



|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
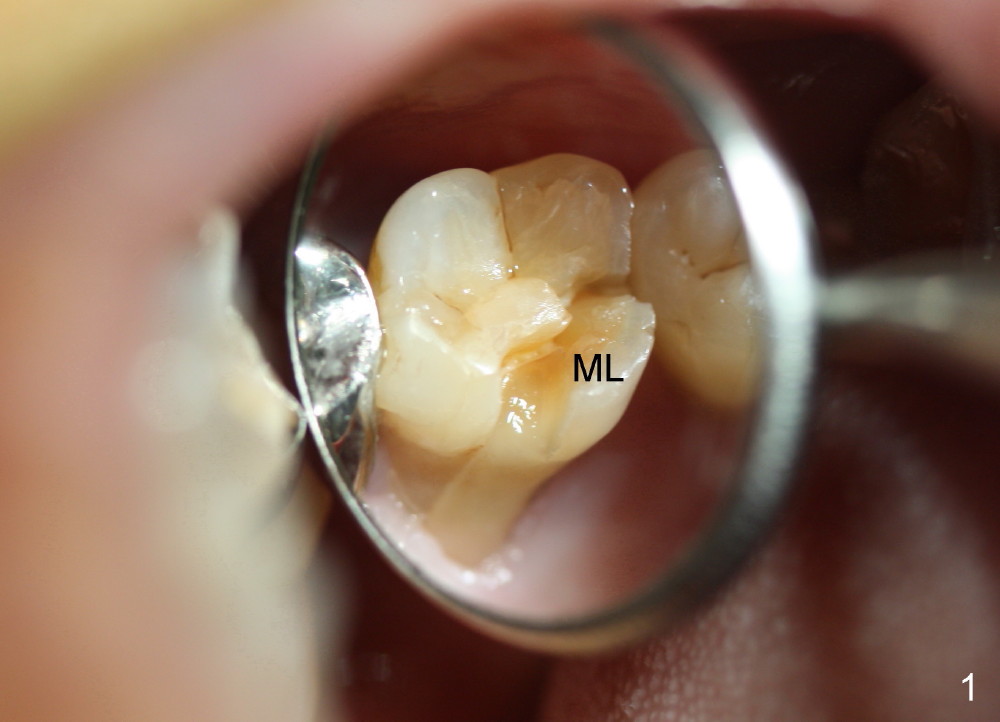
Septum of Upper 1st Molar
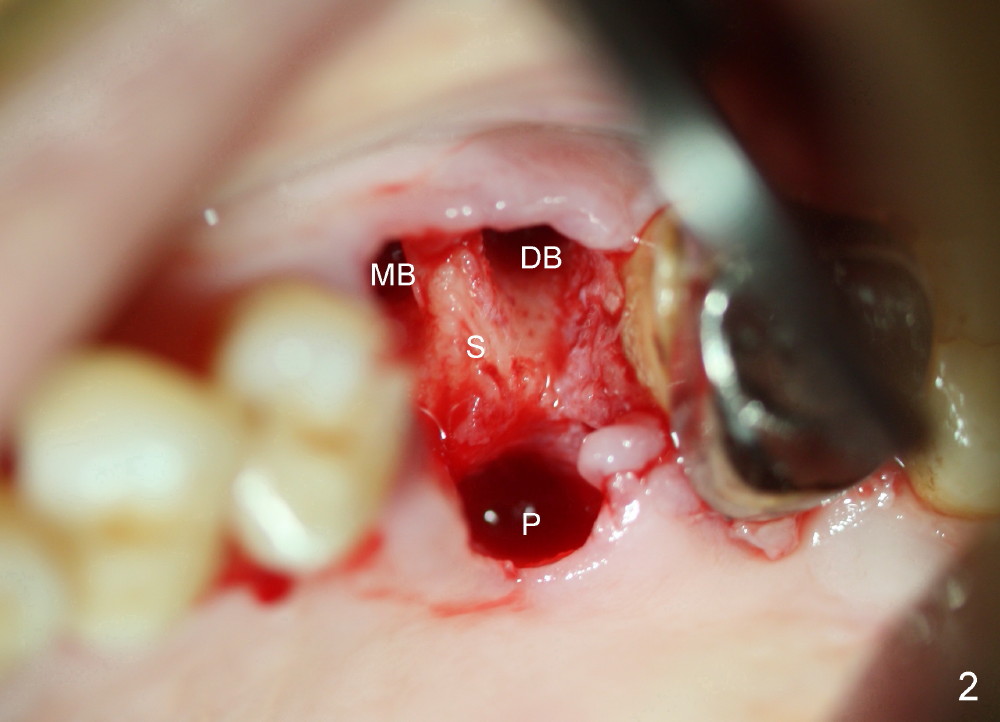
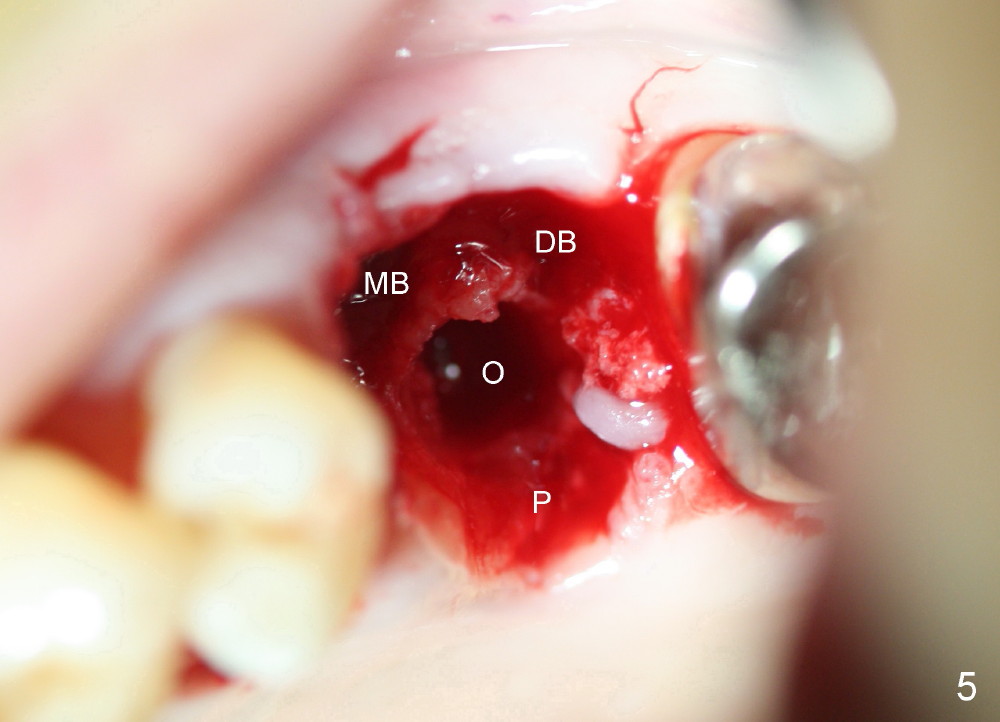
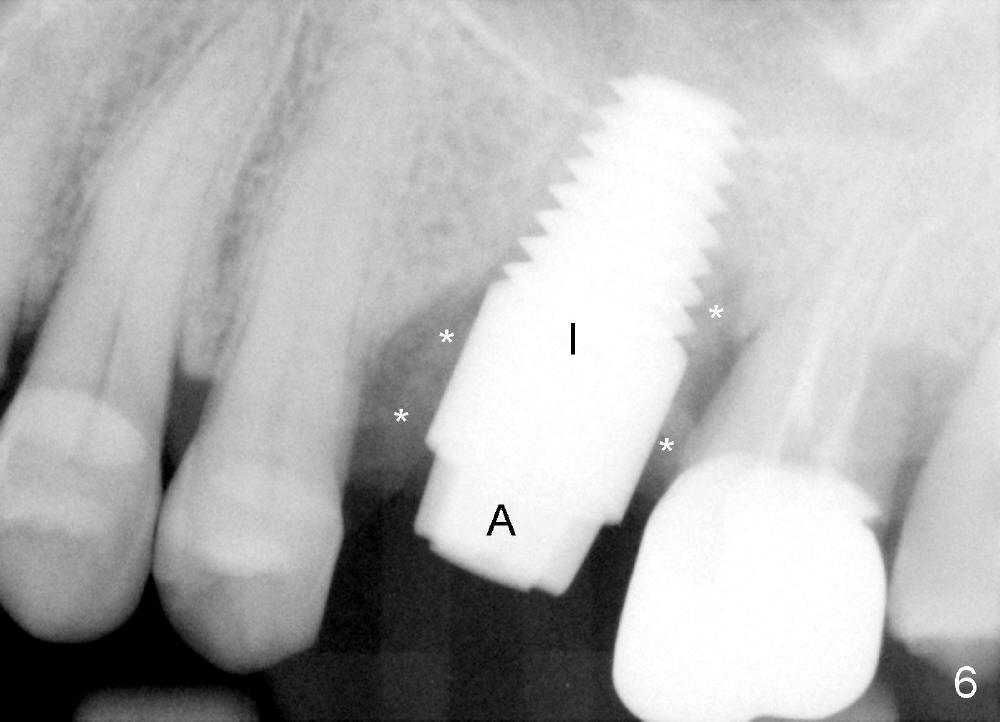
