
.jpg)

|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
||
|
|
|
|
|
||
As Long As Possible
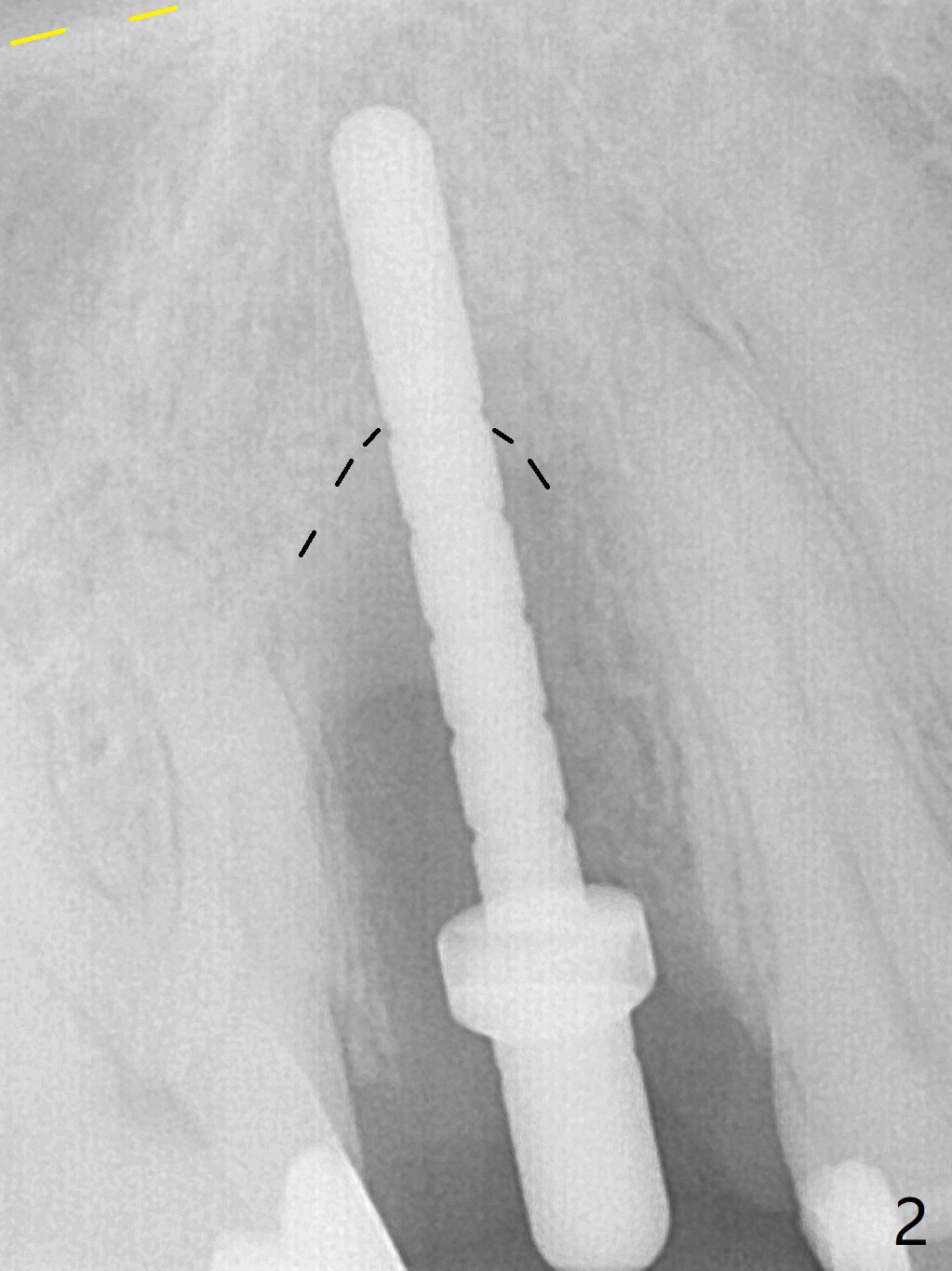
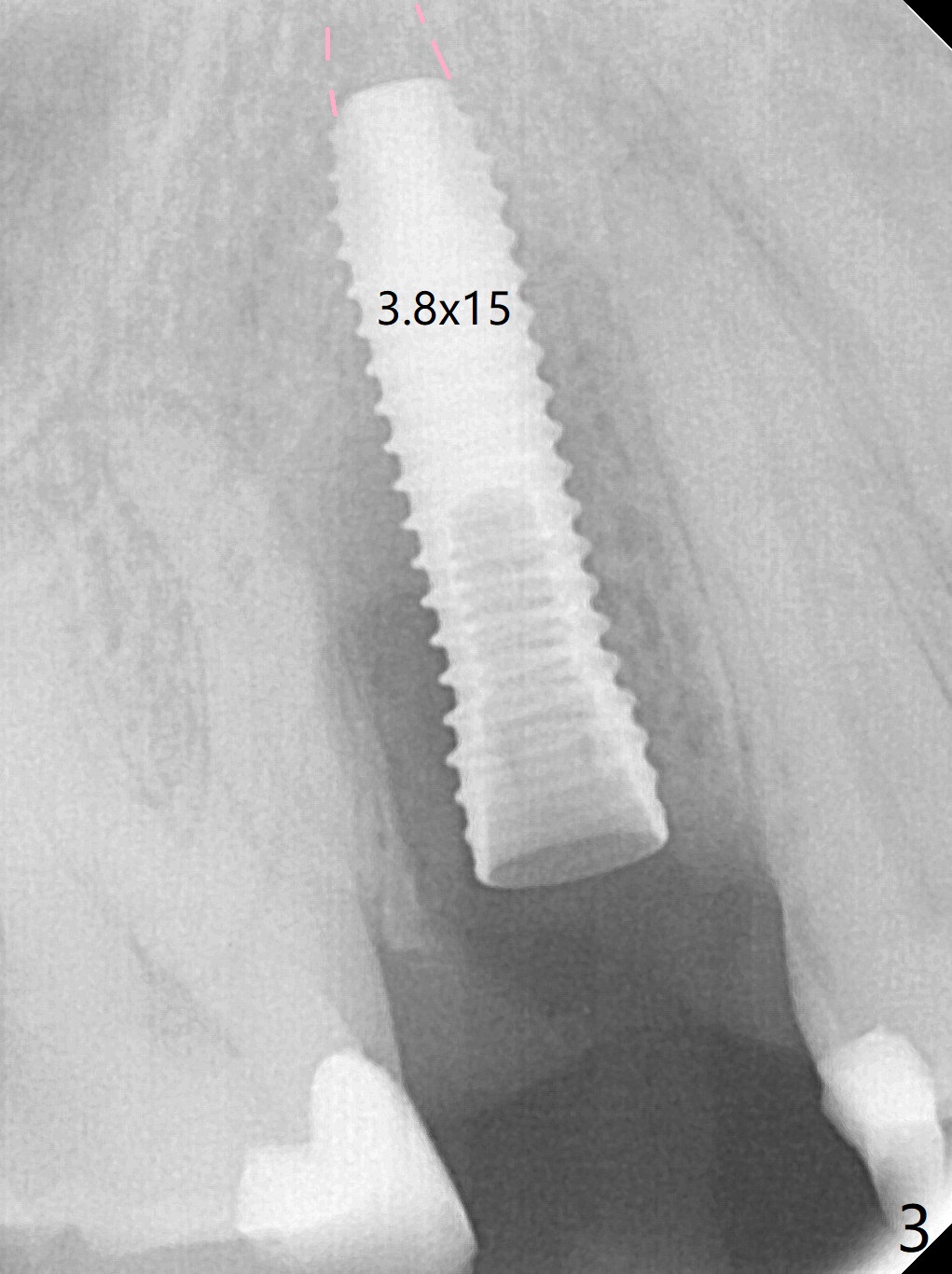
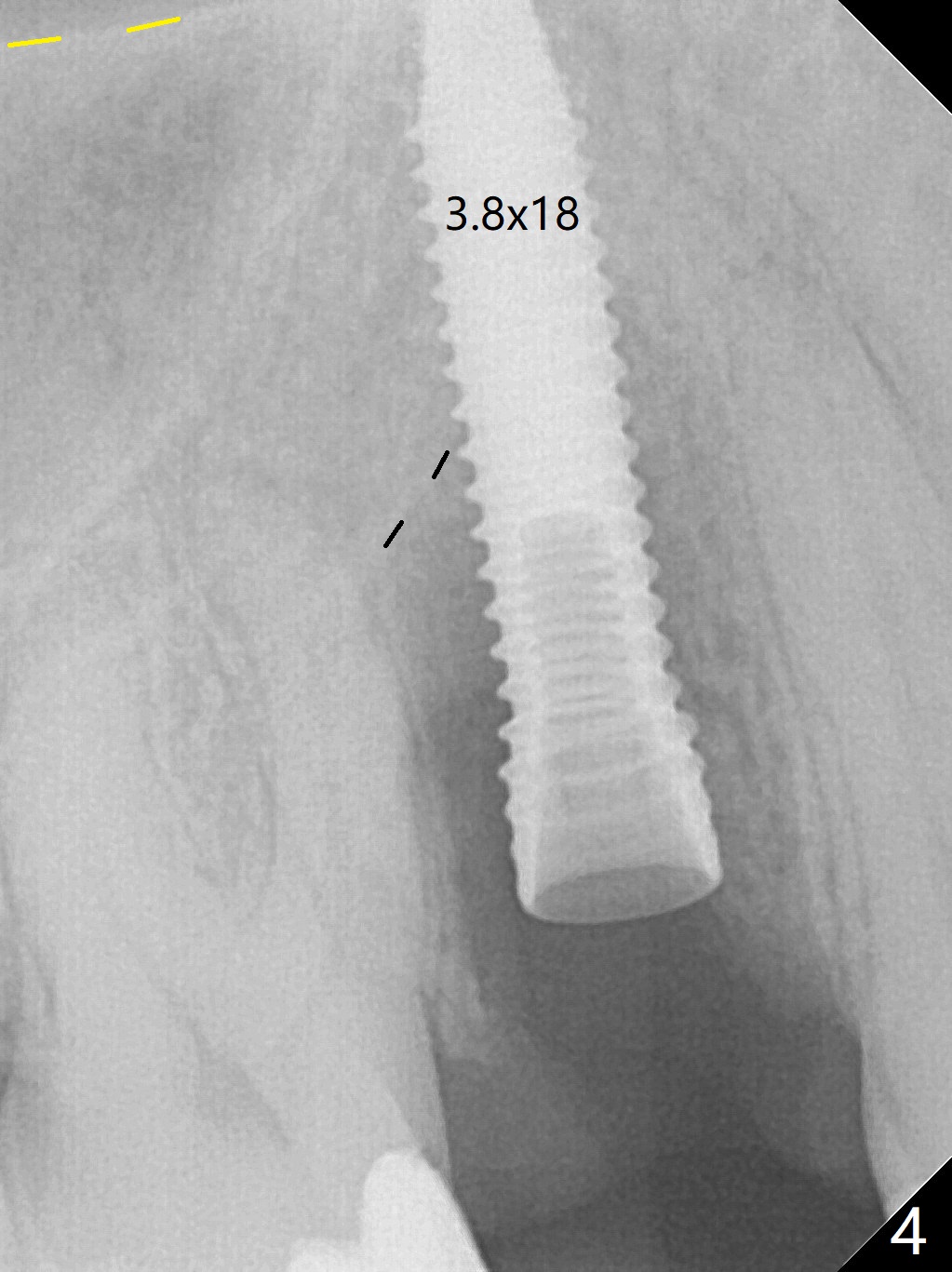
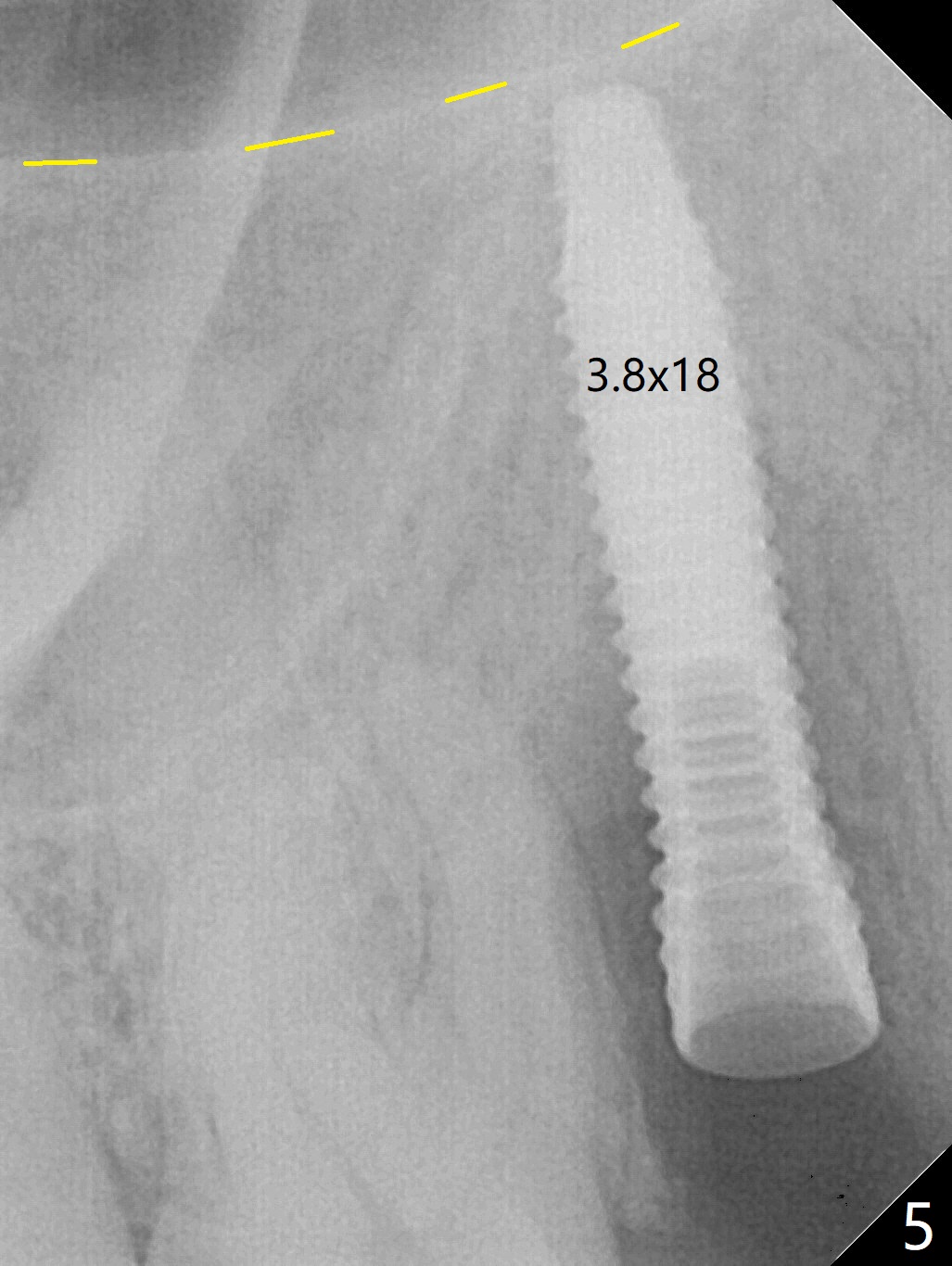
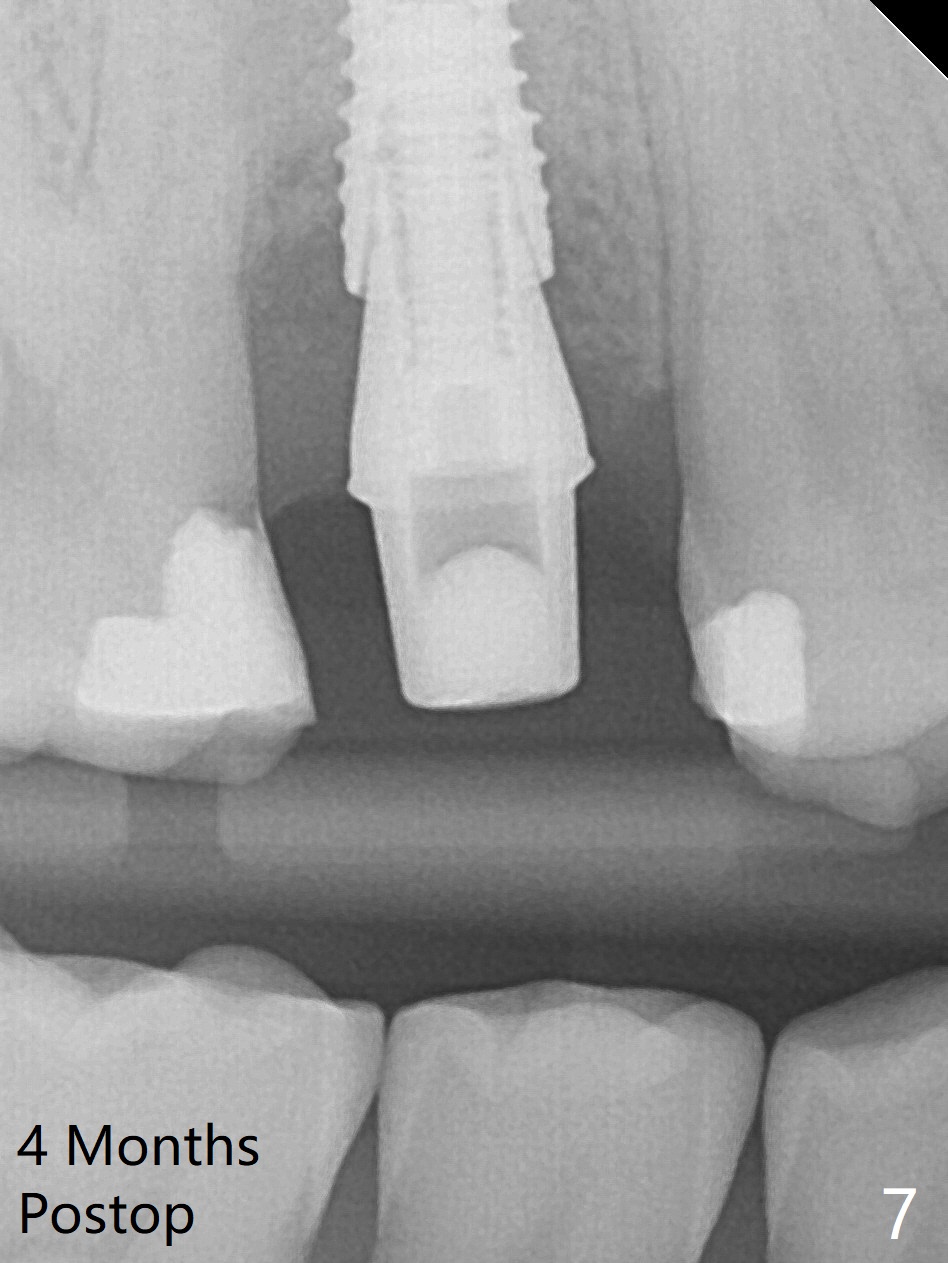
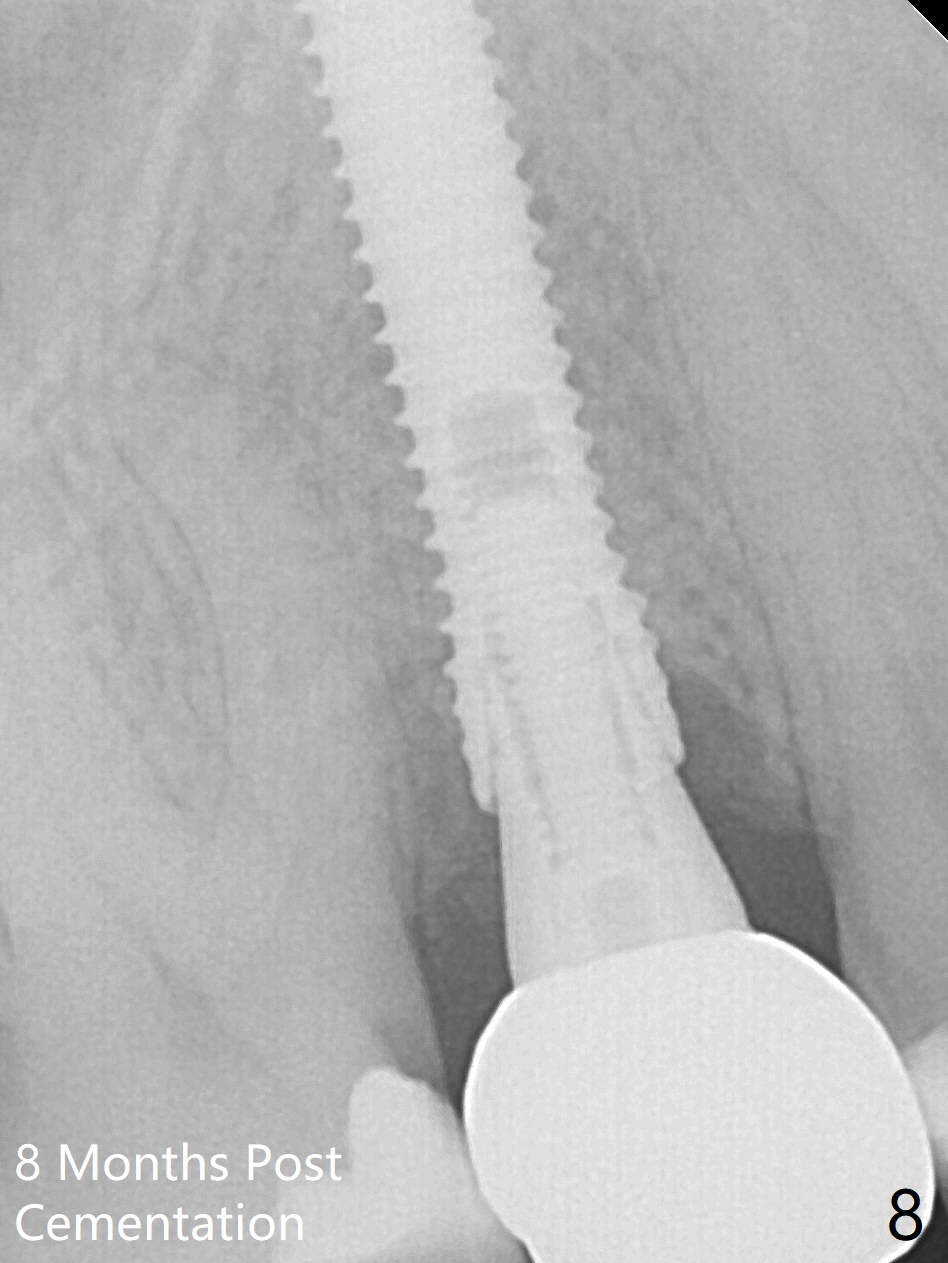
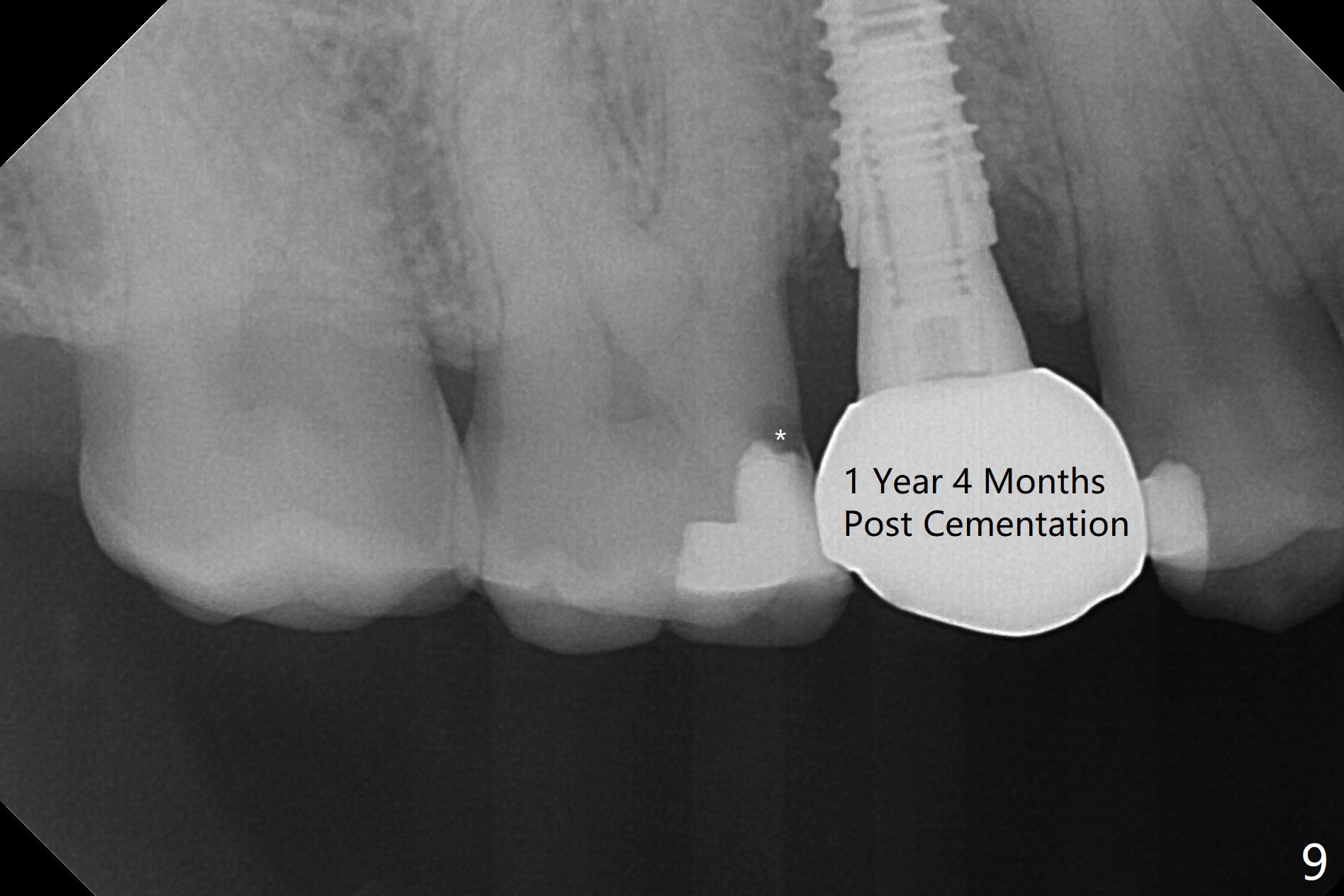
