
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|||||
Protocol for Bone Graft and Immediate Provisional for Upper 1st Molar
An immediate provisional is able to keep bone graft in place more securely than perio dressing. After immediate implant and abutment placement, a strip of gauze is inserted into the peripheral socket gap so that shaving does not drop into the gap during margin prep. The immediate provisional is fabricated. Rinse out the shaving and the gauze is removed. Bone graft is placed in the remaining gap, followed by collagen dressing if there is space. The provisional is cemented.
If bone graft is placed in the coronal aspect of the socket first, cut a piece of plastic from implant bag with a hole in the middle and place it over the implant and socket. In this way, acrylic for fabrication of the provisional does not stick to the graft.
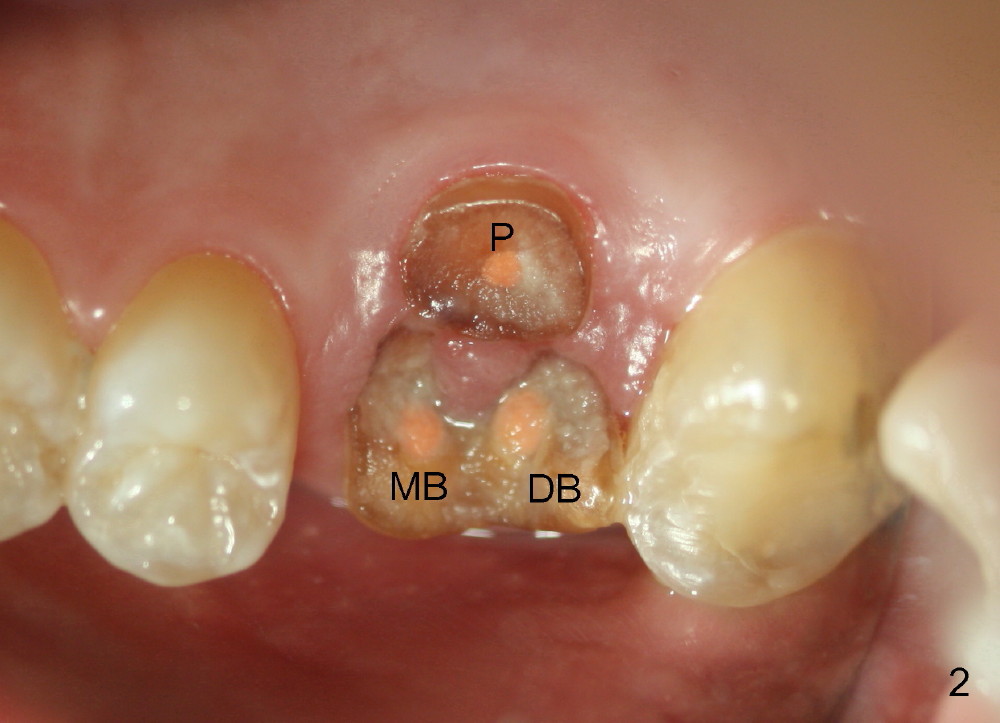
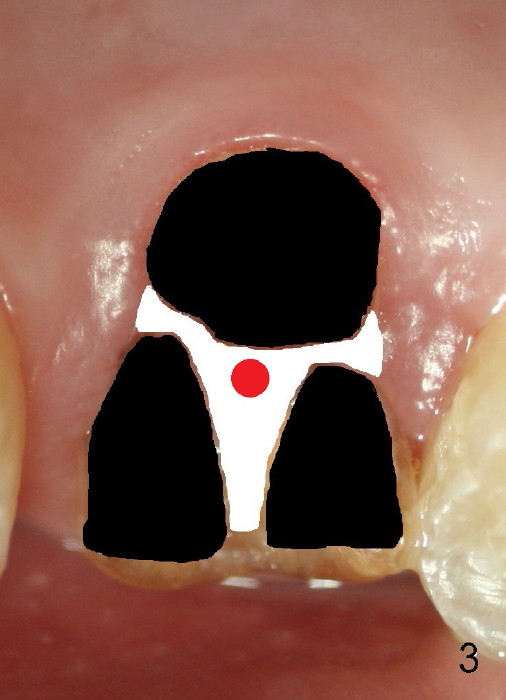
The 1st approach is used for the following case: a 46-year-old man with #14 (Fig.1). The root stumps are large and relatively close to each other (Fig.2 mirror view) so that when the roots are extracted (Fig.3 black), the septum is narrow (white). A 1.2 mm pilot drill penetrates the septum (red).
