
.jpg)
|
|
|
|
|
|
|
|
|
|
Flapless & A Flexible System
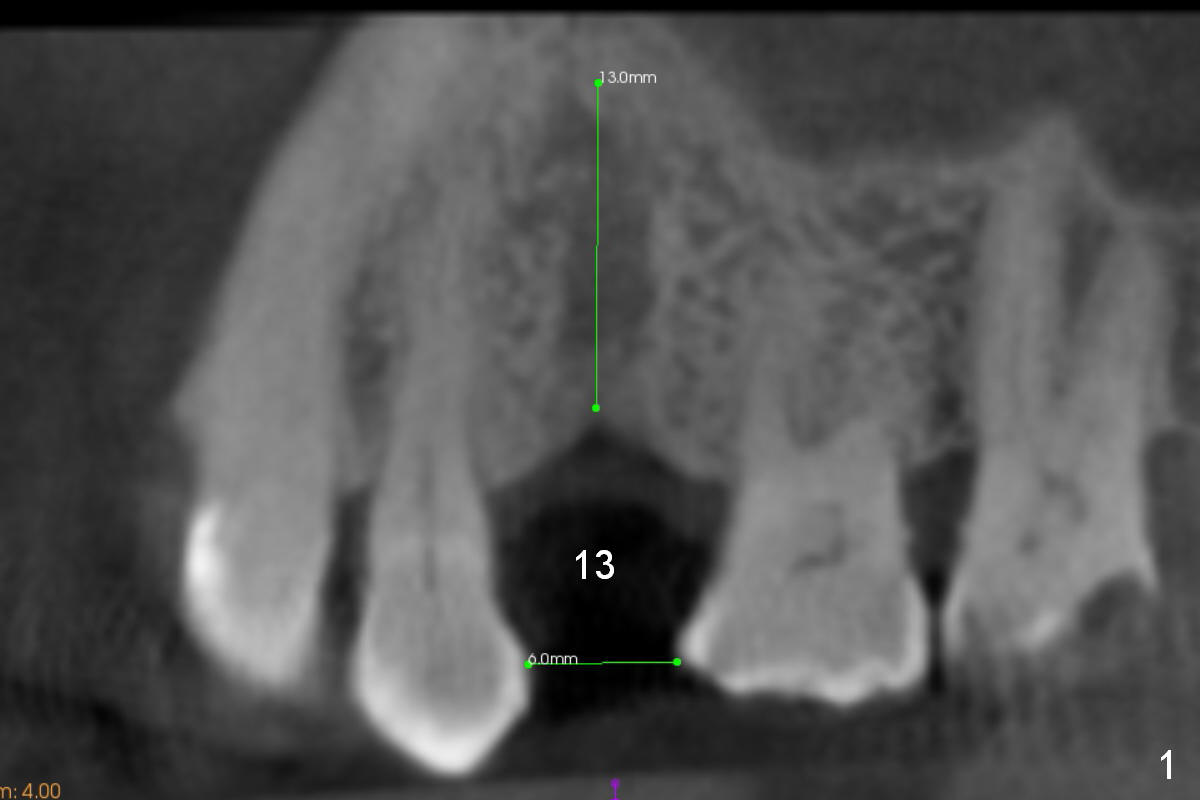
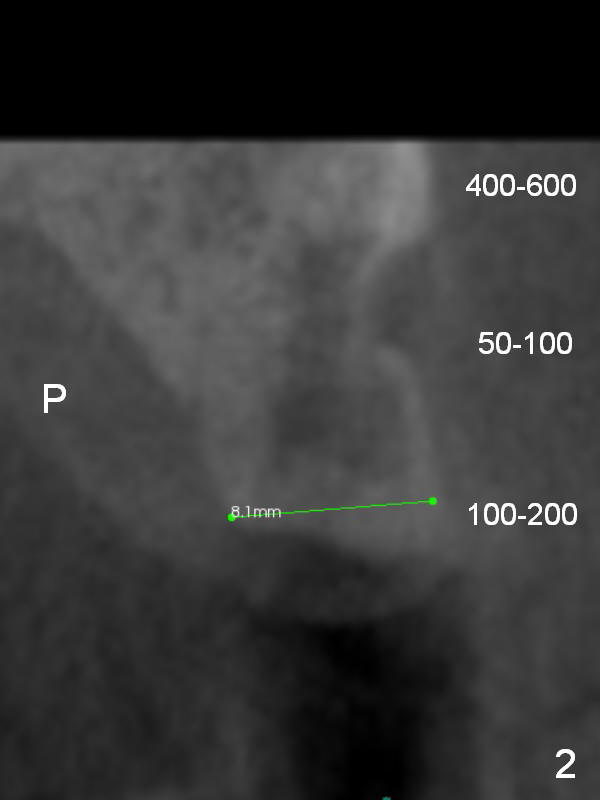
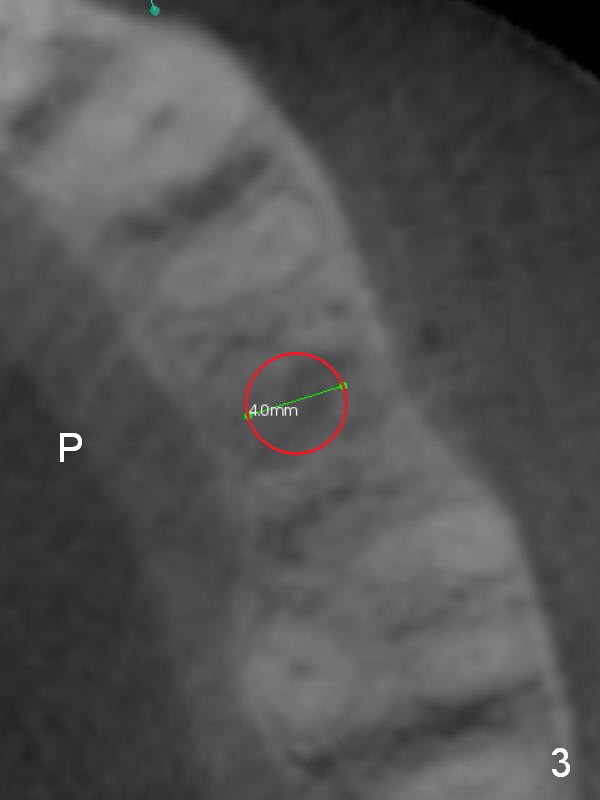
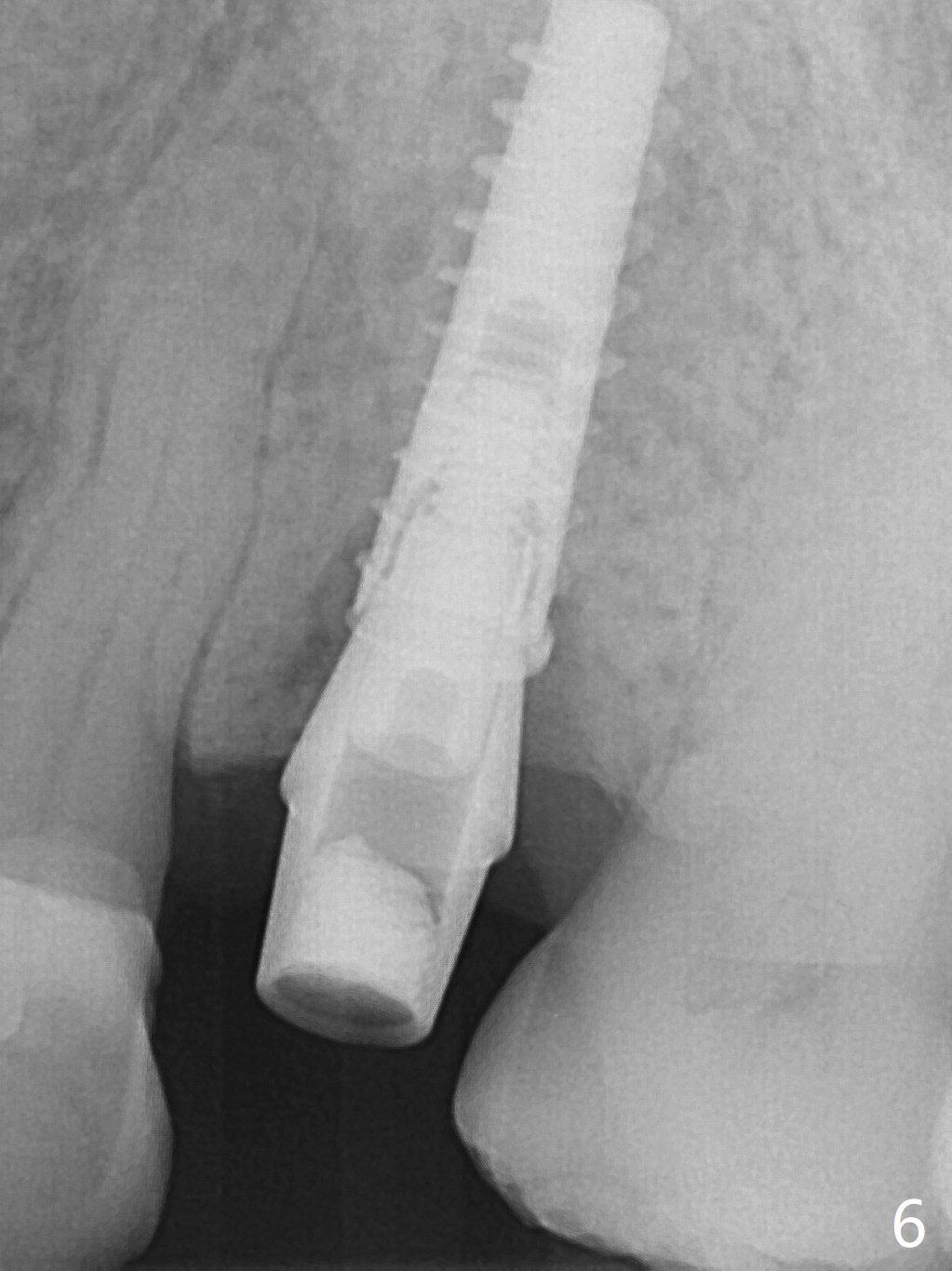
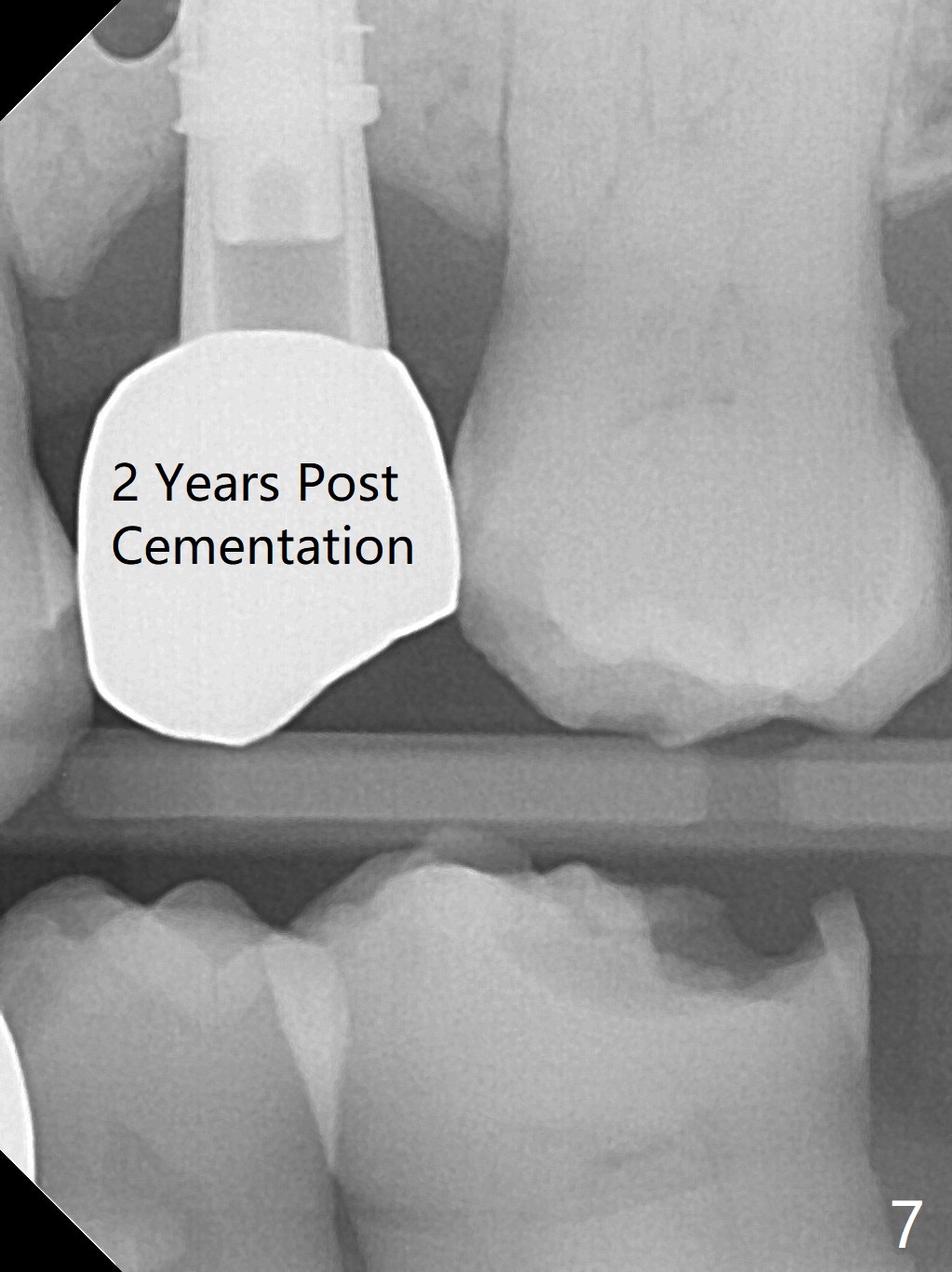
A 74-year-old man has diabetes. Implant osteointegration appears to be slow at #4, while the implant at #28 failed once. He requests implant at #13 (Fig.1). It seems that the bone is wide