
.jpg)


%20mm%20(N),%205.5x7(4).jpg)
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Abnormal Pattern of Bone Loss
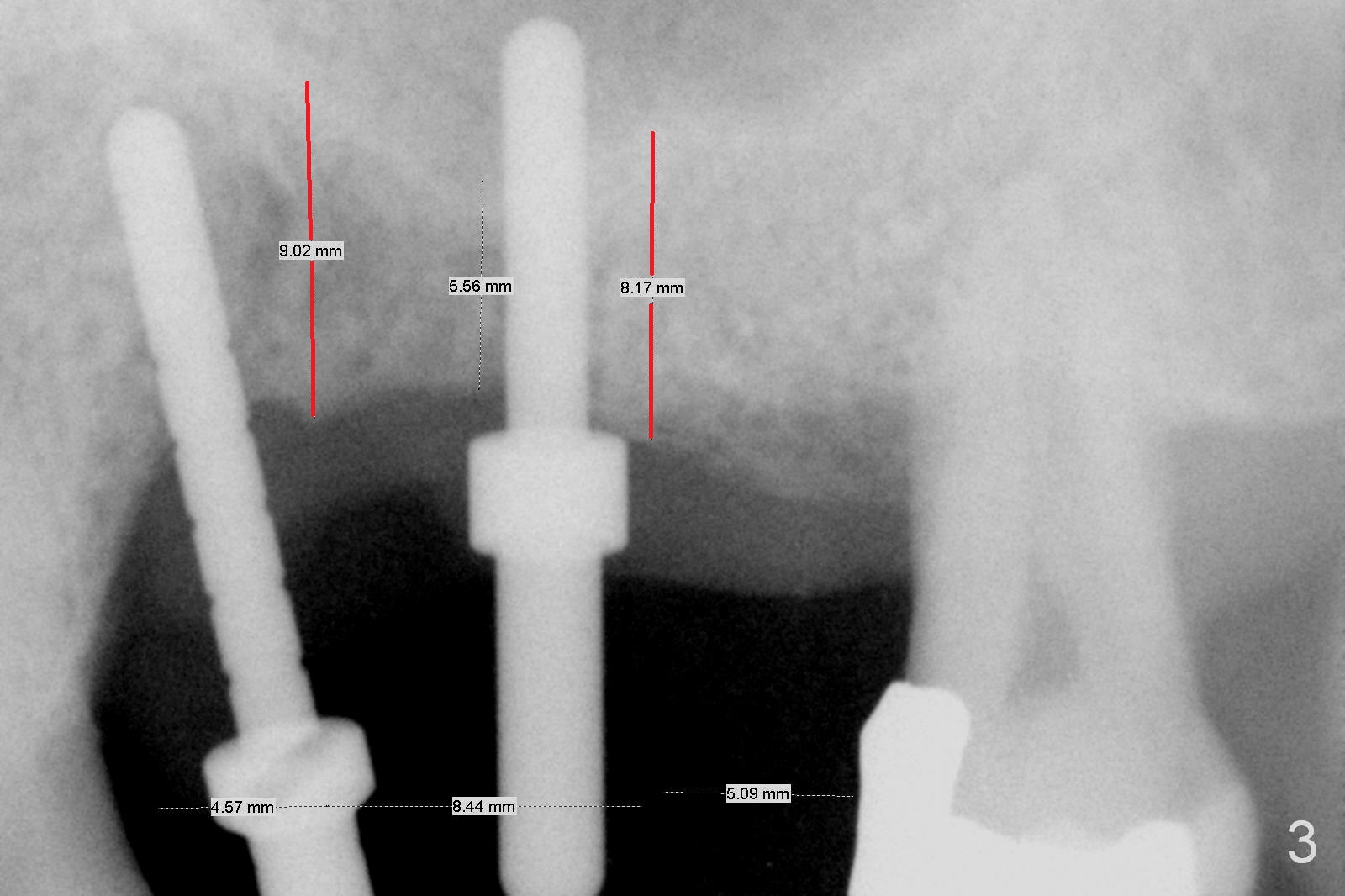
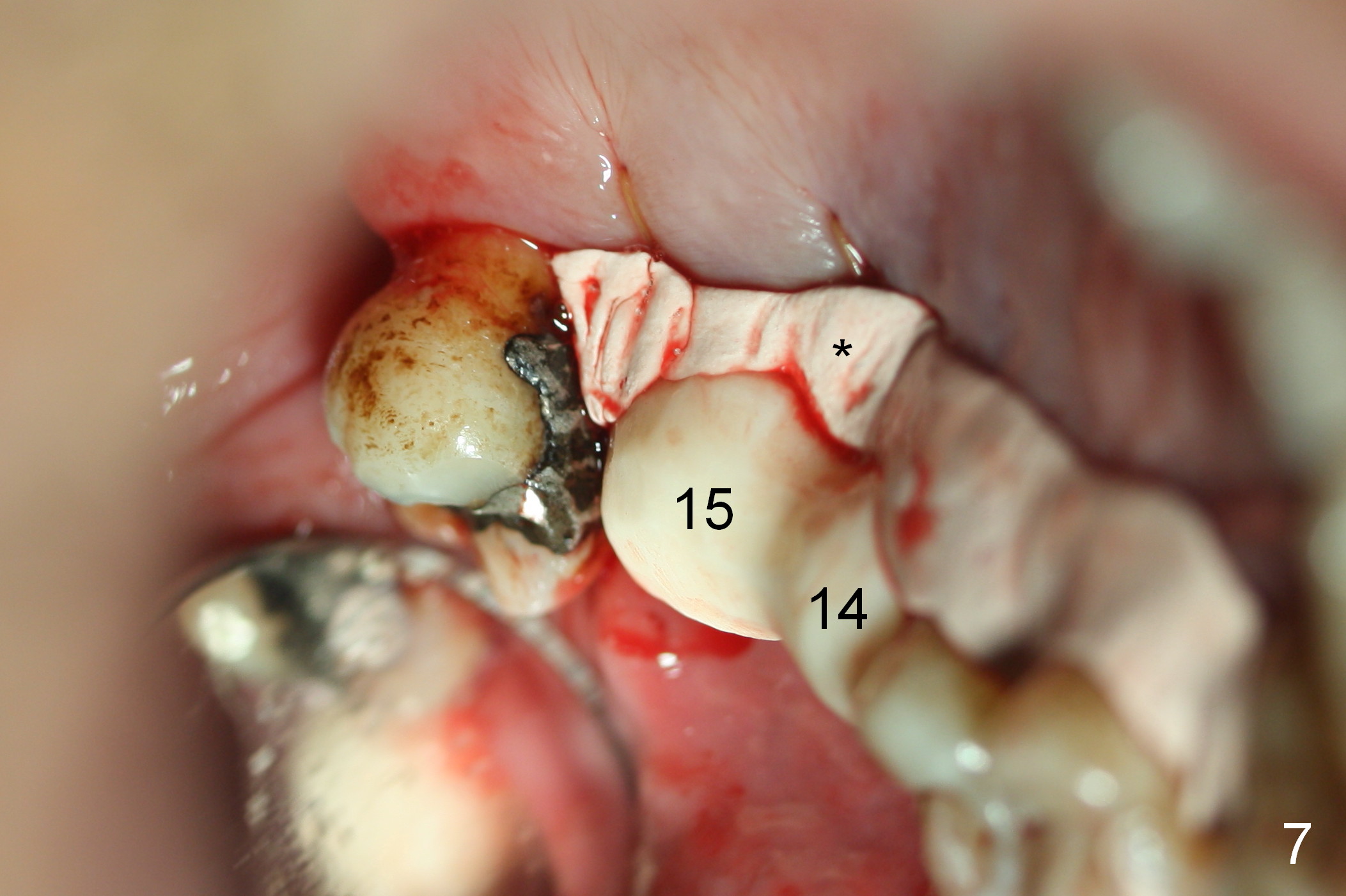
When the tooth #14 is extracted, the socket is almost exclusively covered by the gingiva (Fig.1 *). Flap is needed for implant placement at #14 and 15. The buccopalatal width at #14 is narrow. The position and trajectory of initial osteotomy (Fig.2,3) is going to be changed, as indicated by red lines in Fig.3. The implants at #14 and 15 are 4.1x12 (SM) and 6x6 mm (UF) (Fig.4 >50 Ncm). The latter is later placed higher (Fig.5 >). In fact sinus lift is accomplished. Abutments are placed immediately (4.8x7(4.5) and 6.5x5(5) mm) (Fig.4-6) for immediate splinted provisional (Fig.7 (palatal view)). The remaining wound is further protected with periodontal dressing (Fig.7 *). The 3rd molar is intentionally not extracted for added retention for the provisional and periodontal dressing. Fig.8 is taken 2.5 months postop.
The patient returns for final restoration 7 months postop. An angled abutment (3.9x15° A (4) mm) is placed at #14 so that impression material (light body) easily flows into the mesial margin (Fig.9 arrow) following laser gingivectomy (*, as compared to Fig.8). The abutment at #15 has to be changed with longer abutment height and shorter cuff (5.5x7(4) mm) because of severe pre-existing bone loss. The implant at #15 should have been placed deeper.
Return to Upper Molar Immediate Implant,
Posterior Immediate Provisional,
Systemic Diseases
Xin Wei, DDS, PhD, MS 1st edition 10/31/2015, last revision 01/19/2018