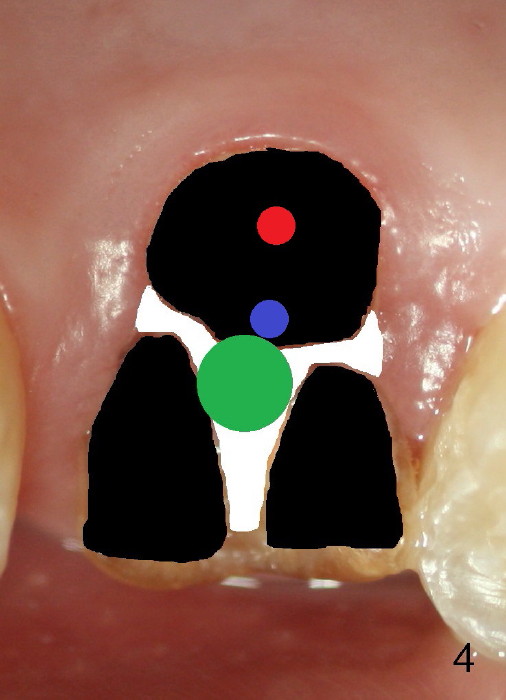
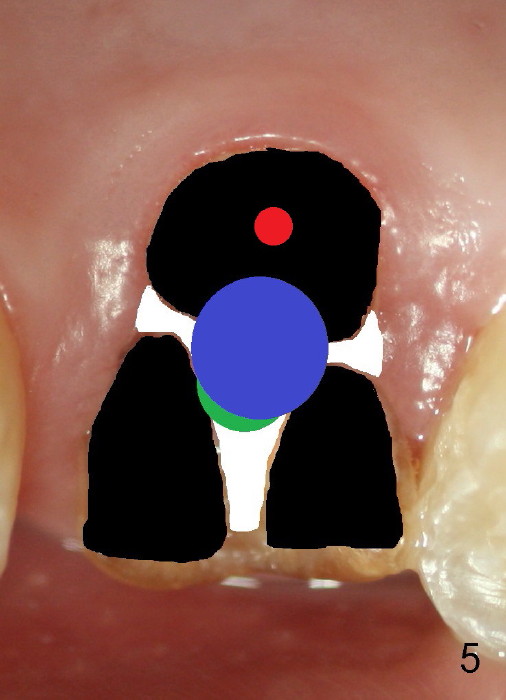
By the time a 2.6 mm bone expander is used, the septum starts to break off (Fig.4 green). The osteotomy site has to be changed: first to the palatal slope of the palatal socket (red) with the coronal end of the drill leaning buccally. Suddenly a better idea occurs: new osteotomy remains in the palatal socket, but as buccally as possible (blue) and finishes with rounded tapered osteotomes 2-4 mm at ~17 mm deep. The coronal end of the osteotomes is controlled to be positioned in the center of the socket (Fig.5 blue).
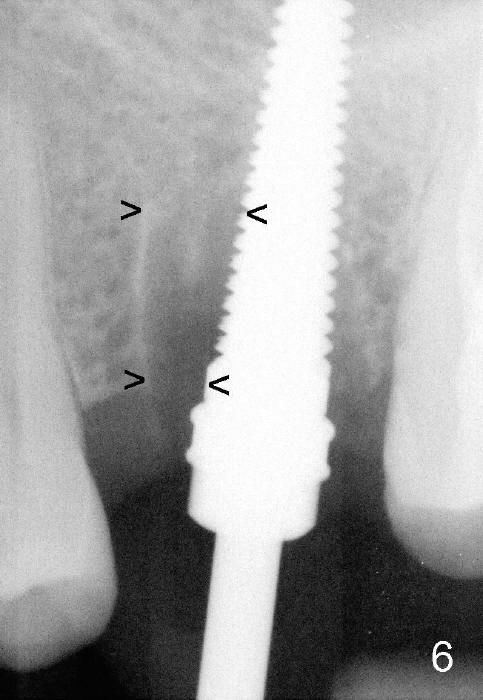
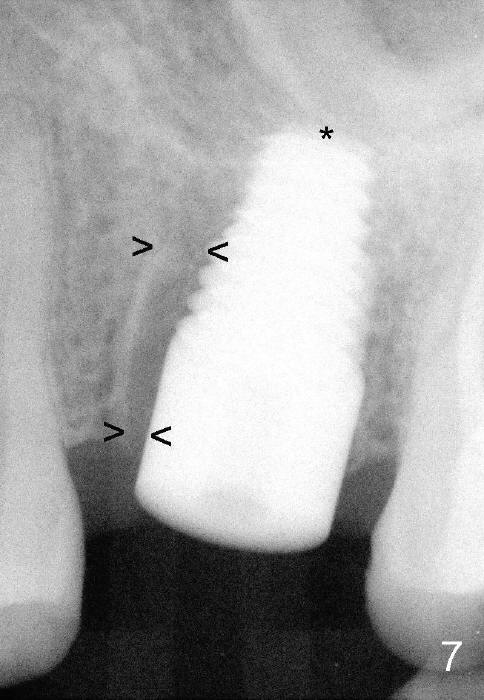
Fig.6 shows 4.5 mm tap in place with stability. It appears too high. When it is removed, the sinus membrane is found to have been perforated. The next taps (5,6 and 7 mm) are placed shorter by 3 mm with stability. A piece of collagen dressing and a small amount of bone graft (Fig.7 *) are inserted to the osteotomy before placement of a 7x14 mm implant.
