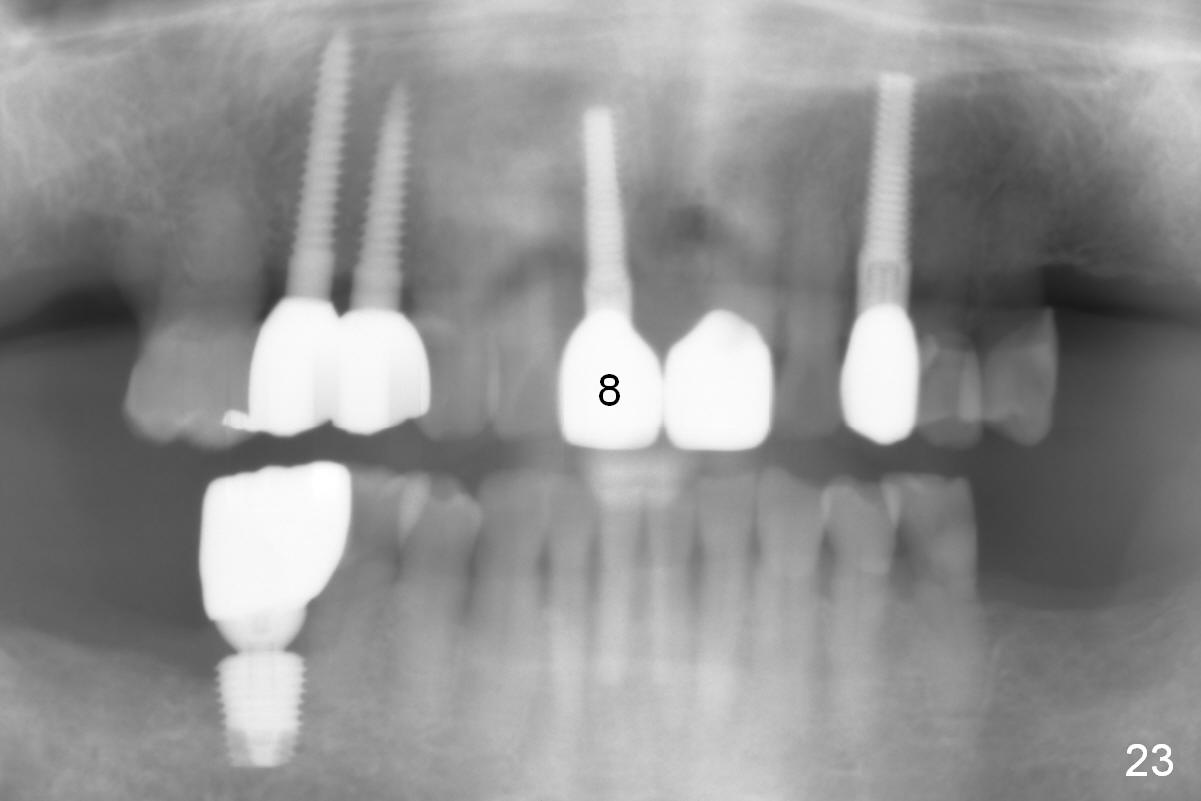
After interaction with lab (1,2), crowns are cemented 4 months postop at #8,9 with small black triangles distally (Fig.19,20). Although the gingival margin is symmetrical, there is a concavity apical to #8 (Fig.21 arrowheads). The patient is satisfied with the appearance of the crowns 1 month post cementation (Fig.22). There is no bony defect 8 months post cementation (Fig.23).
Return to Upper Incisor Immediate Implant,
Metronidazole Study
Xin Wei, DDS, PhD, MS 1st edition 08/11/2015, last revision 05/27/2018