
|
|
|
|
Visibility & Precise Entry
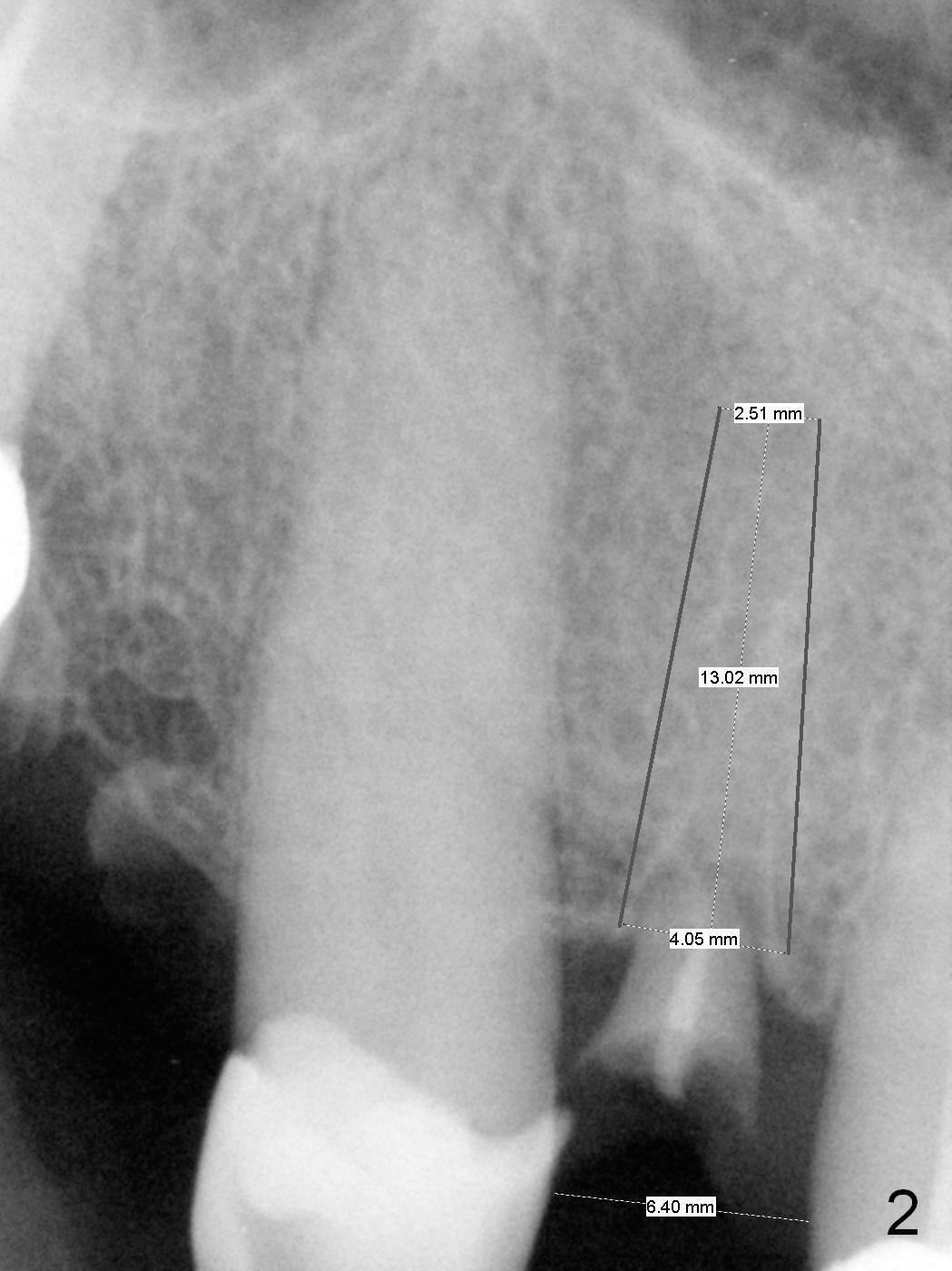
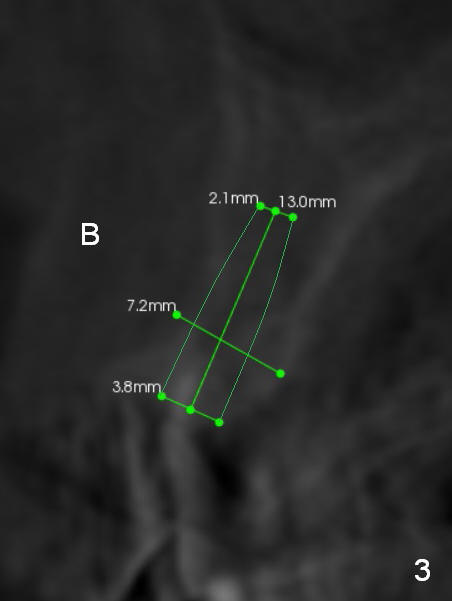
A 59-year-old man (used to be coke drinker) has several missing teeth and residual roots. He wants to get rid of a loose flipper for #7, which is incisally (Fig.1 arrow) and labially (take preop photos) displaced. When it is extracted with curettage of apical granulation tissue (Clindamycin), the socket may not be completely exposed, especially palatally. Do not hesitate to make incision for better visibility and precise osteotomy. If the mesiodistal width of the edentulous space is more than 6.4 mm (Fig.2), use 1.6 mm pilot drill. Otherwise consider 1-piece implant. Pay attention to bone density while drilling. The initial depth will be 10 or 11 mm. PA is to be taken for trajectory and depth confirmation. To prevent periimplantitis, make sure that the first coronal thread is below the labial crest. Due to several missing teeth with insufficient posterior support, the immediate provisional should have daylight clearance. CT shows that 3.8 mm wide implant is appropriate for the buccopalatal width (Fig.3). Retrospectively, the implant could be smaller or to be placed more palatal. If the bone density is low, the implant could be longer than 13 mm.
Return to Upper Incisor Immediate Implant, Prevent Anterior Periimplantitis, IBS Xin Wei, DDS, PhD, MS 1st edition 09/26/2016, last revision 01/01/2019