When the tooth #4 with vertical root fracture (Fig.1) is extracted, the buccal plate is found to be lost. The lowest point of the defect is shown as black dashed line in Fig.2 (yellow dashed line: sinus floor). After use of 2.5 mm reamer for 21 mm (buccal gingival level) and 3.0 mm reamer for ~17 mm, a 3.8x15 mm dummy implant is placed with 30 Ncm and 1.85 mm apical space (Fig.3 pink outline). A 3.8x18 mm (definitive) implant is placed with <40 Ncm with the implant plateau apical to the lingual crest (Fig.4,5). The buccal plate defect is repaired by Vanilla Graft (Fig.6 *) before and after insertion of a 4.5x4(3) mm abutment. The buccal plate defect seems to being repaired 4 months postop (Fig.7). Occlusal wear suggests bruxism, which is also associated with the root fracture. Night guard is recommended. The defect repair is close to completion 8 months post cementation (Fig.8). The crown/abutment is found to be loose 1 year 4 months post cementation and retightened without checking whether there is clinical 2nd DO caries of #3 (Fig.9, "sensitive to water pik"). A few days later, DO composite is being removed. It is difficult to determine whether the 2nd DO caries or gap has been removed with the neighboring crown in place. When the crown/abutment is removed and gingival retractions are inserted, there is no decay. The gap is removed. With Toflemire in place, the crown/abutment is reseated and hand tightened; after packable composite, the crown/abutment is removed, there is no more DO gap.
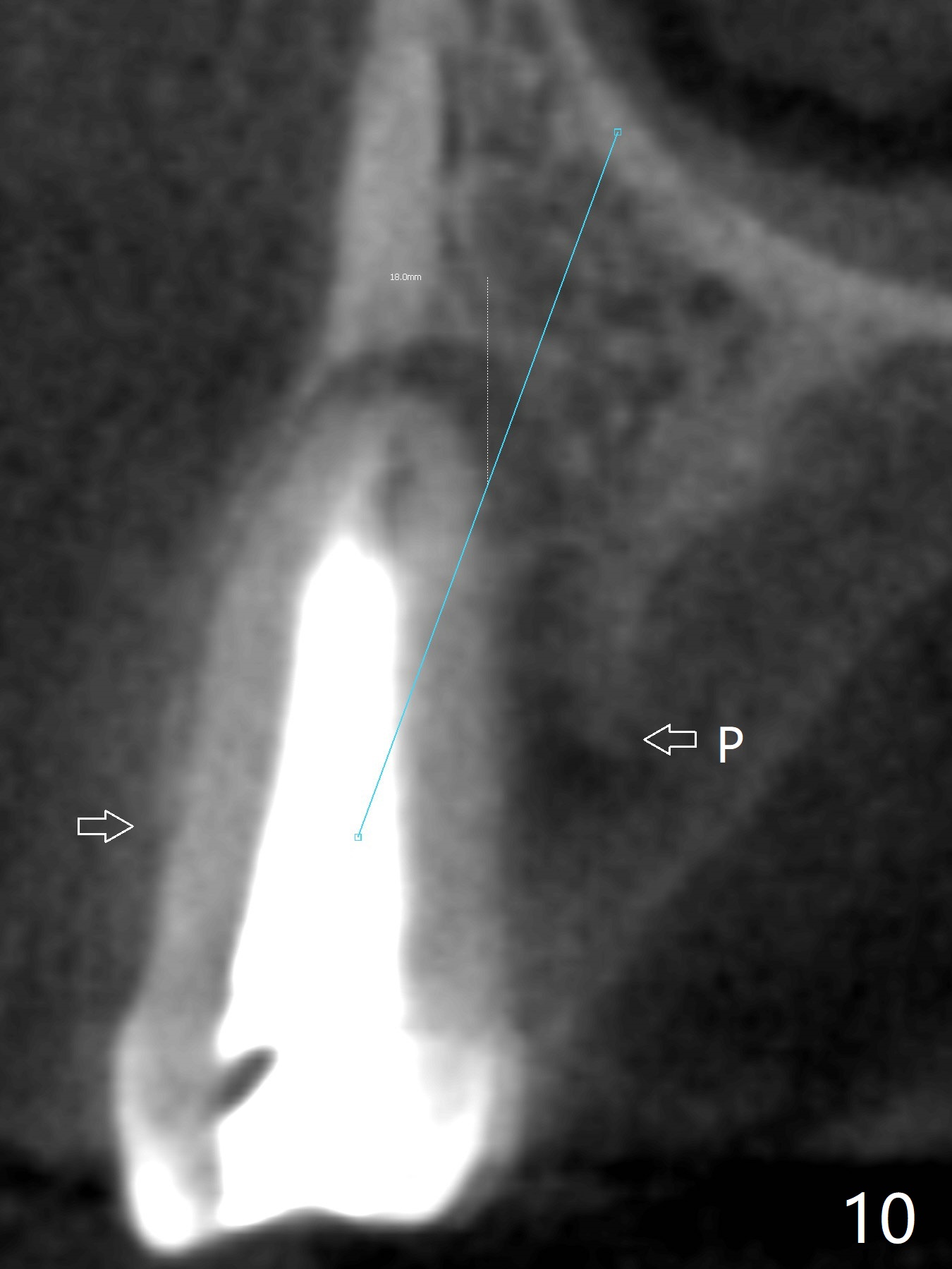
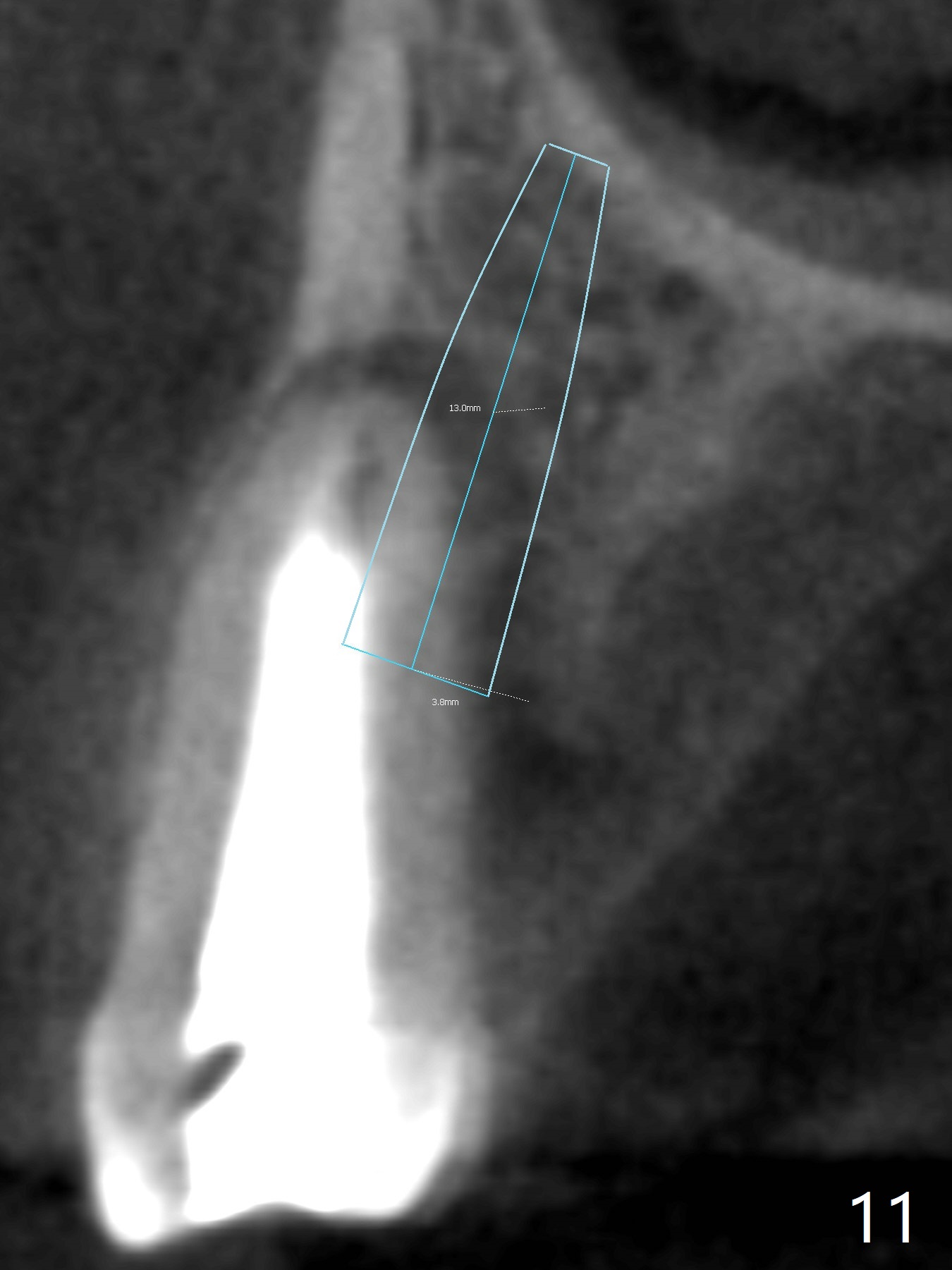
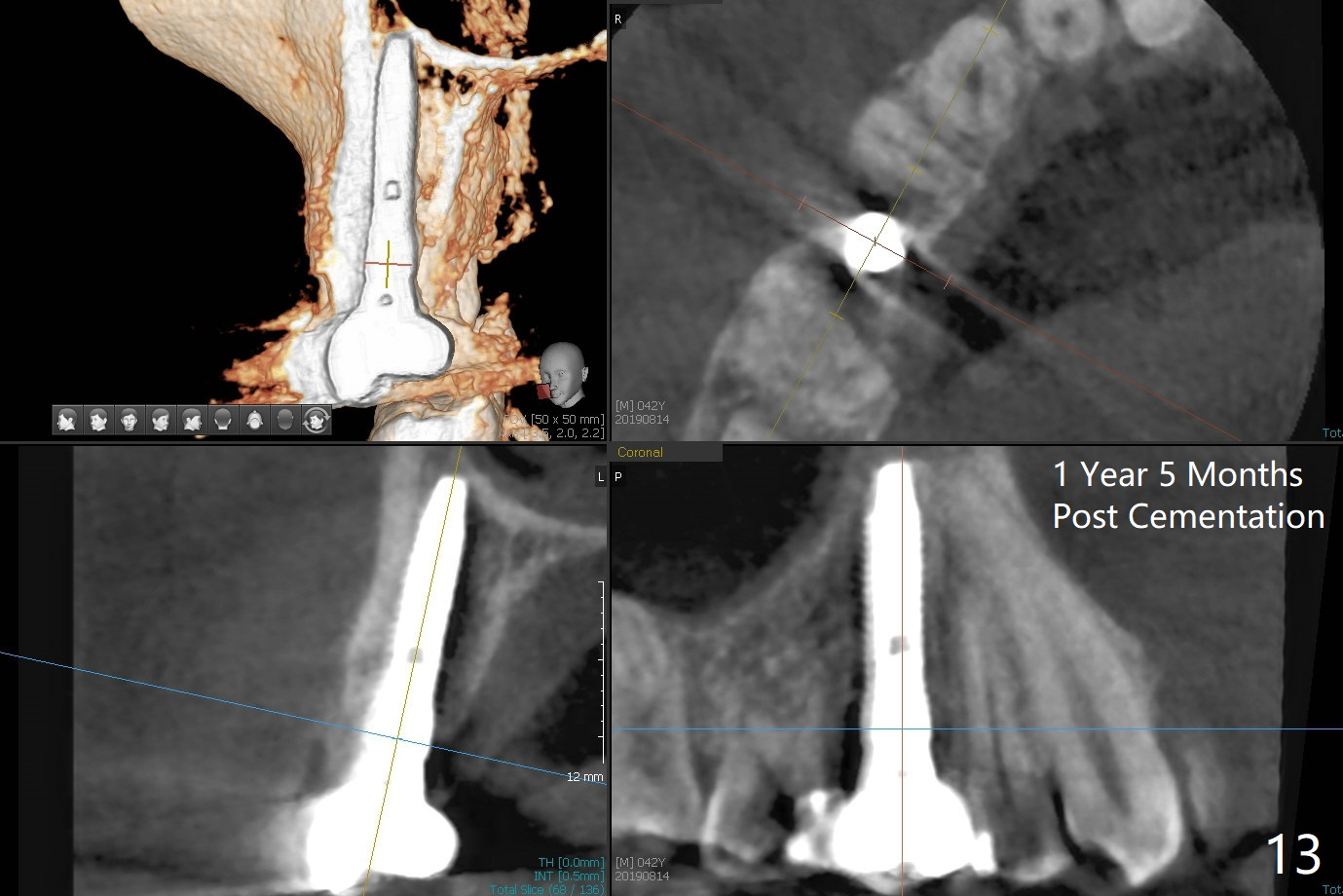
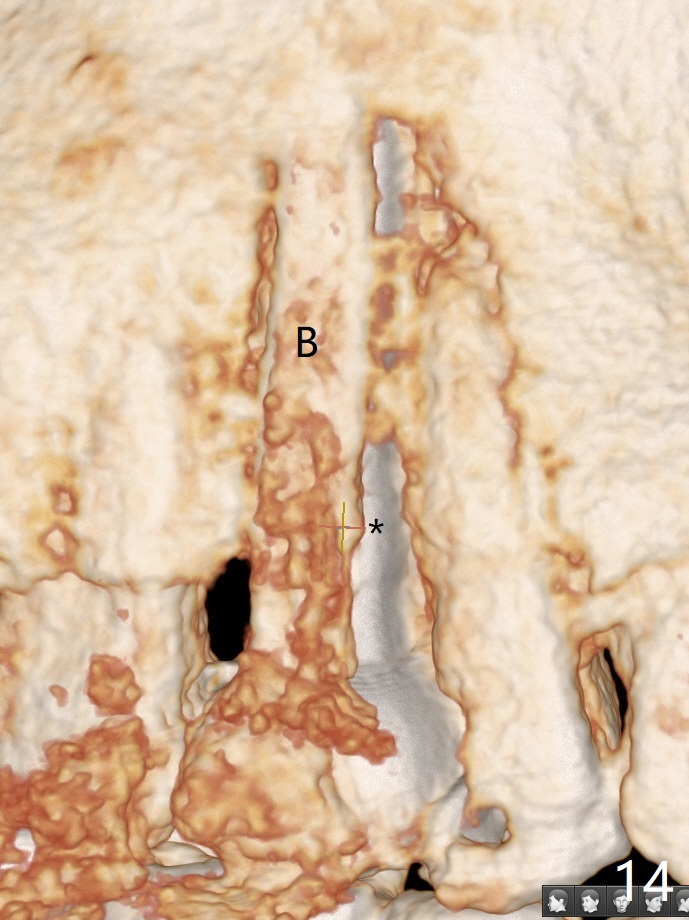
