



|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
When Not to Place Immediate Implant?
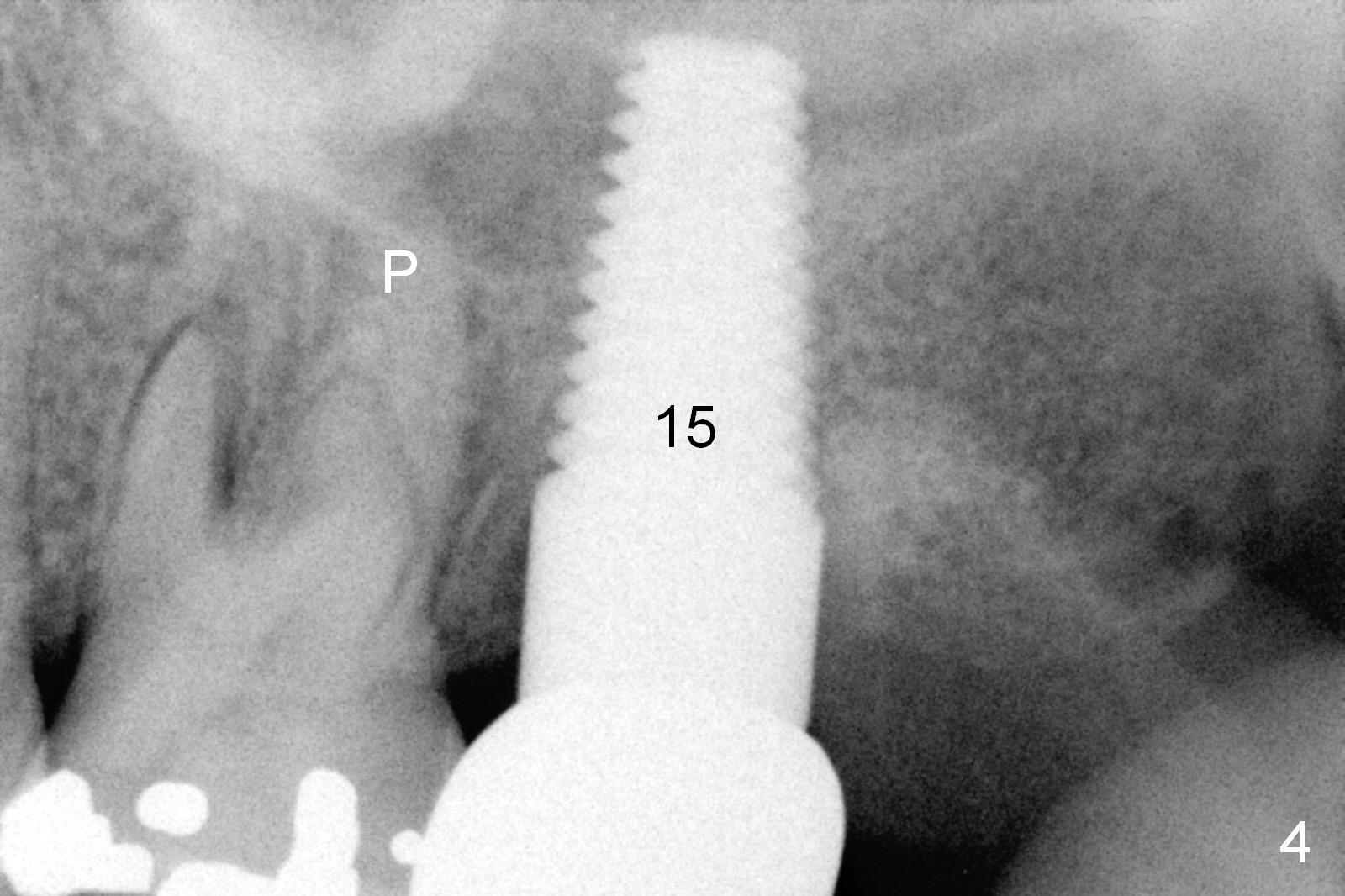
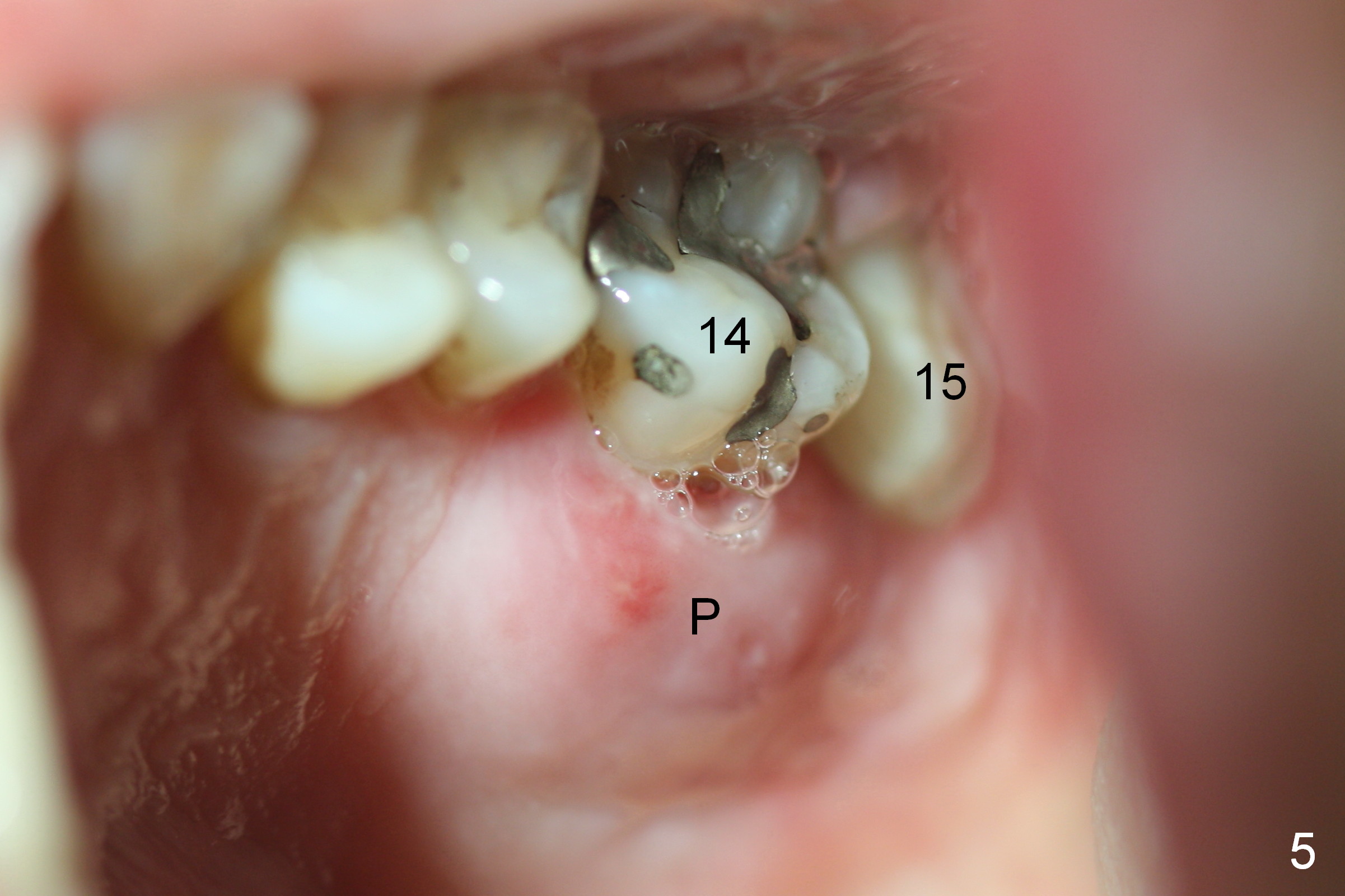
A 48-year-old lady has 4 relative contraindications to immediate implant: 1. infection is so severe at the site of #14 (the posterior maxilla with low bone density, Fig.4,5) that there is no enough bone to support the implant (Fig.7 illustration (1, 2); 2. dental insurance runs out; 3. she shows late in the afternoon when there is not enough staff; 4. she has had 2 immediate implants placed (Fig.4: #15 (3,4)). After socket preservation (Fig.8,9), she is most likely to return for implant placement.