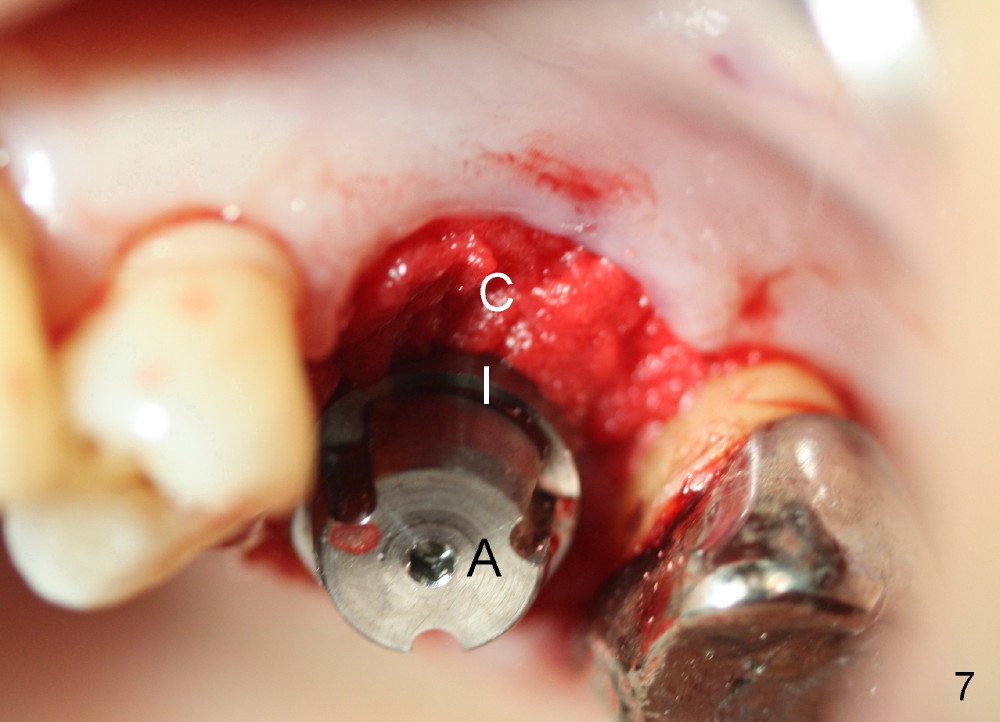
Fig.1 shows fracture of the mesiolingual cusp (ML) of the upper 1st molar. The septum (Fig.2 S) is wider than that of 2nd molar. Osteotomy starts in the septum with combination of drills, osteotomes and taps (Fig.3-5). A 7x14 mm implant is placed (Fig.6-8 I) with a 6x3 mm abutment (A), bone graft (Fig.6 *) and collagen membrane/plug (Fig.7,8 C). The latter is kept in place with perio dressing.