enough (8 mm, Fig.2 (CT coronal section) (P: palatal)) to hold a 4 mm implant (Fig.3 (axial section)). Since bone density is low at the coronal (100-200 units) and middle (50-100 units) segments (Fig.2), bone condensation will be beneficial. To facilitate wound healing, flapless approach is adopted using 1.6 mm pilot drill (Fig.4), followed by 1.4/2.6 mm bone expander. In fact there is resistance to expansion in the zone 1. Magic expander (3.0 mm) is also tried with difficulty. It appears that bone density is higher than expected. The second portion of Magic Surgical Kit is then used: 3.3 mm Magic Drill for 15 mm (gingival level, followed by Final Drill). A 4x13 mm IBS implant is seated incompletely. The osteotomy is further enlarged by 3.8 mm Magic Drill for 11 mm and deepened with 3 mm drill until 18 mm. Finally the implant is placed at a satisfactory level with insertion torque > 50 Ncm (Fig.5). A 4.5x4(3) mm abutment is placed and periodontal dressing is applied. The patient chooses to return for impression 6 months postop (Fig.6). The abutment changes to a 4x4(4) mm one. The crown is recemented nearly 2 years post cementation, which is related to distal and deep placement of the implant and bruxism (Fig.7).
Upper Premolar Immediate Implant 21 Xin Wei, DDS, PhD, MS 1st edition 02/18/2017, last revision 09/05/2019