,%20Vanilla,%203.8x10,%204.5x4(2).jpg)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
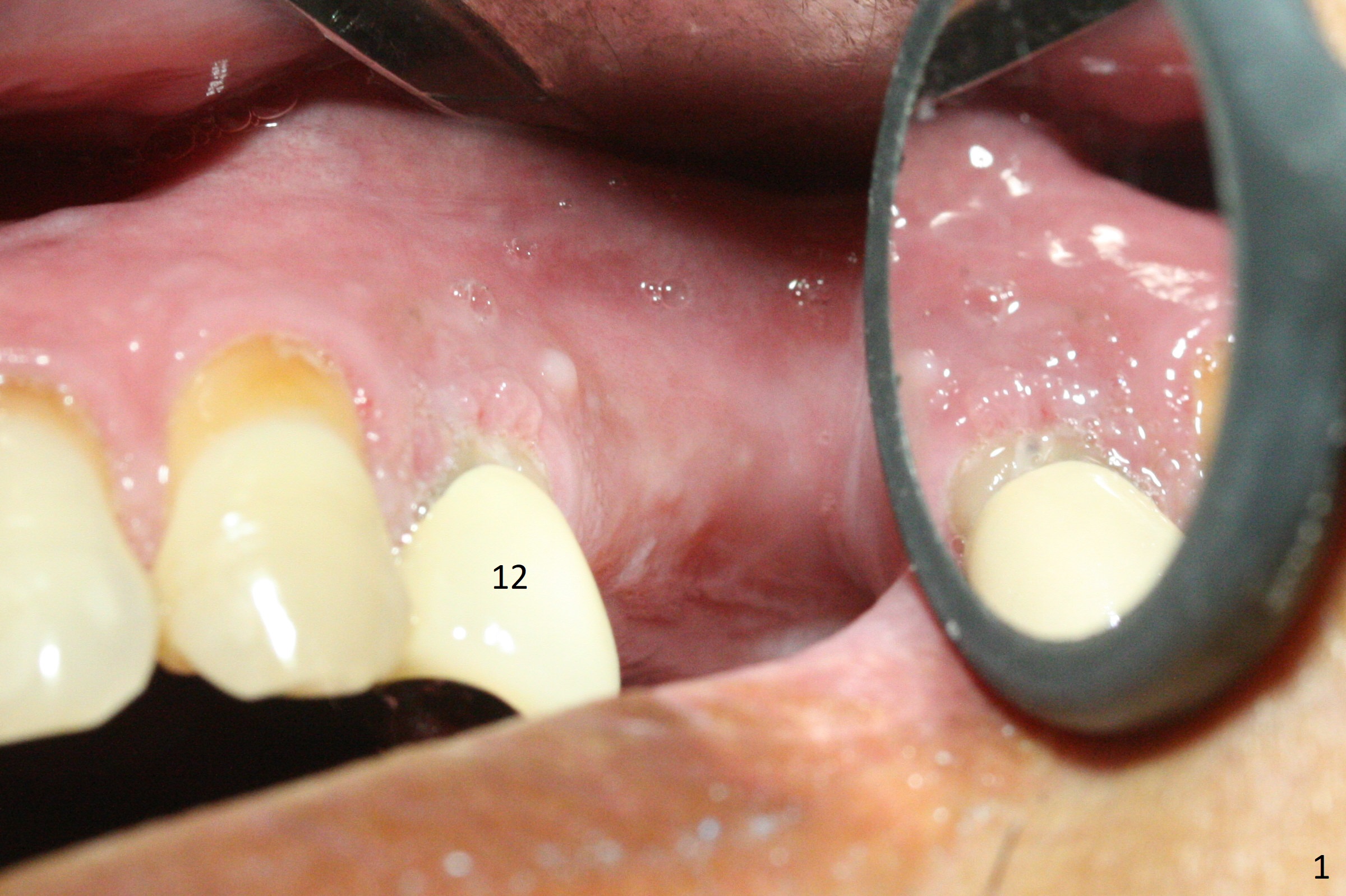
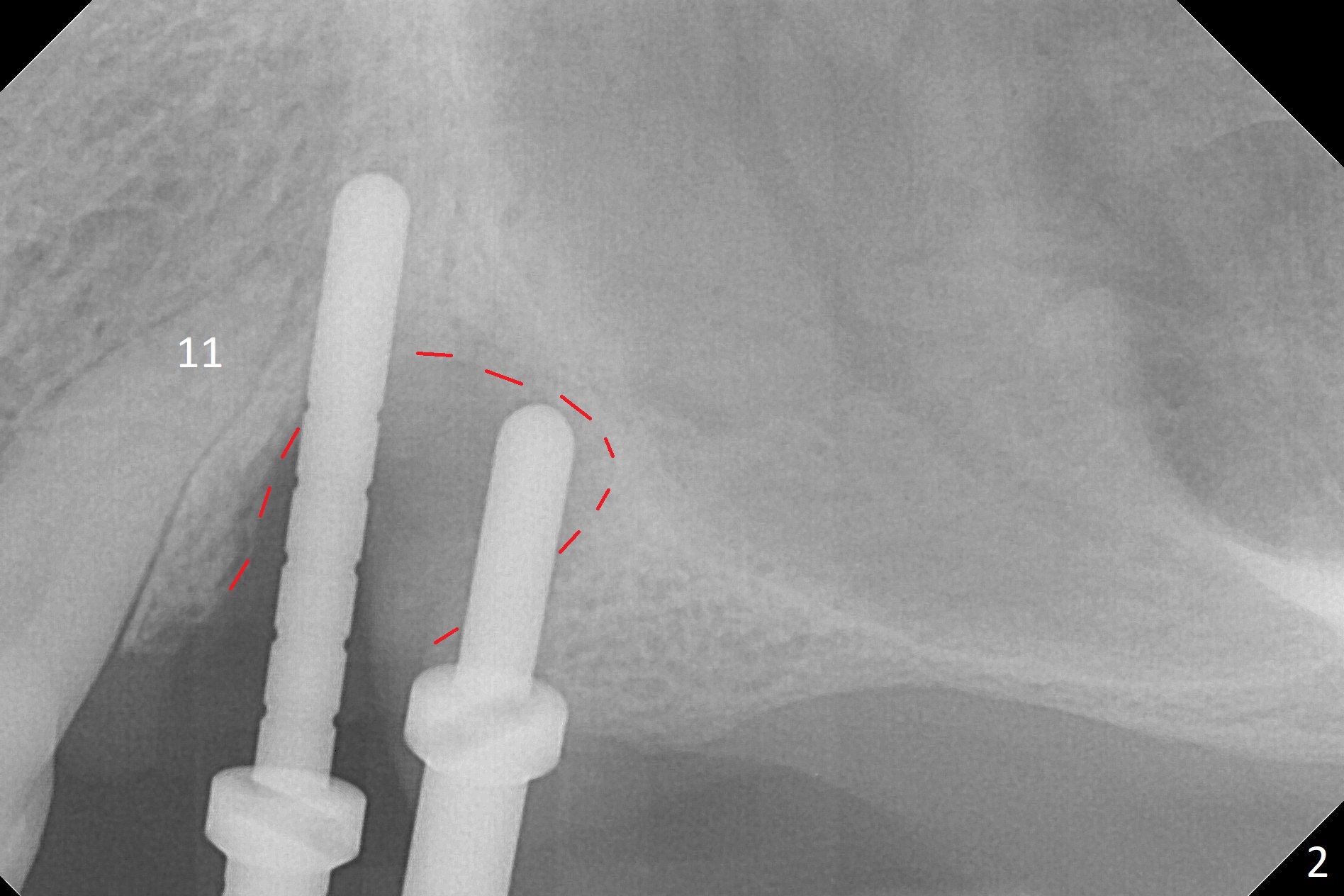
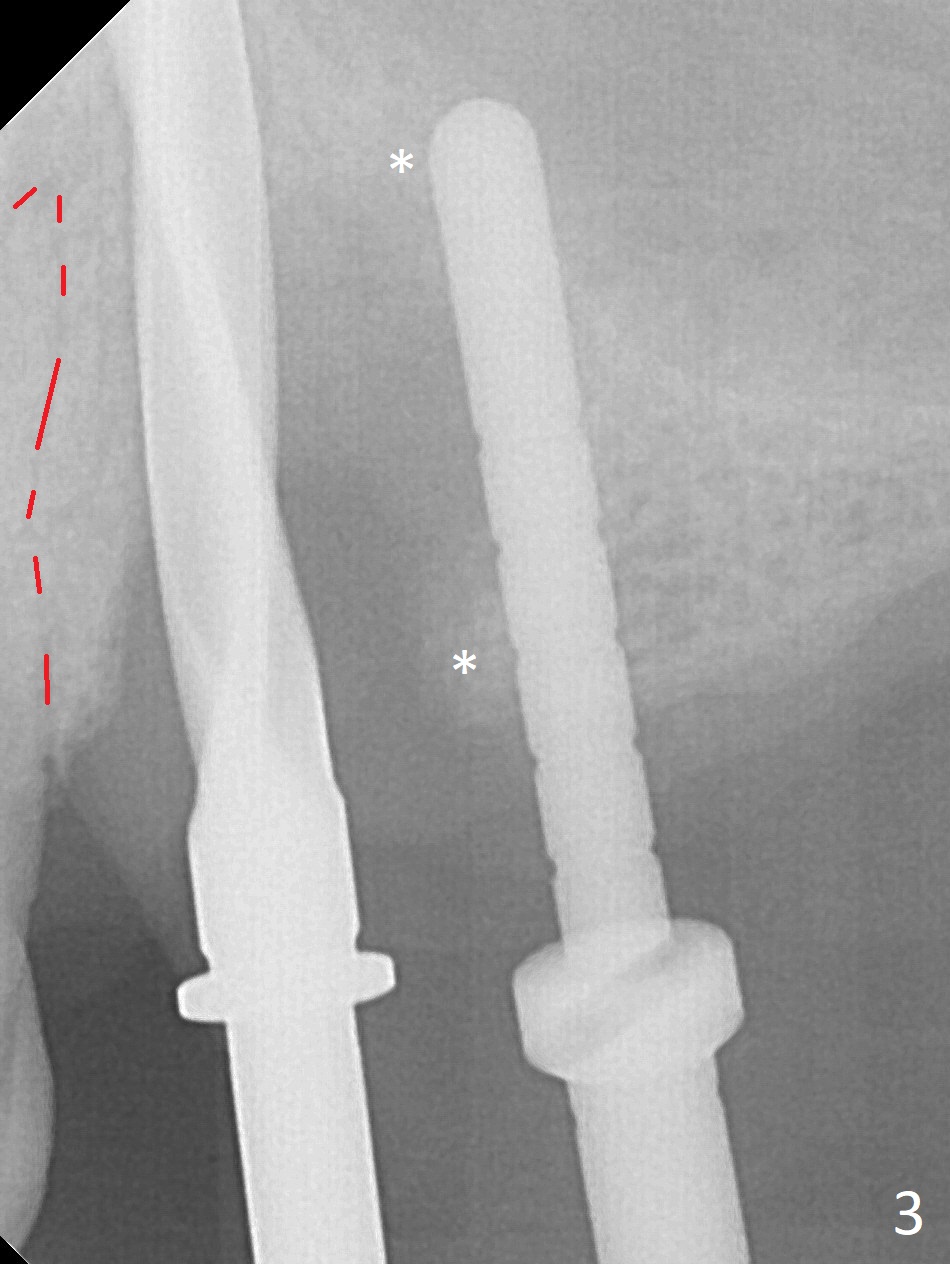
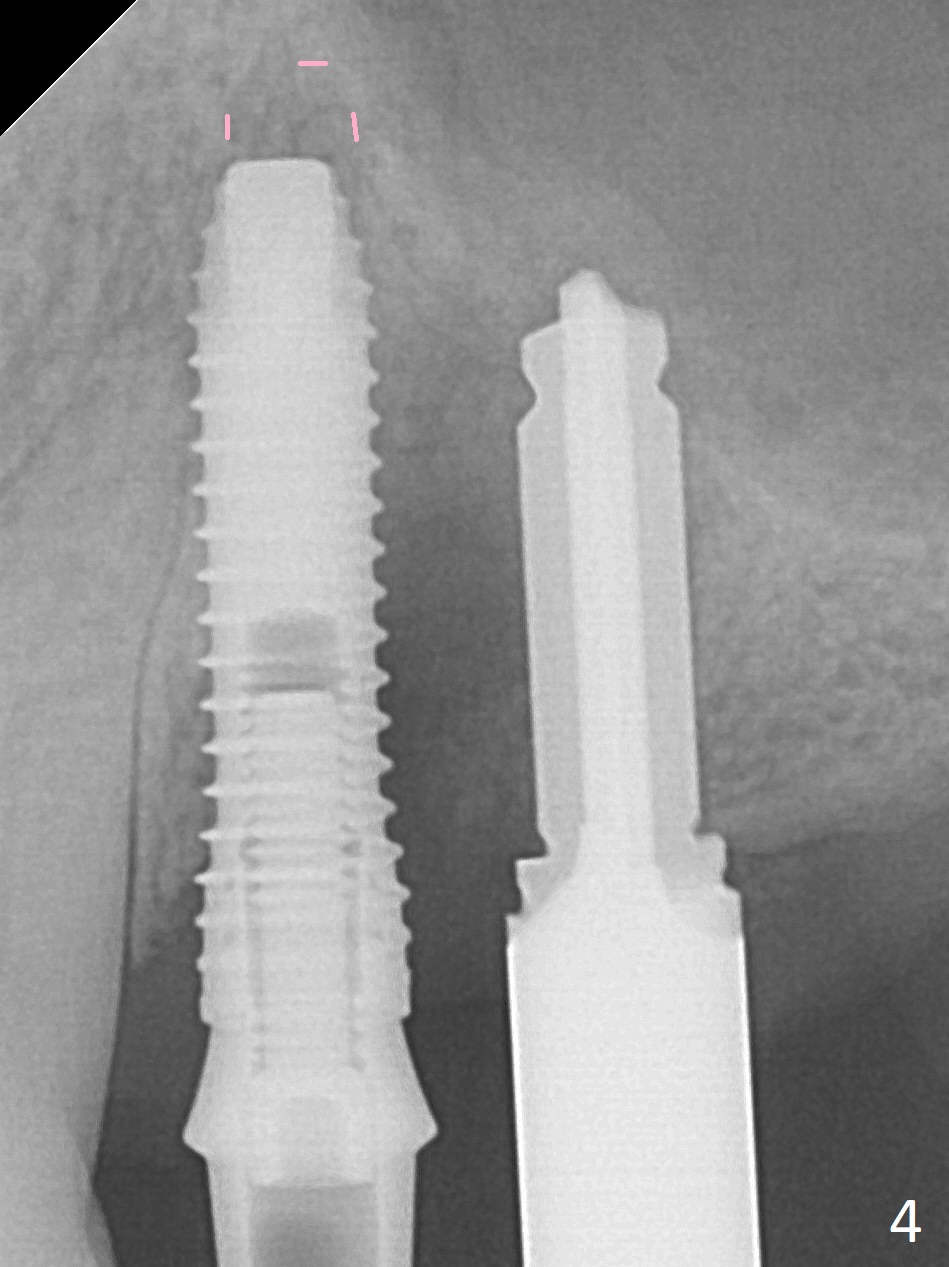