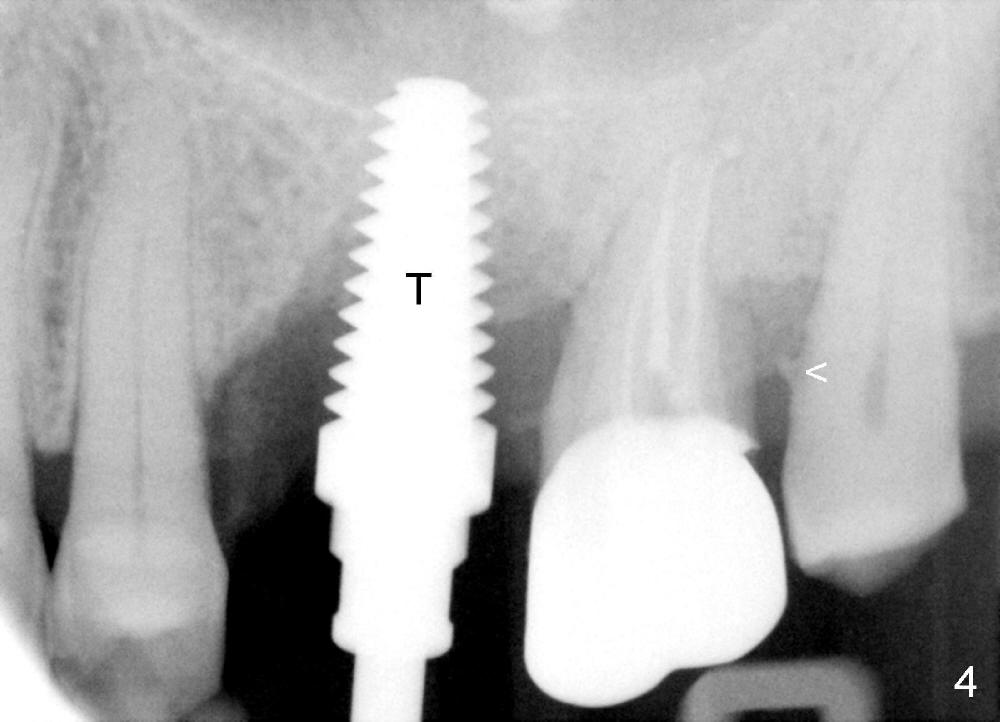
Three missions are planned (local scaling & root planing, Emdogain and immediate provisional). The first one is accomplished (compare arrowheads in preop PA, Fig.4, 6). By the time the implant is placed, the patient is tired. The last two missions are not done. The immediate provisional will be fabricated as soon as the perio dressing is dislodged, since the tooth #15 is periodontally affected. Shifting of this tooth is expected if the provisional is not provided in a timely manner.
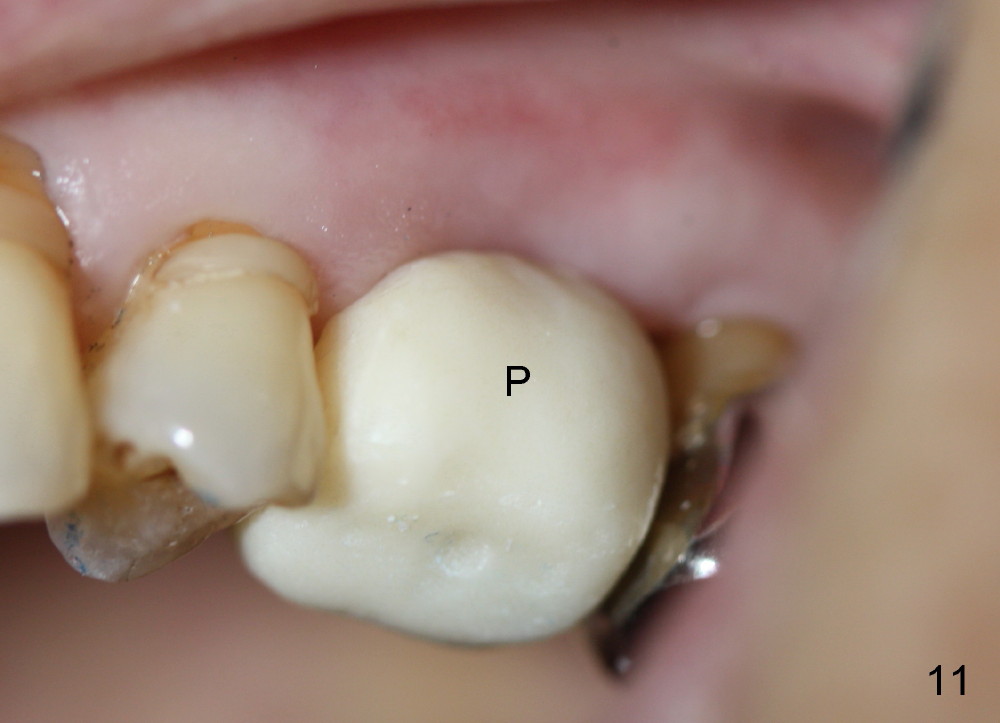
The patient returns 1 week postop. The perio dressing has dislodged. The lingual gap has closed completely (Fig.9), while the buccal partially (Fig.10). A provisional (Fig.11 P) is fabricated and cemented after initial preparation of the implant/abutment. (Fig.9,10).