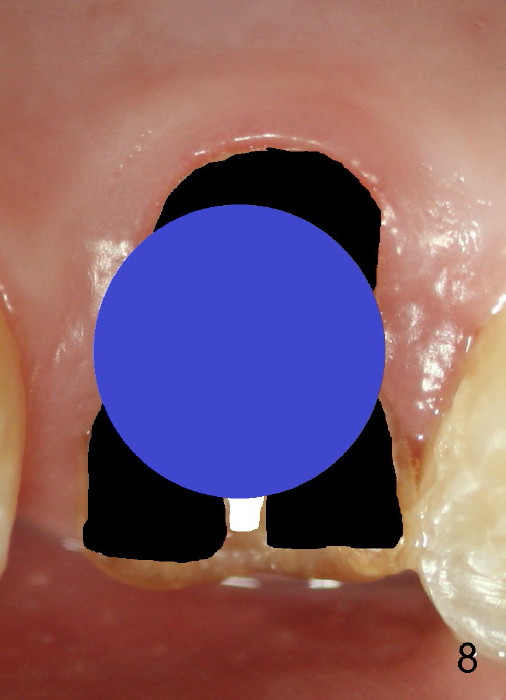
Fig.8 illustrates the implant (blue) placed in the middle of the socket. The remaining buccal and lingual gaps (black) are then closed by graft and membrane. Placing the graft in the deeper portion of the mesiobuccal socket is not so easy because the large implant blocks the entrance (Fig.7 between lower arrowheads). If more graft has been dispensed and the earlier PA shows larger upper space exists (Fig.6 