Extensive Defect
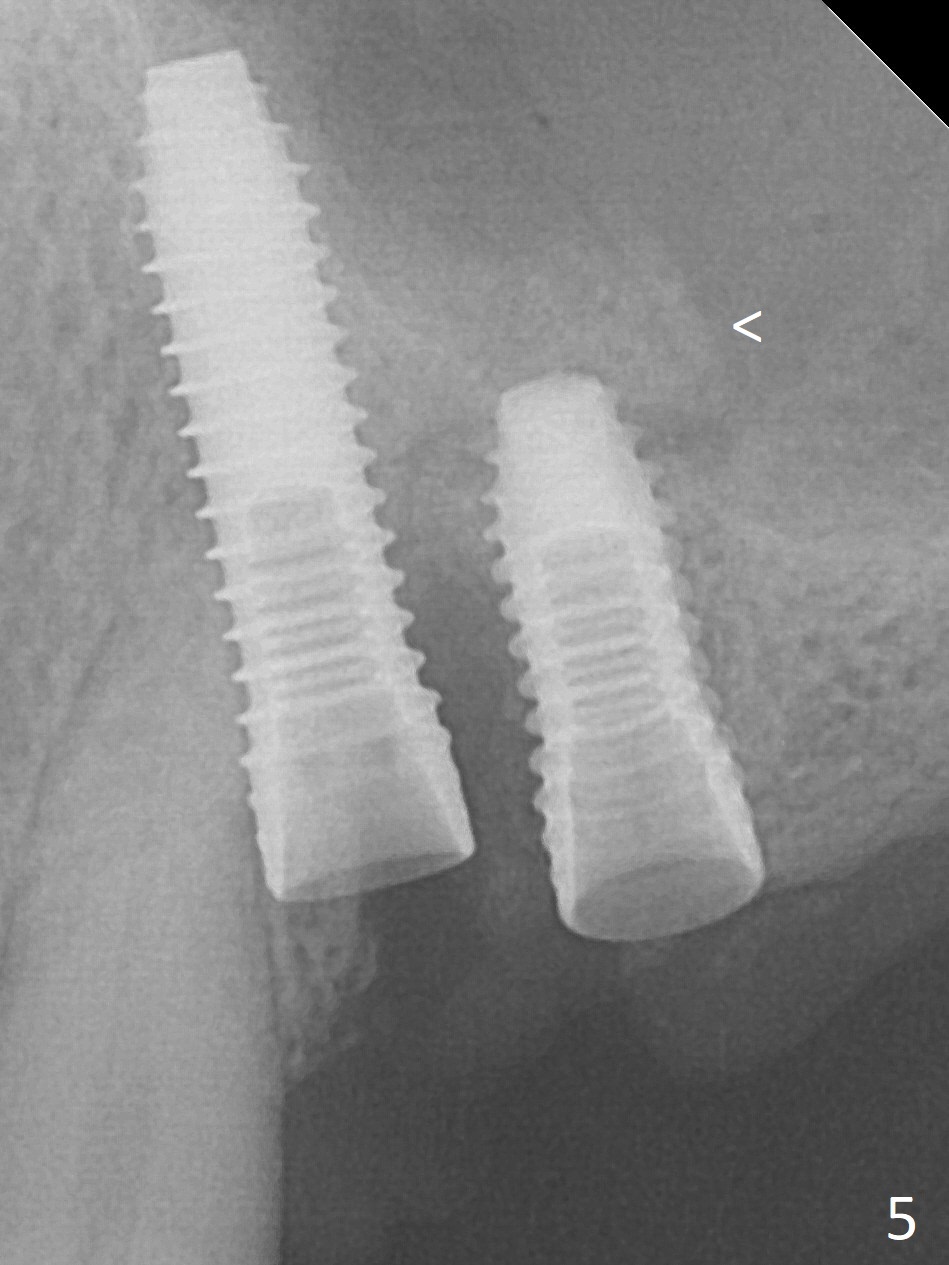
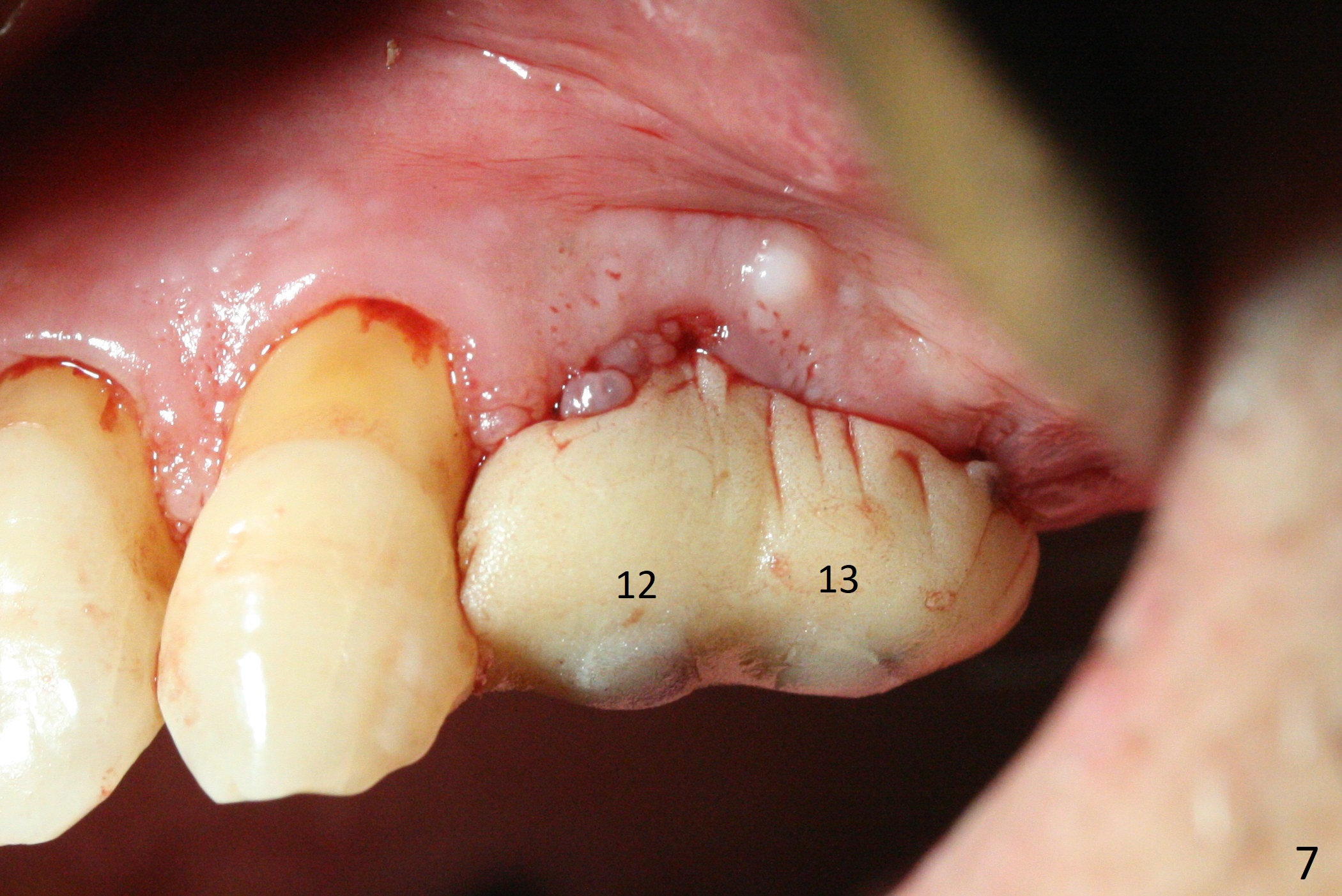
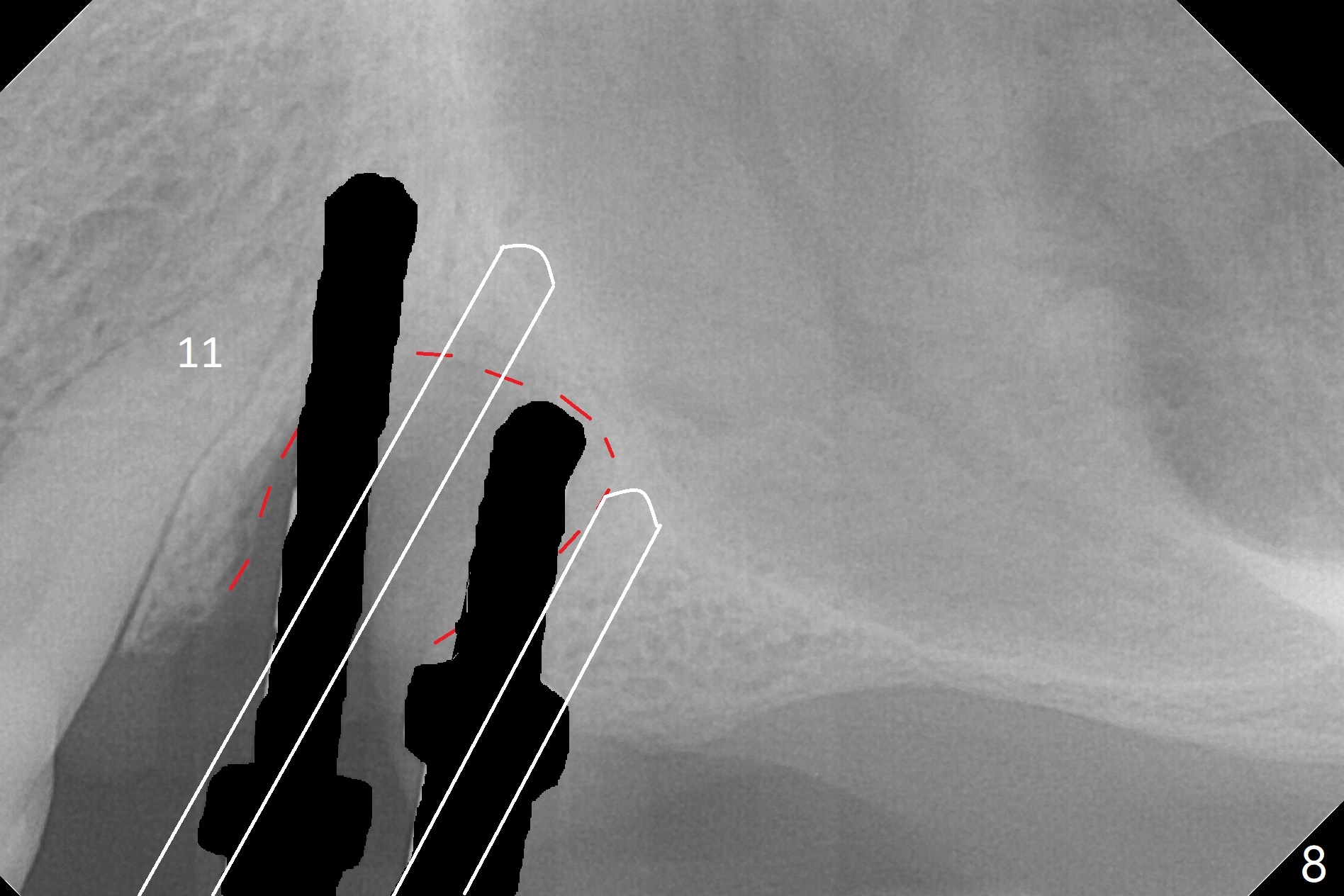
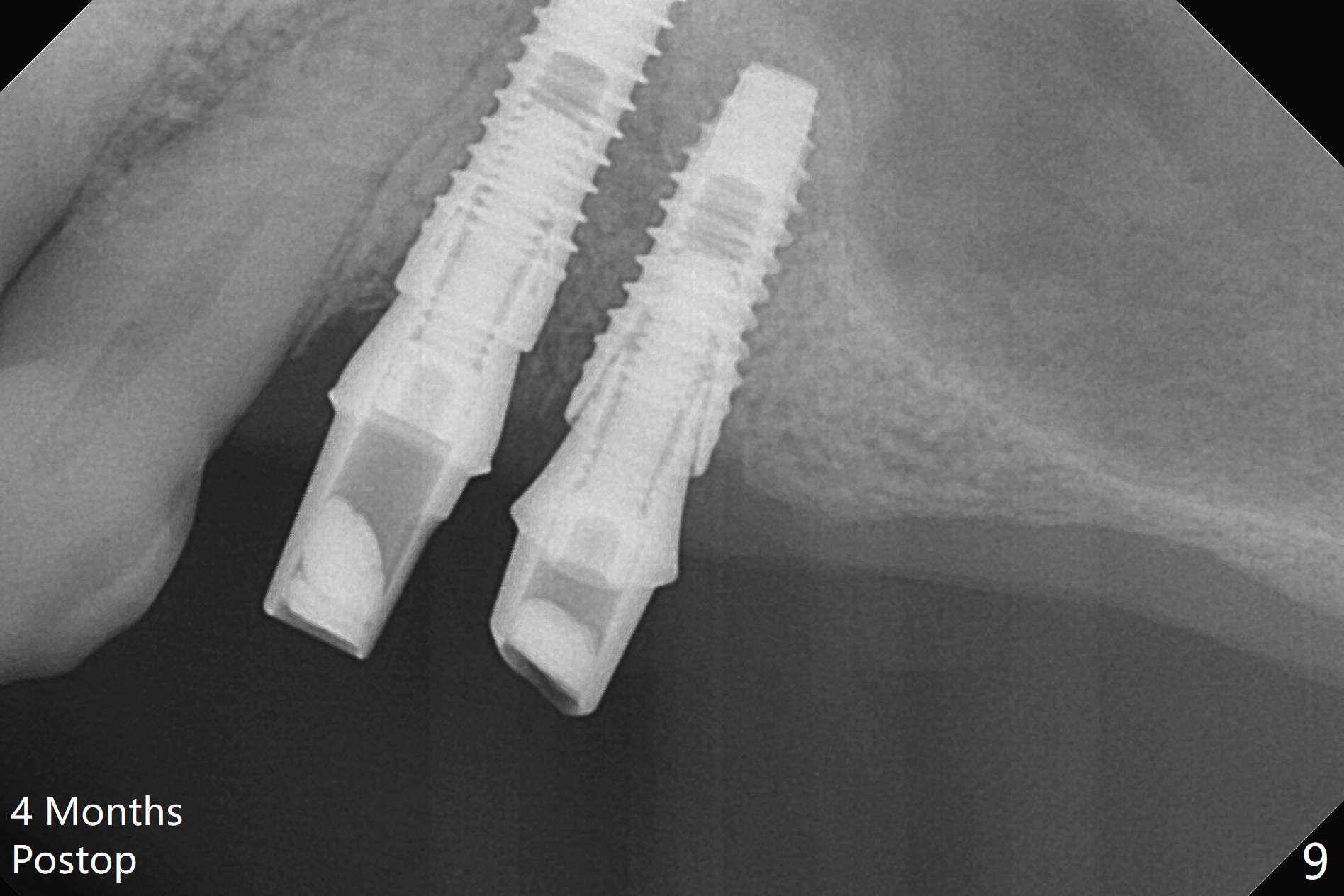
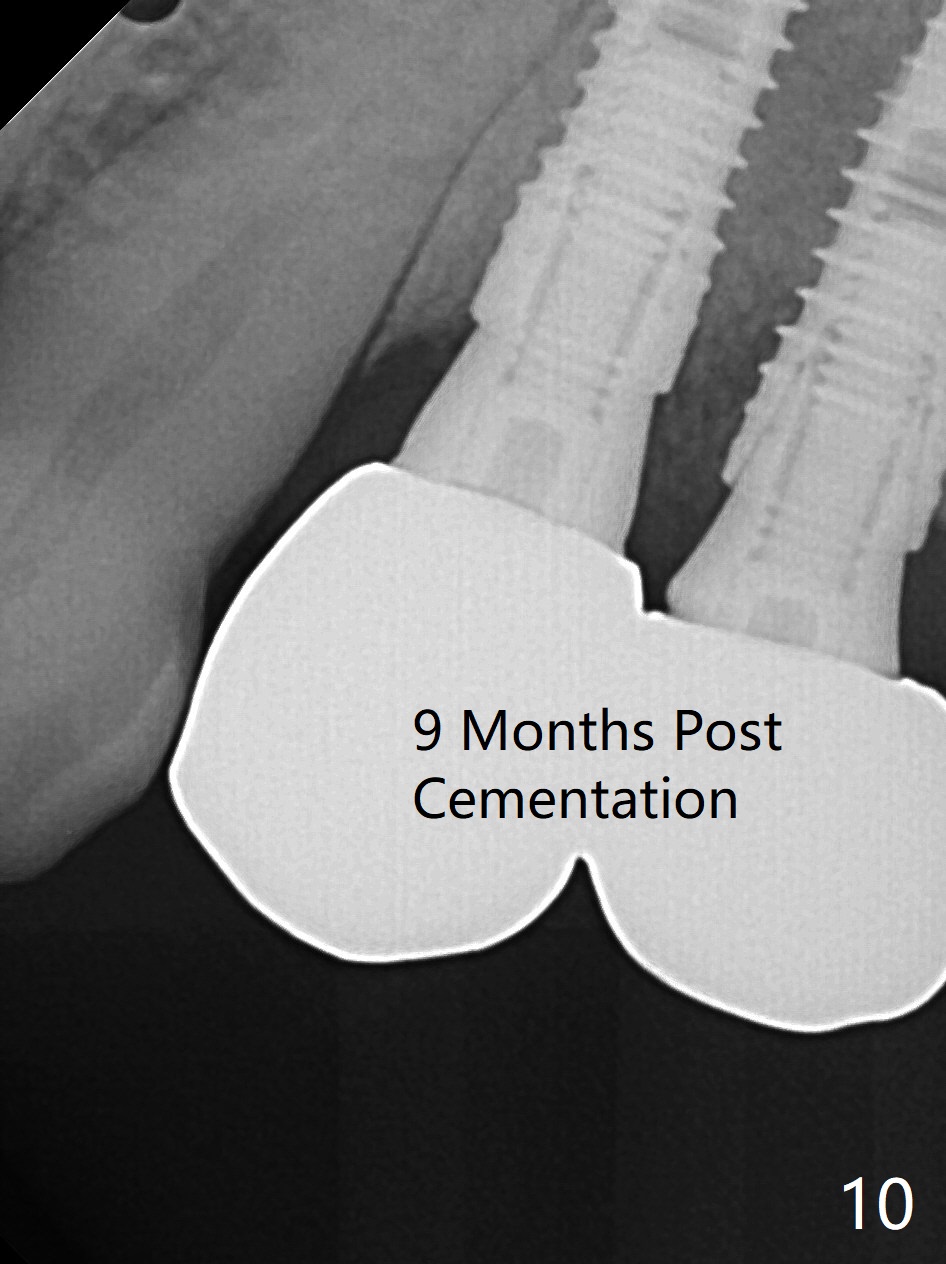
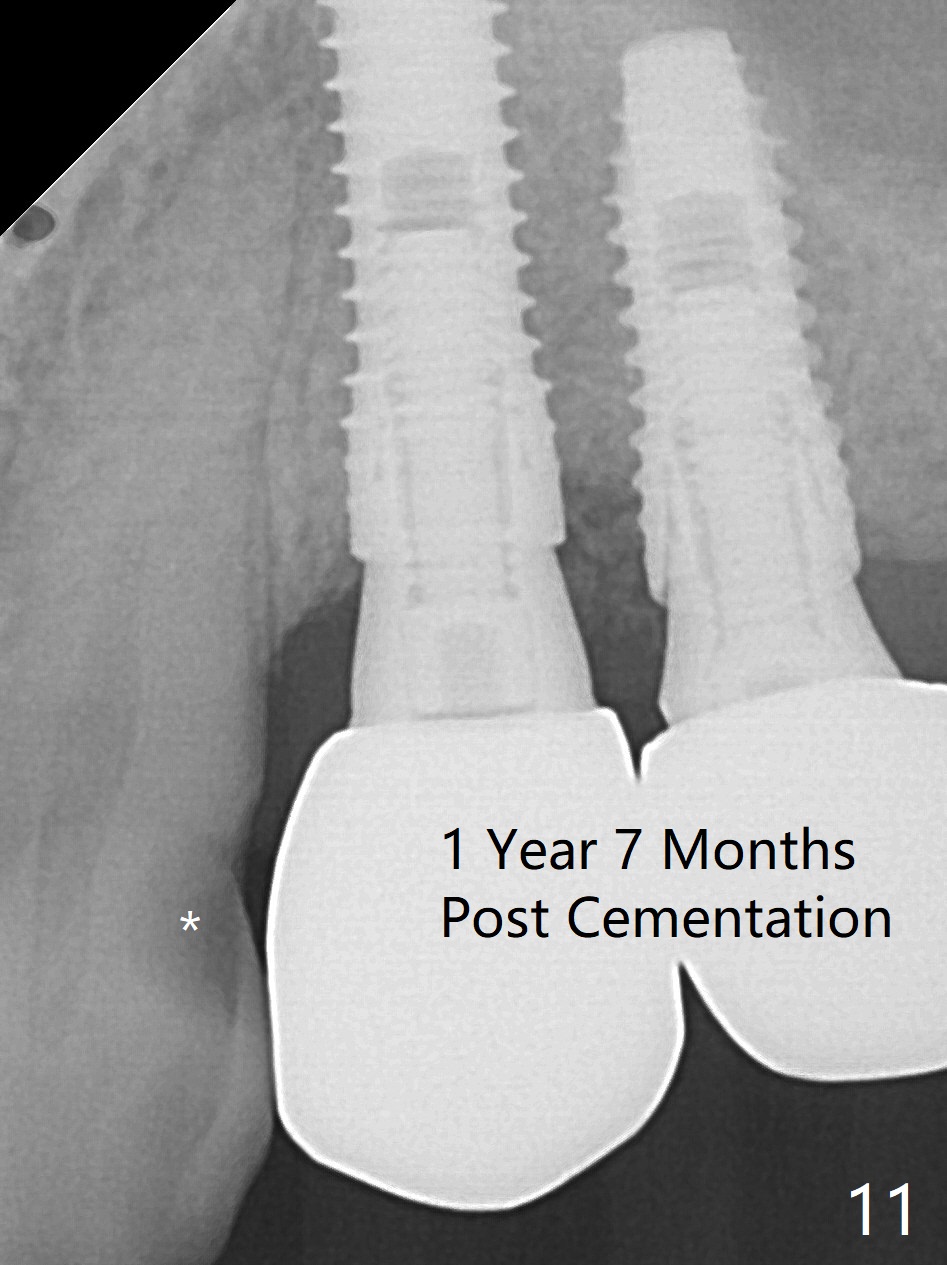
