



|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
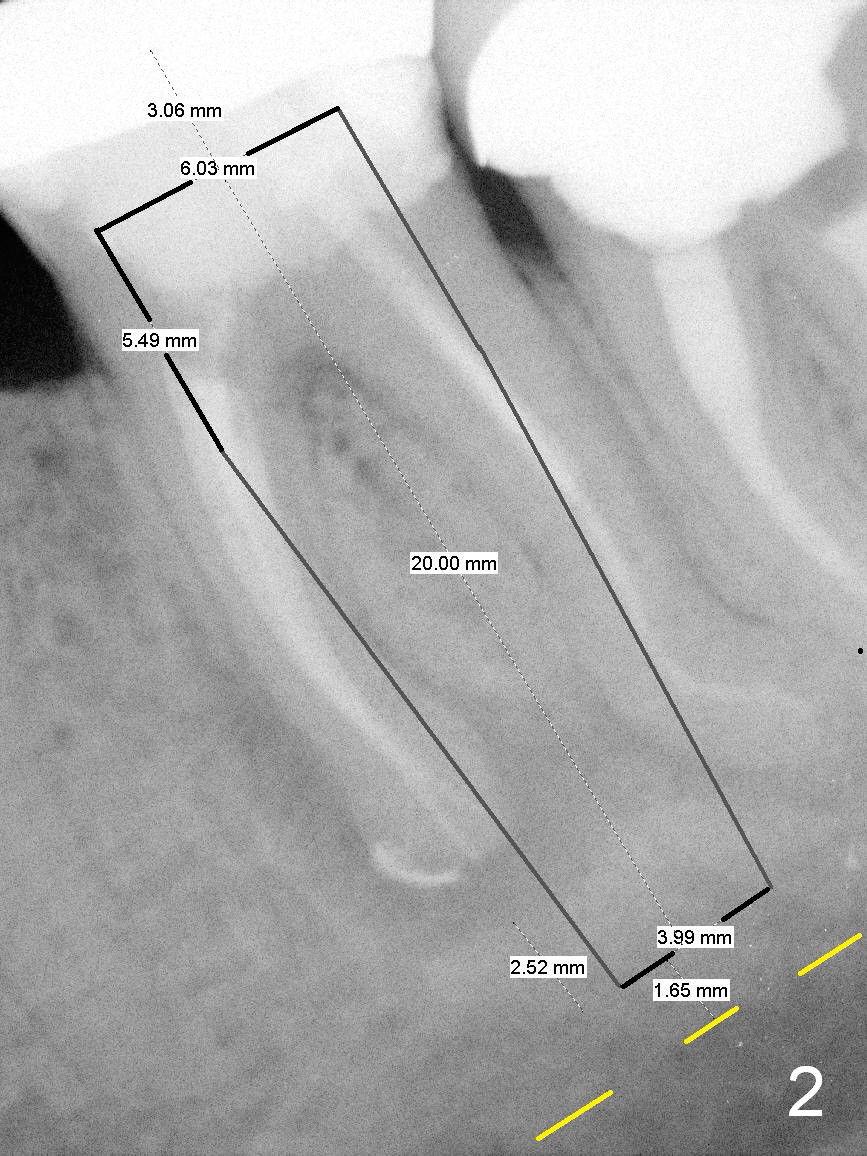
Septal Struts for Immediate Implant Stability
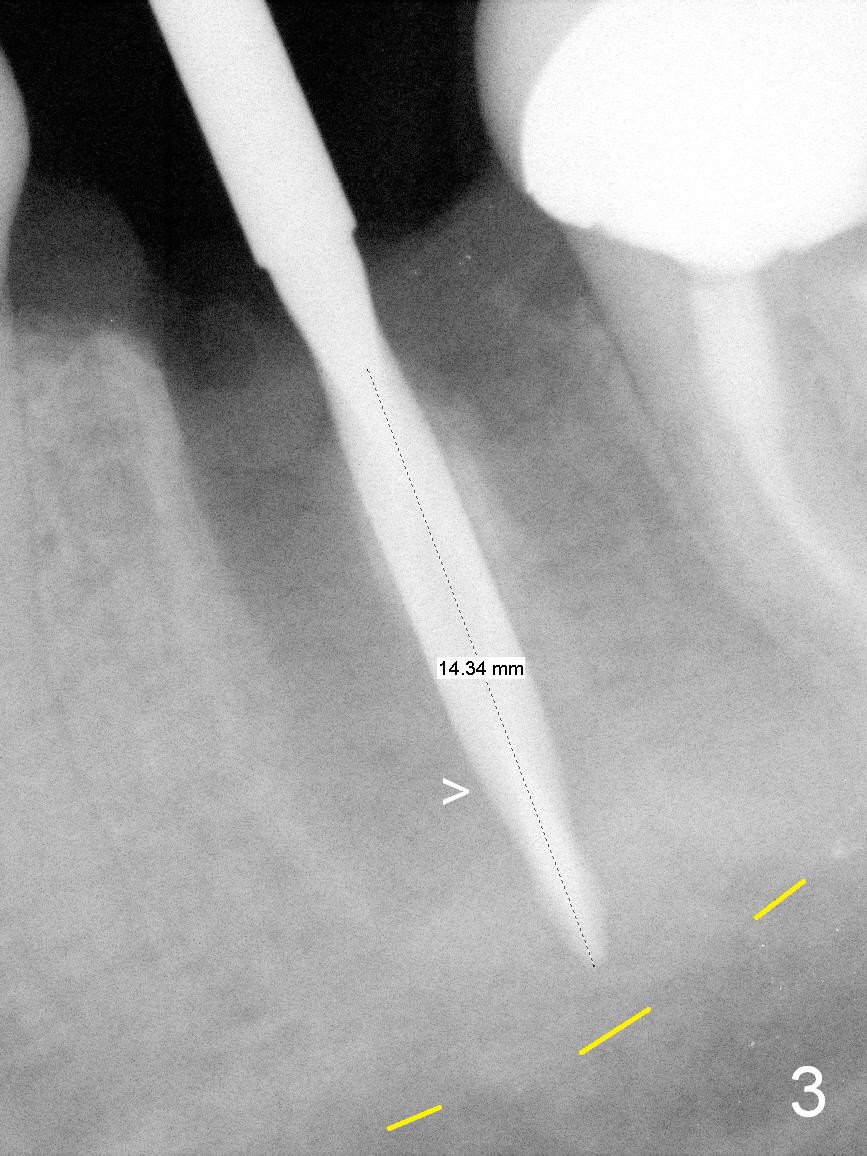
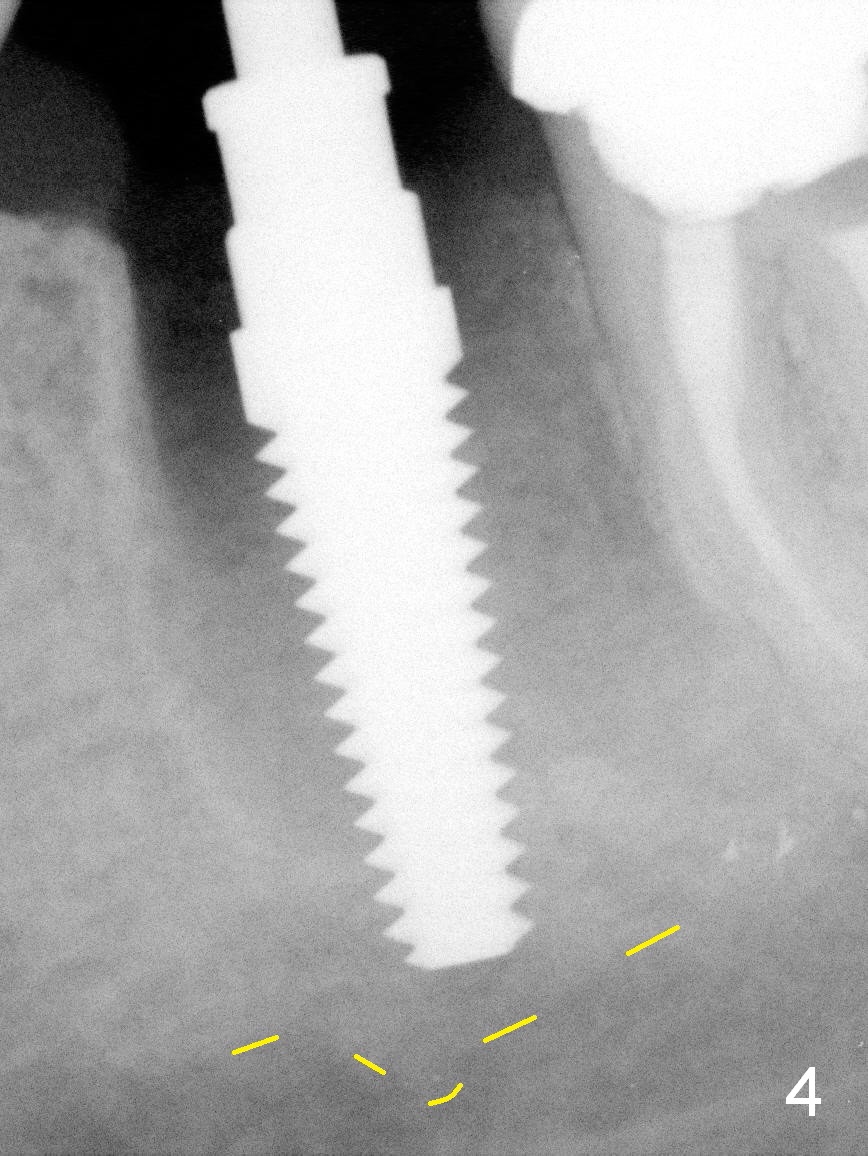
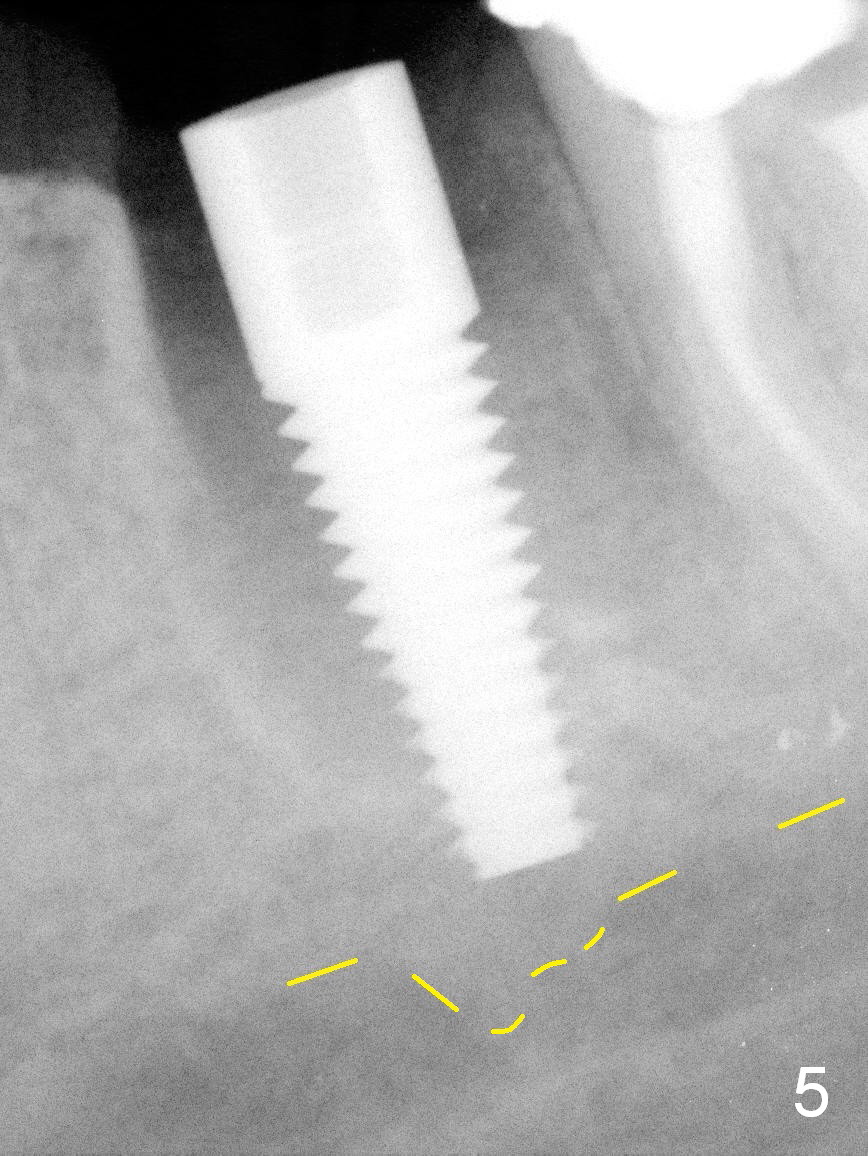
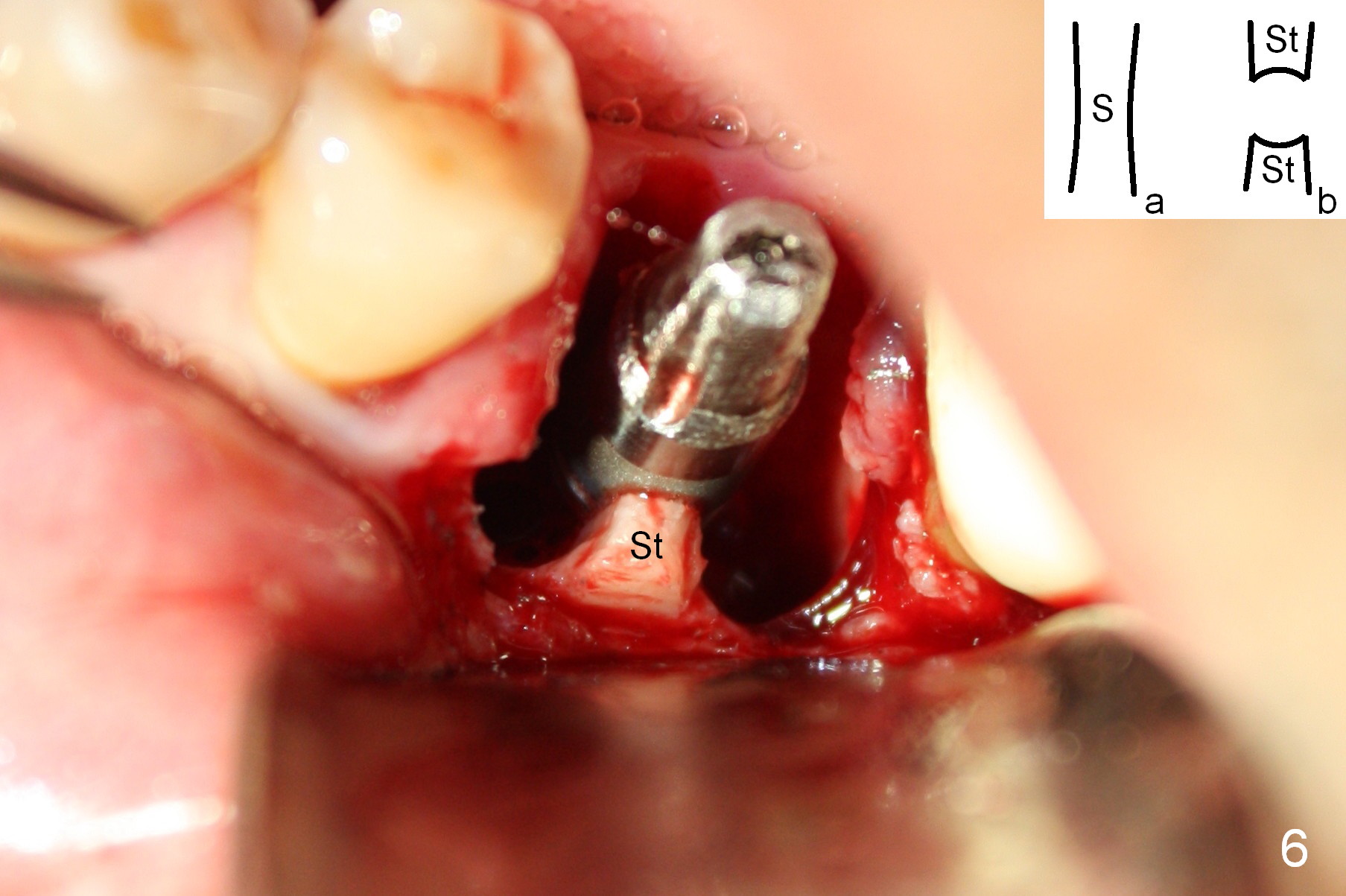
A 42-year-old man requests extraction and implant at the site of #19 (Fig.1). It appears that the site can hold a 6x20 mm tissue-level implant (Fig.2). The extraction turns out to be extremely difficult and time-consuming, but the bright side is that the bone is dense. The most reliable landmark for osteotomy depth is the septal crest; when a 2 mm pilot drill is used in the middle of the septum (S in Fig.6 (insert a)) at 14 mm, it is close to the Inferior Alveolar Canal (Fig.3 yellow dashed line). In fact the apical mesial wall of the septum is perforated (Fig.3 >). While the depth of the osteotomy is tightly controlled, the osteotomy is enlarged using reamers 2.5-4 mm until the mesial and distal surfaces of the septum are completely perforated (Fig.6 insert b). When a 5x17 mm tap is inserted (Fig.4), it is stable. A 5x17 mm implant is placed with high insertion torque (Fig.5,6). Primary stability appears to be derived from apical new bone (Fig.5) and the septal struts (Fig.6 St). When bone density is high, the septal struts may provide enough stability. There appears no need to obtain apical new bone, which may damage the Inferior Alveolar Nerve.
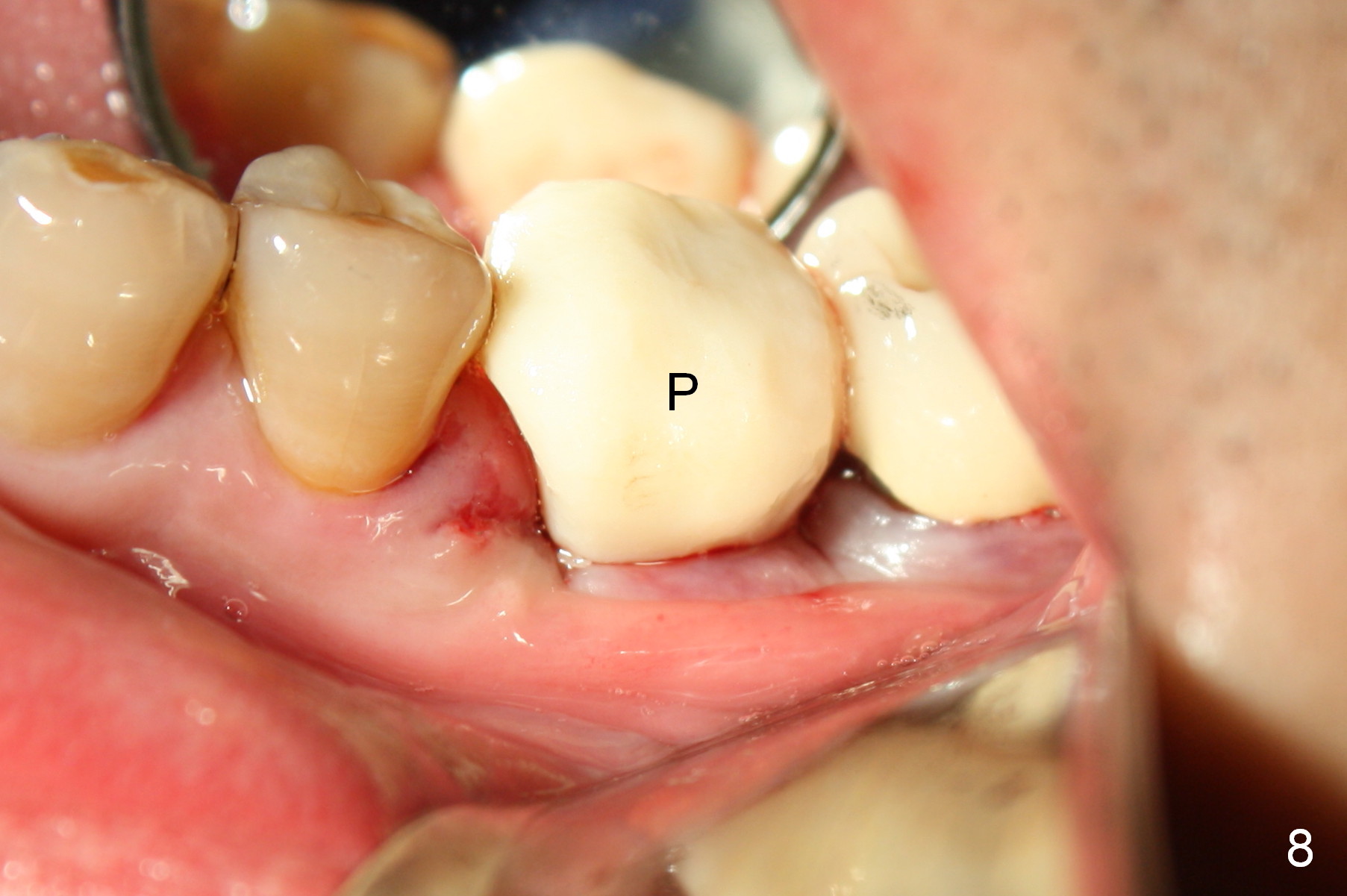
The remaining sockets are bone grafted (Fig.7 G); an abutment (A) is placed for fabrication of an immediate provisional (Fig.8 P). The socket opening is closed with the help of sutures near papillae.
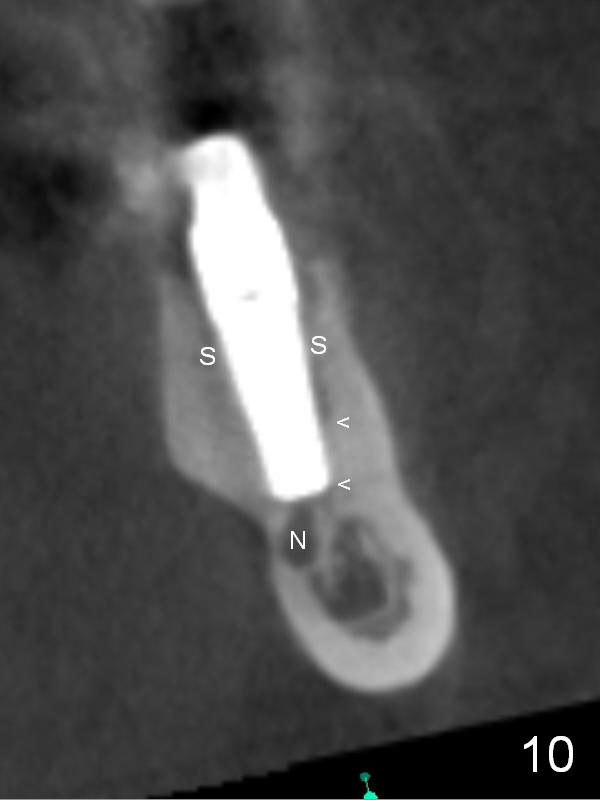
The patient has had pain associated with #15 (without periapical radiolucency (PARL) after root canal therapy and retreatment) and #19 (with PARL after RCT; Fig.1). There is percussion: none with #15, mild with #19. Pain is referred to the temple sometimes. The implant and osteotomy are close to IAN (Fig.3-5). Postop there is no anesthesia, but the patient has the same patterns of pain, a little worse than preop. He has to take Motrin often to control pain. After taking Medrol dose pak and Norco, the pain associated with #19 implant is basically nonexistent, whereas that with #15 is persistent. The patient requests #15 extraction. CT taken 3 weeks postop reveals that the osteotomy and implant may invade the upper border of the Inferior Alveolar Canal (Fig.9, 10). Considering high torque value associated with the 5x17 mm implant, a 5x14 mm implant should be stable, depending mainly upon the engagement into the septal struts.