between upper arrowheads), the graft should be placed to that region prior to implant placement.
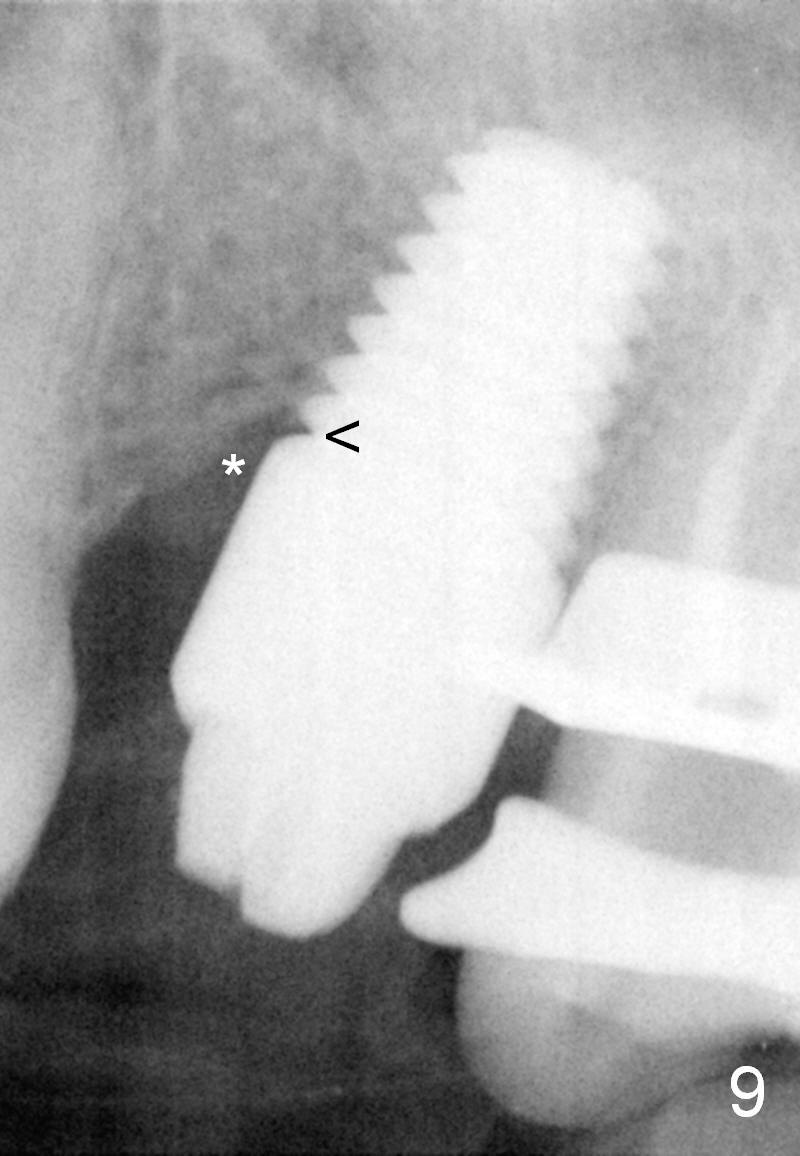
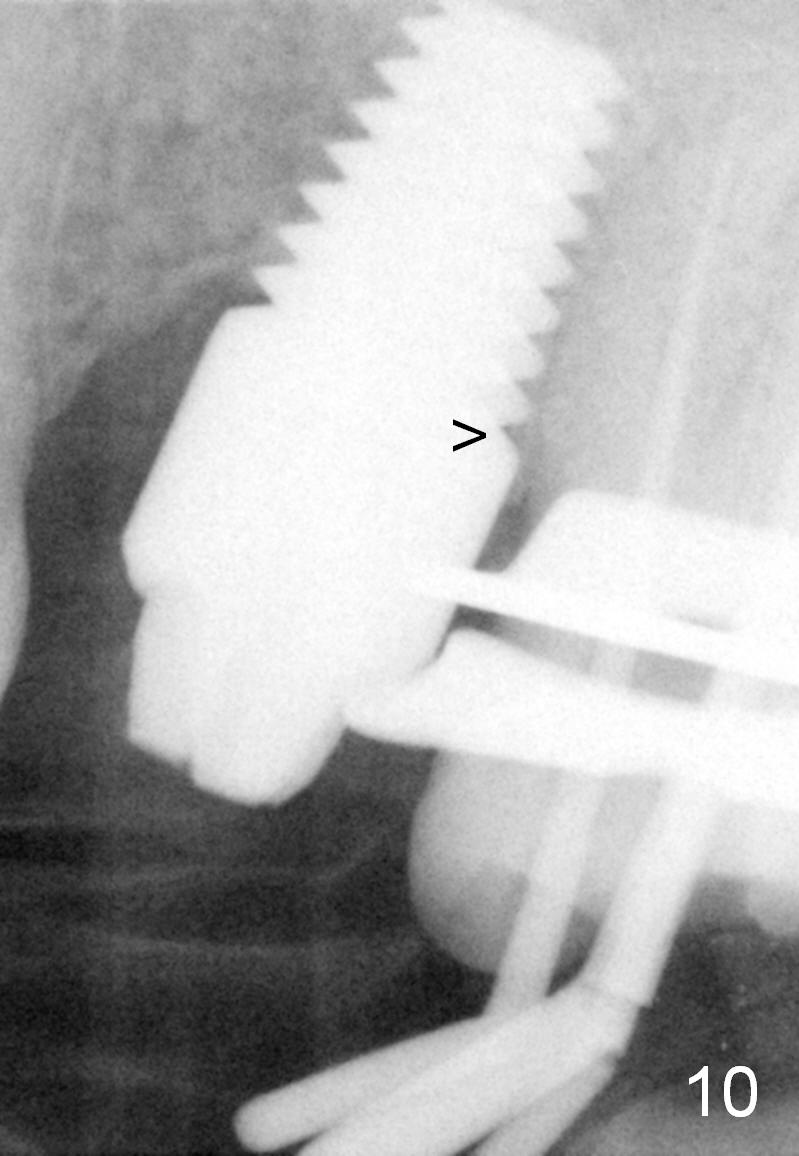
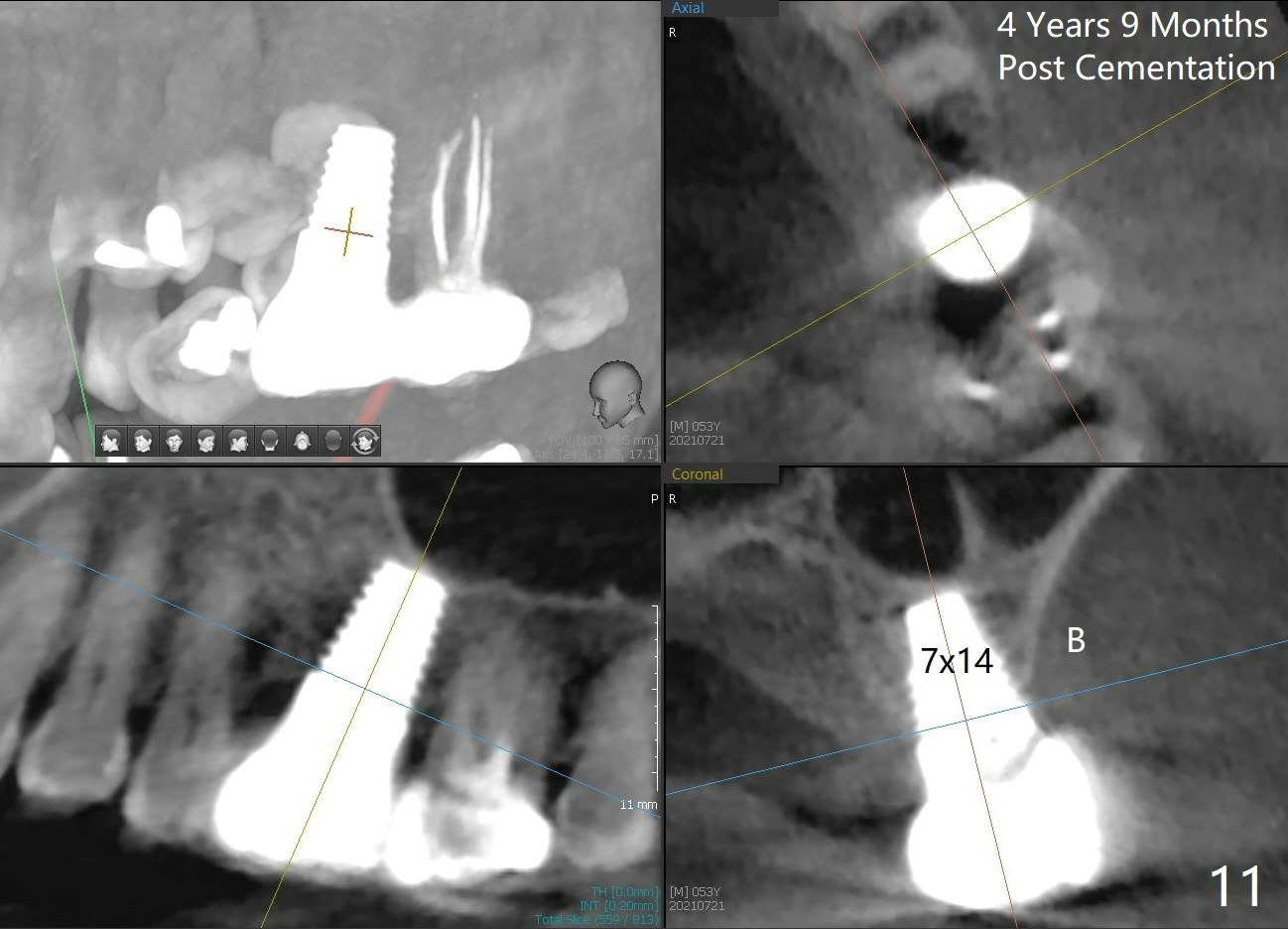
Twenty-one months postop, the patient returns for #15 RCT. PAs show that although there is a narrow space in the original mesial socket (Fig.9 *), the 1st thread space is partially obliterated with the bone (<). In contrast, the distal 1st thread space is completely obliterated (Fig.10 >). After the RCT, impression is taken for #14 and 15. Although there is no sign of periimplantitis, the 7x14 mm implant looks too large for the site with possible buccal thread exposure 4 years 9 months post cementation (Fig.11). To reduce complications, a much small fixture will be at #30.
Return to
Upper Molar Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 12/15/2014, last revision
08/15/2021