

|
|
|
|
|
|
|
|
|
Immediate Implant and Immediate Provisional for Bruxer
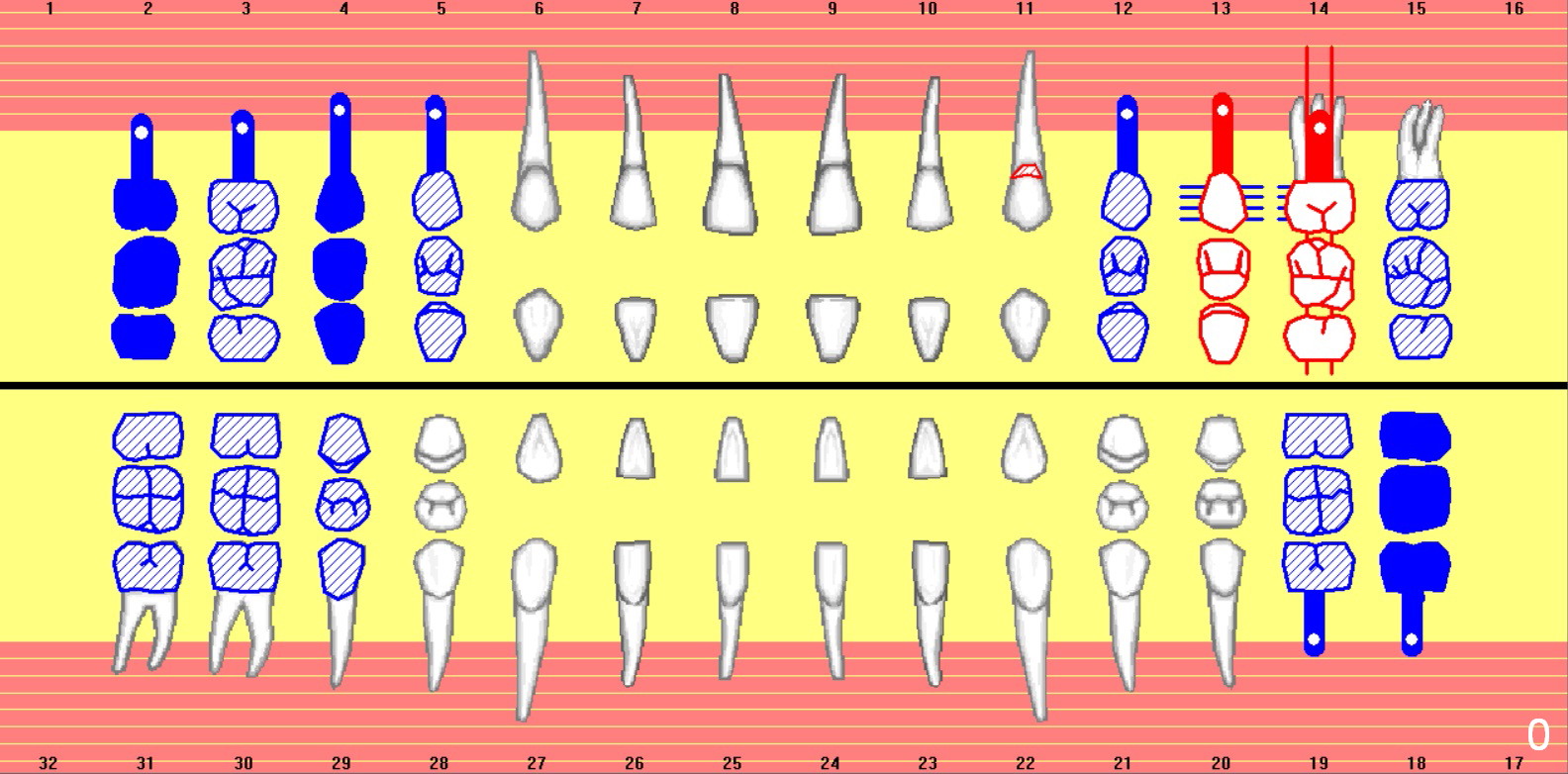
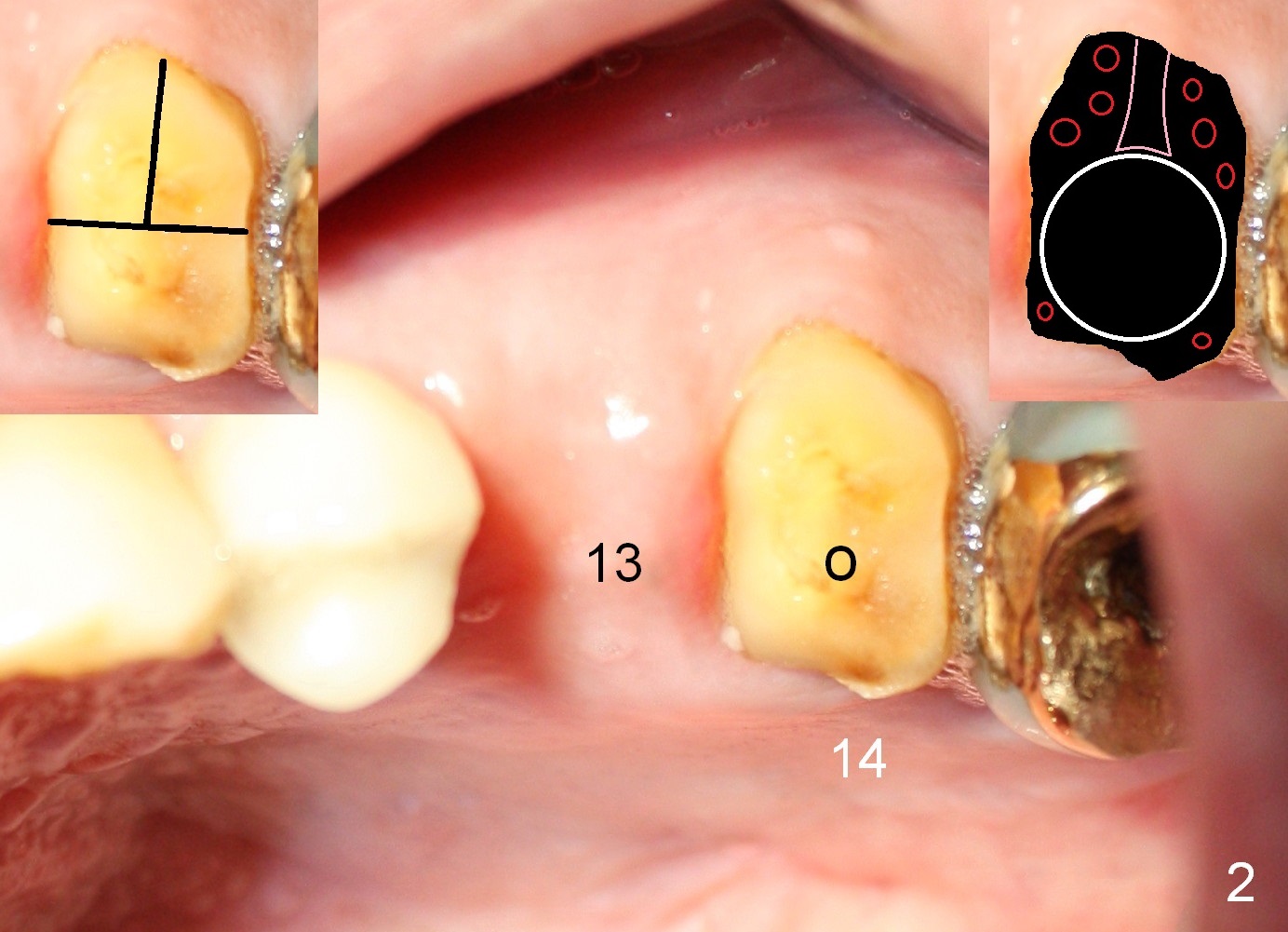
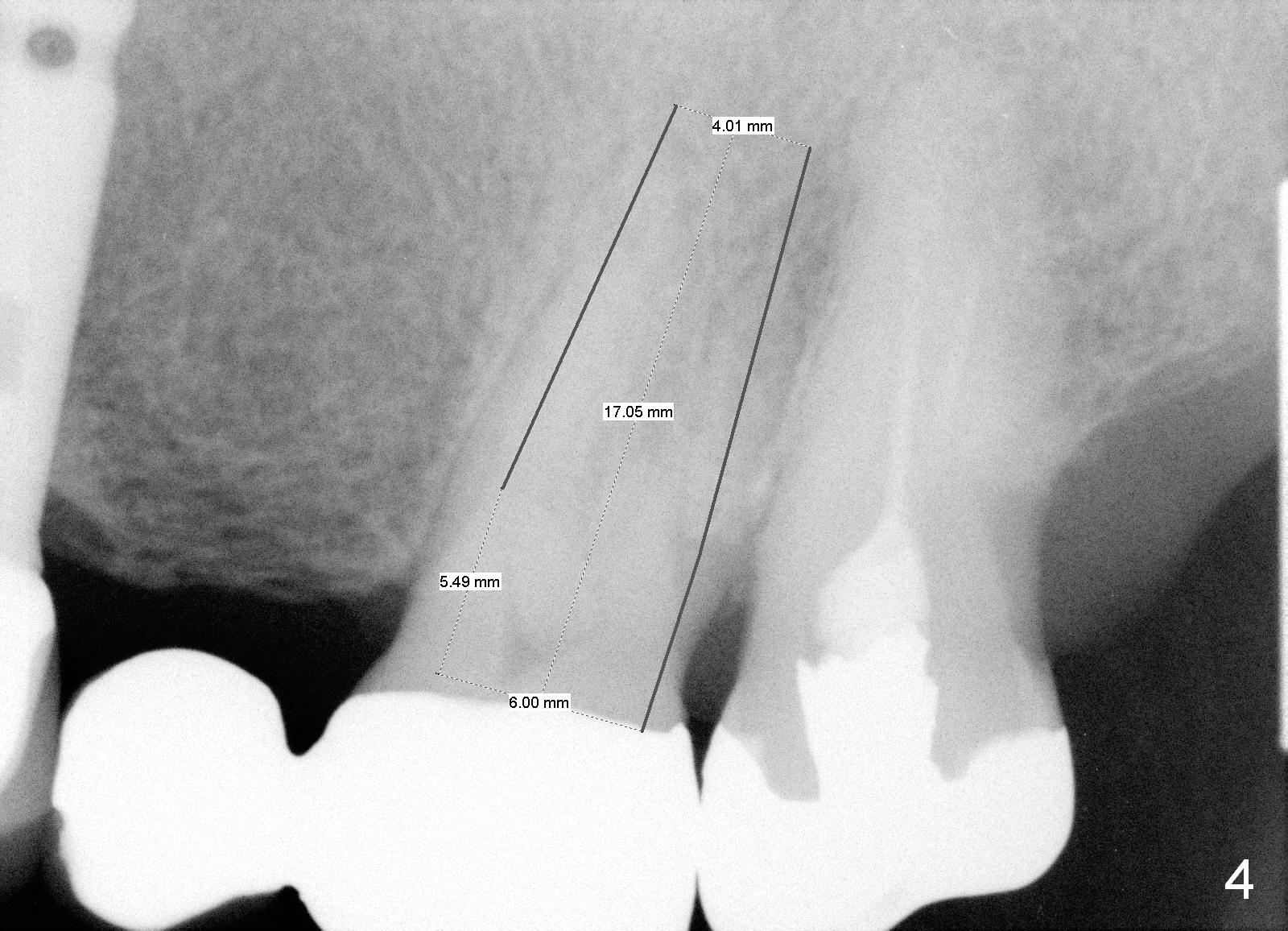
A 71-year-old man has multiple restorations, most of which are high noble crowns (Fig.0). He used to have a cantilever bridge involving the teeth #13 and 14 (Fig.1). It fractures (Fig.2,3). Considering the obliterated canals (Fig.1) and history of "bristle teeth", implants will be the best treatment option. The tooth #14 will be sectioned (Fig.3 upper left inset) for extraction. The osteotomy will be initiated in the septum slightly palatal, as shown by O in Fig.3 so that the immediate implant will be almost obliterating the socket mesiodistally (Fig.2 upper right inset white circle). The implant is also contacting the palatal wall of the socket and the buccal septal strut (pink outline) for primary stability. It appears that a 6x17 mm tissue-level implant is able to occupy the mesiodistal space (Fig.4) and that a 7 mm may be a better option. There is enough bone height for a 20 mm long implant.
An implant will be placed at the site of #13 at the same appointment. Bone will be harvested from the site of #13 while making osteotomy and transplanted into remaining sockets of #14 after implant placement (Fig.2 upper right inset red circles). If insertion torque is reasonably high for these 2 implants, an immediate provisional FPD (non-cantilever) will be fabricated to keep the papilla between the sites of #13 and 14 (Fig.3 *).
Return to
Upper Molar Immediate Implant
#2
Xin Wei, DDS, PhD, MS 1st edition 04/26/2015, last revision 06/11/2019