The buccal gingiva at #12 with vertical root fracture looks unhealthy (Fig.1). Osteotomy at #13 is initiated prior to #12 extraction. In fact the osteotomy happens in the extensive defect associated with #12 (Fig.2 red dashed line). To obtain primary stability, the osteotomy at #12 needs to be long, while that at #13 needs two-pointed fixation (Fig.3 *). After adjustment of trajectory at #12 and increase in diameter of the osteotomy at #13 (Fig.4), a 3.8x15 and 3.8x10 mm implants are placed (Fig.5). Following adjustment of implant depth (Fig.6), the implant at #12 becomes loose, while that at #13 tightens. With placement of abutments, an immediate splinted provisional is locked in place to stabilize the loose implant at #12 (Fig.7). The patient complains of cold sensitivity in the upper left quadrant, possibly related to the fact that the implant at #12 is close to the apex of the tooth #11. The position and trajectory of the initial osteotomies should be changed as shown in Fig.8 (white lines, as compared to Fig.2). There is no sensitivity 1 month postop. Impression is taken 4 months postop (Fig.9) after #13 mesiobuccal margin prep. The implants were placed too close to each other. The abutment screw at #13 is retightened 8 months post cementation. There appears no bone loss 9 months post cementation (Fig.10), while the tooth #11 has periapical infection with DL caries 1 year 7 months post cementation (Fig.11).
Return to Upper Premolar Immediate Implant, Armaments 30/31 Xin Wei, DDS, PhD, MS 1st edition 12/29/2017, last revision 11/15/2019