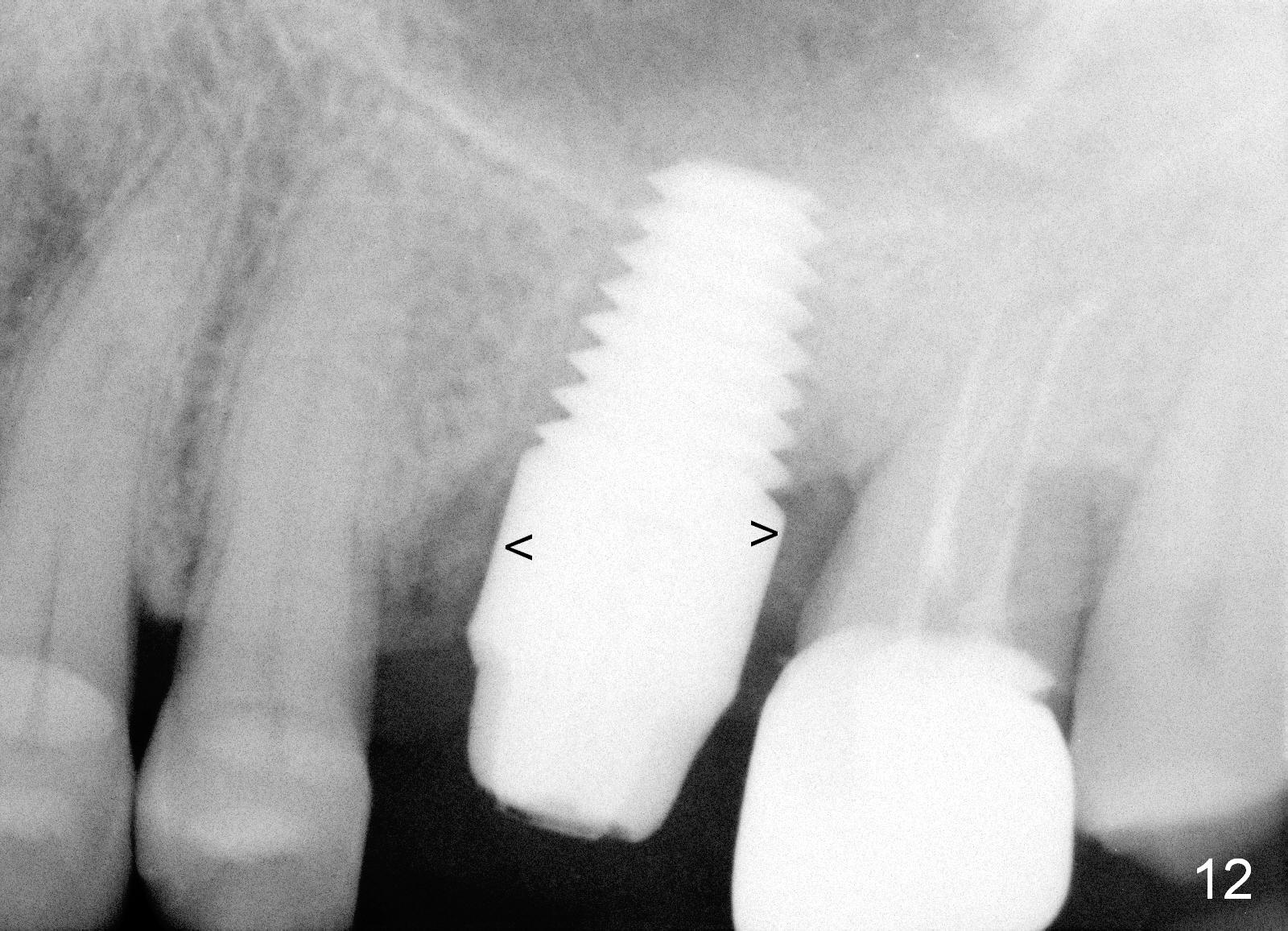
Probably due to bruxism, the provisional is not stable. Less than 2 months postop, the patient requests final restoration. After re-prep and impression, PA is taken. The latter shows that the peri-implant gaps (Fig.12 (arrowheads), as compared to Fig.6) decrease in size, while the bone density in the gap increases.
Return to
Upper Molar Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 12/06/2014, last revision 02/22/2015