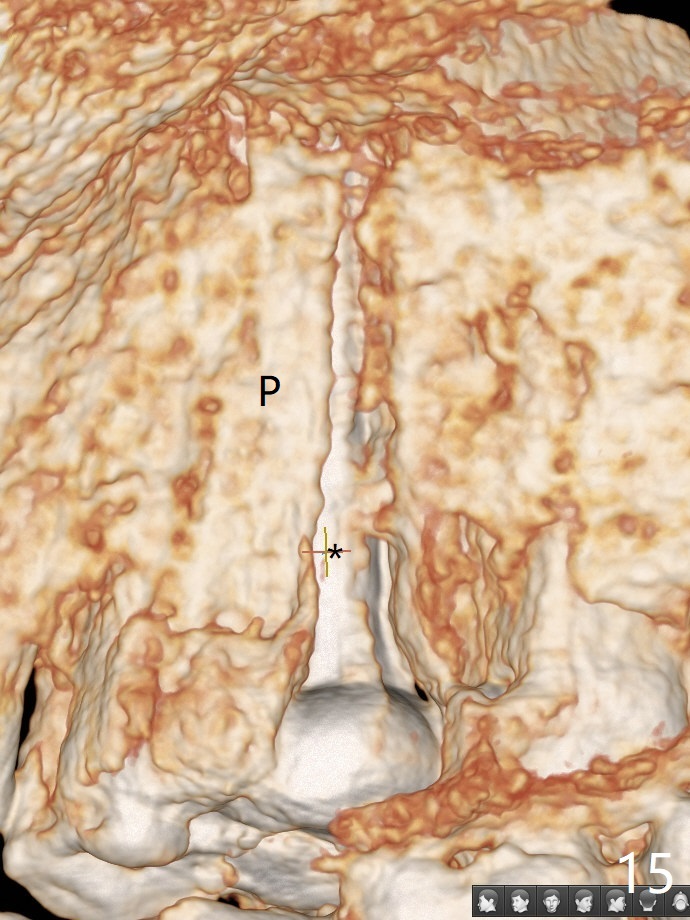
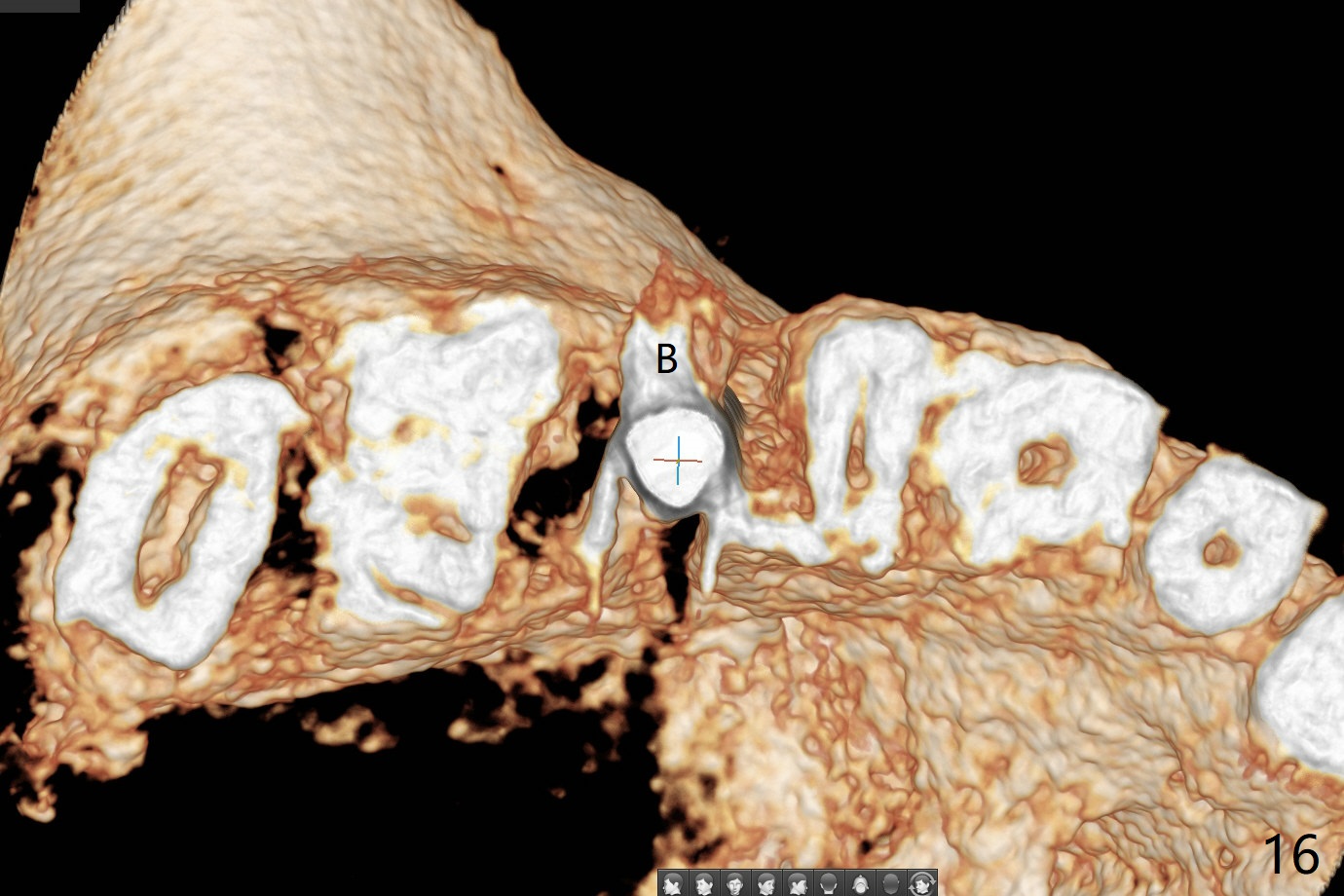
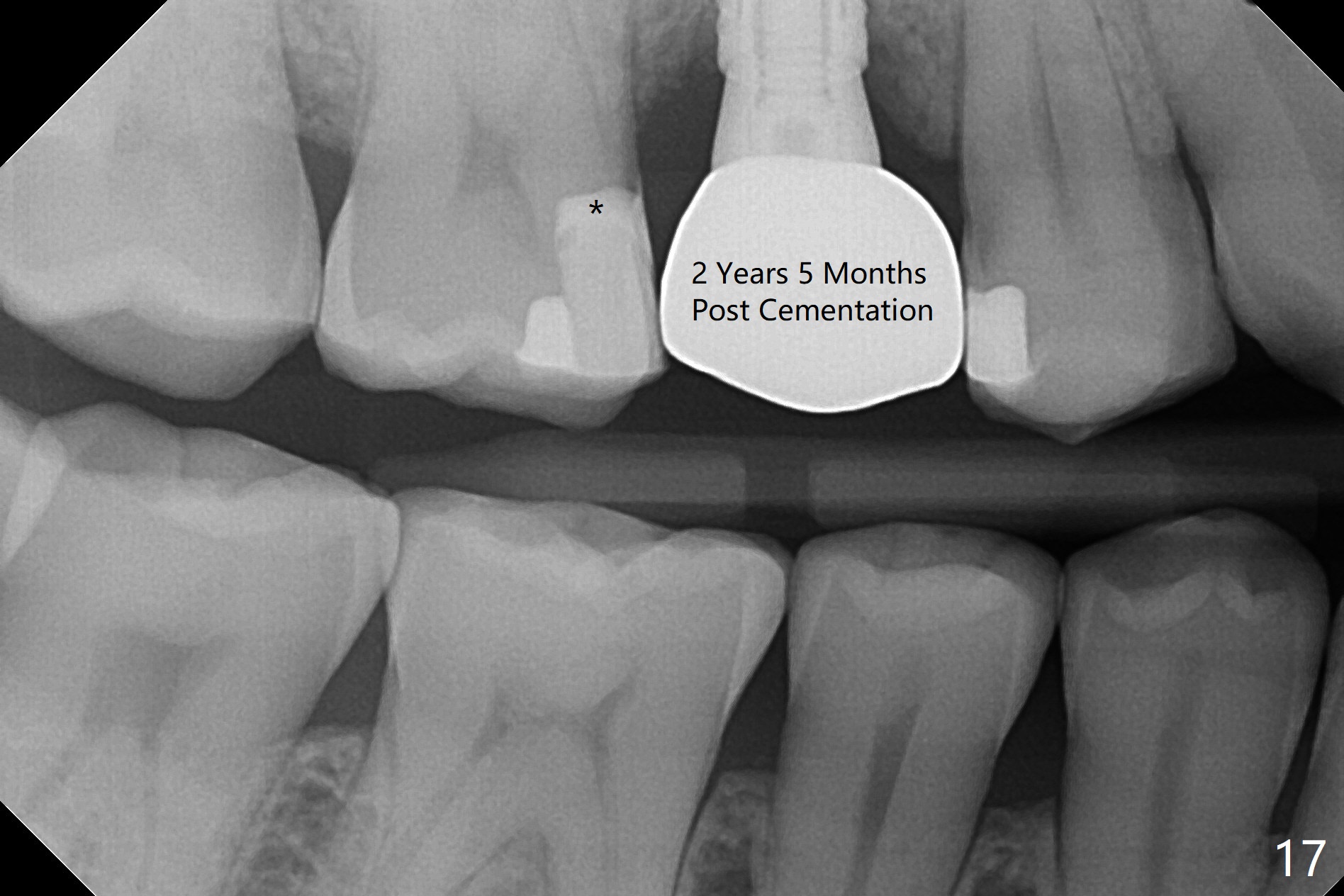
In fact there is a small buccal fistula, which is communicated with the underlying implant threads. Although preop CT shows that the buccal crest is lower than the palatal (3.8x13 mm, Fig.10 P) one, intraop finding of missing buccal plate should dictate a shorter implant (Fig.11) or onlay graft to avoid periimplantitis. Regeneration of the bone plate is limited. Later the fistula disappears with formation of a concavity (Fig.13). There is no symptom. Is bone graft necessary with a remote incision? 3-D images of CT taken 1 year 5 months post cementation show possible mesiobuccal and distopalatal bony defects (Fig.13-16). It is possible that bone graft was placed enough palatal (Fig.16). DO composite at #3 is redo satisfactorily (Fig.17 *).
Bone graft: 2 PRF membranes and 2 pieces of sticky bone buccal and palatal. Remove crown/abutment (incomplete seating) and place healing screw. Cover wound with Cytoplast and Acrylic dressing.
Return to
Upper Premolar Immediate Implant,
IBS,
Trajectory II
No Deviation
Xin Wei, DDS, PhD, MS 1st edition 10/20/2017, last revision 03/06/2021