If extraction of #15 does not improve pain, the implant at #19 will be backed up.
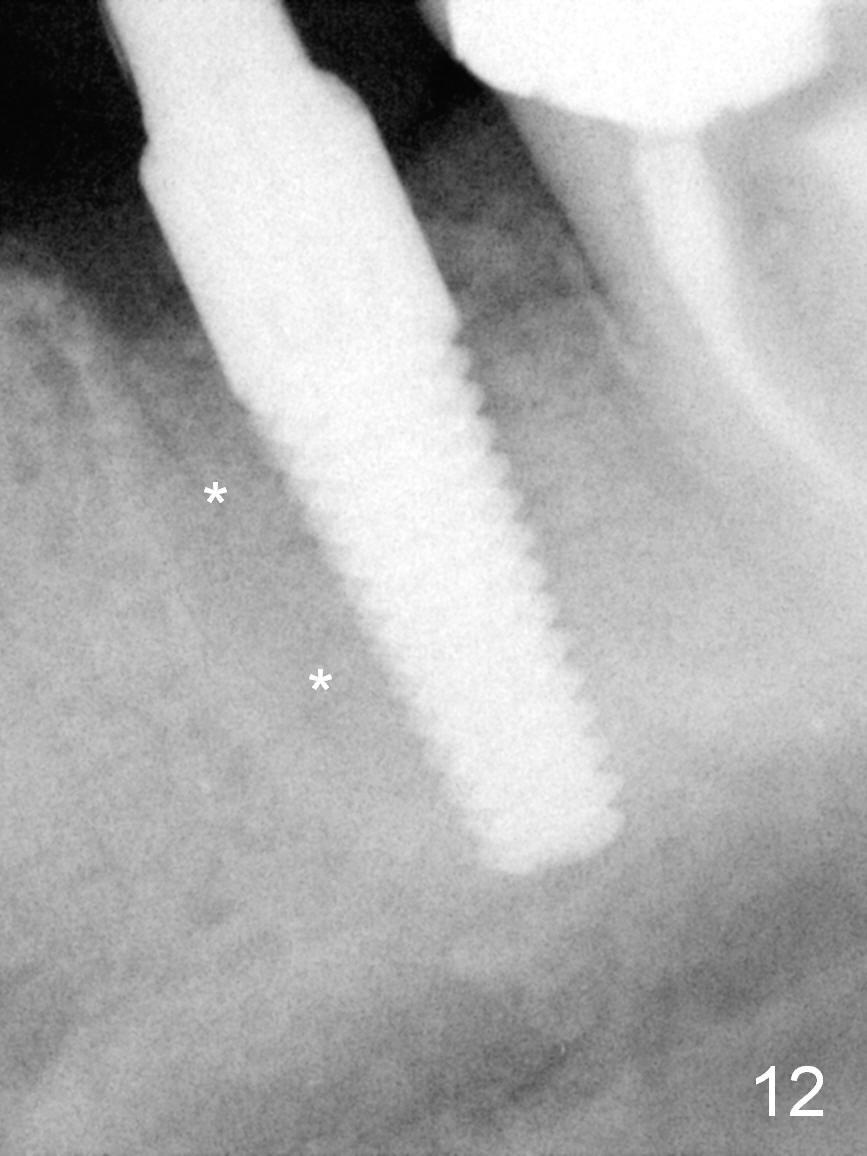
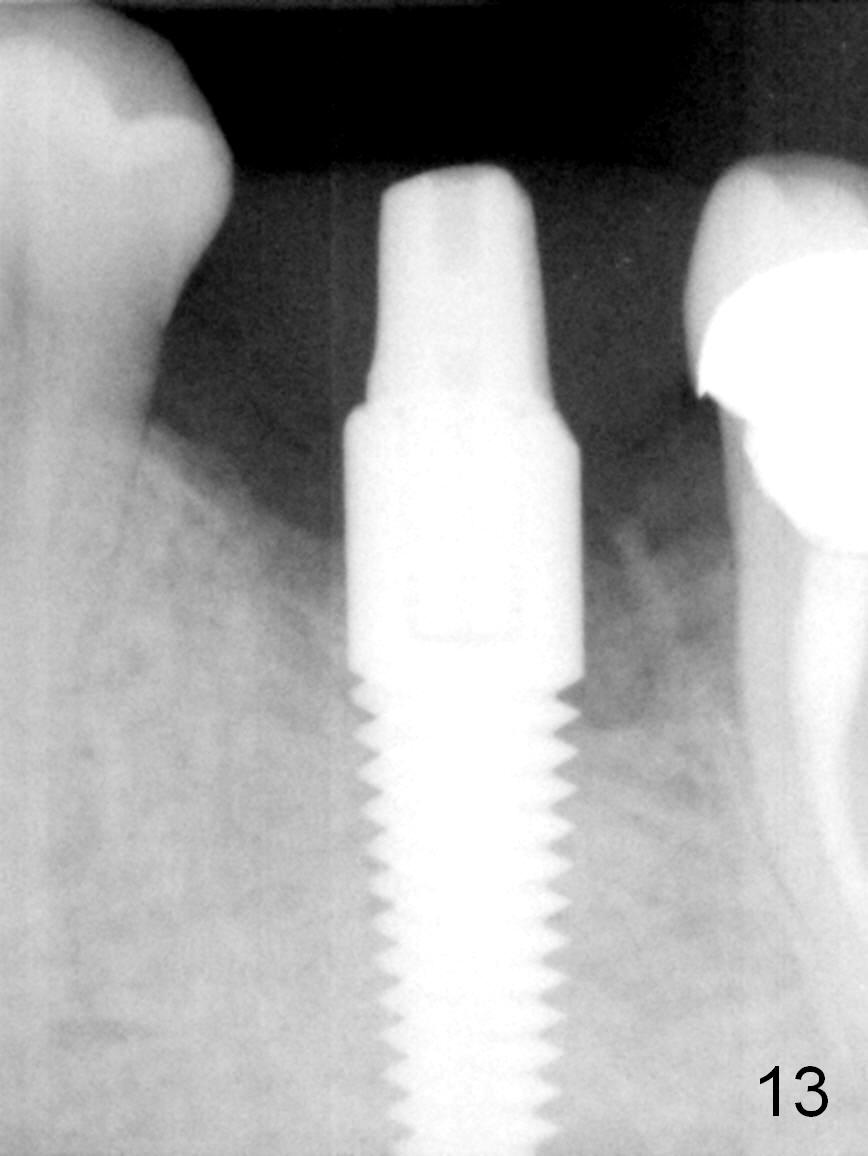
In fact the two procedures were done at the same day (less than 1 month post placement). The implant at the site of #19 was backed up ~ 90 degrees. It became loose. Anyway, the abutment was placed with the immediate provisional. Two months the implant is stable without symptom; the socket density appears to have increased (Fig.12). It appears that the provisional helps keep the implant in place. The socket appears to have healed with formation of bony trabeculae 15 months postop (Fig.13).
Return to Lower Molar Immediate Implant
Posterior Immediate Provisional
Xin Wei, DDS, PhD, MS 1st edition 04/22/2015, last revision 07/19/2016