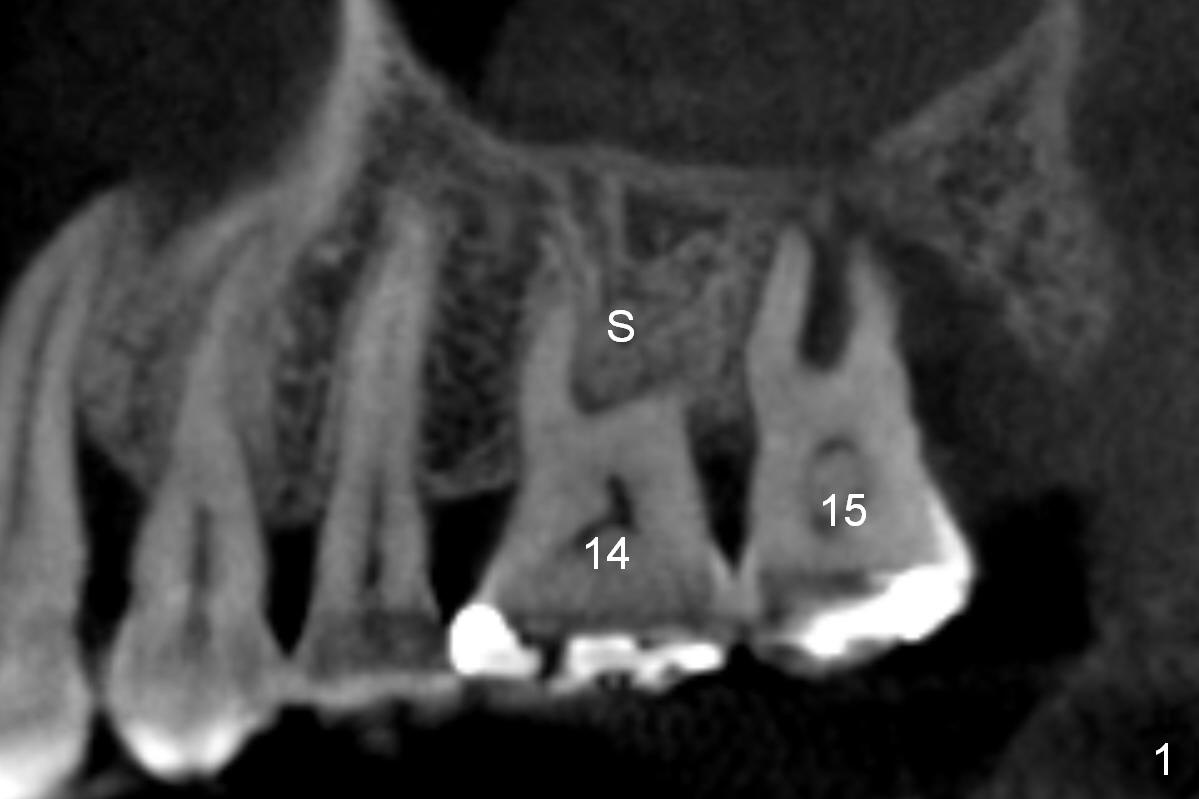
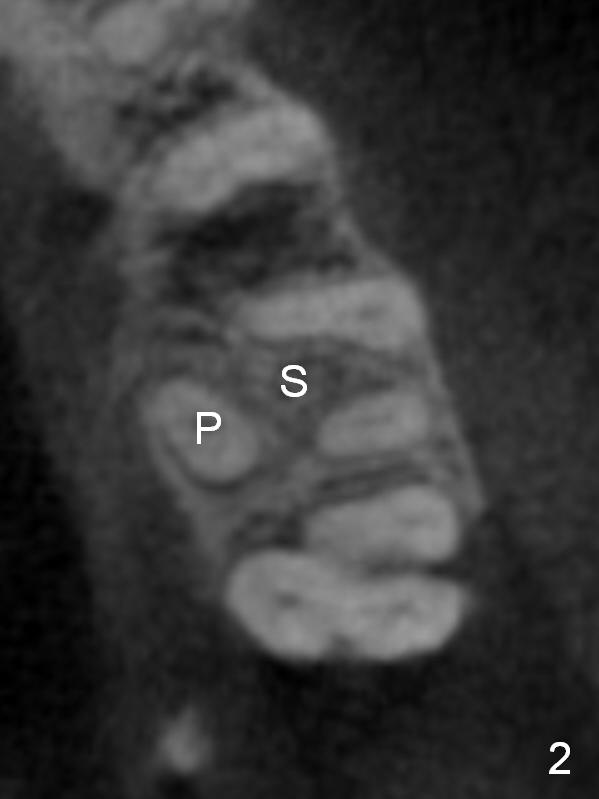
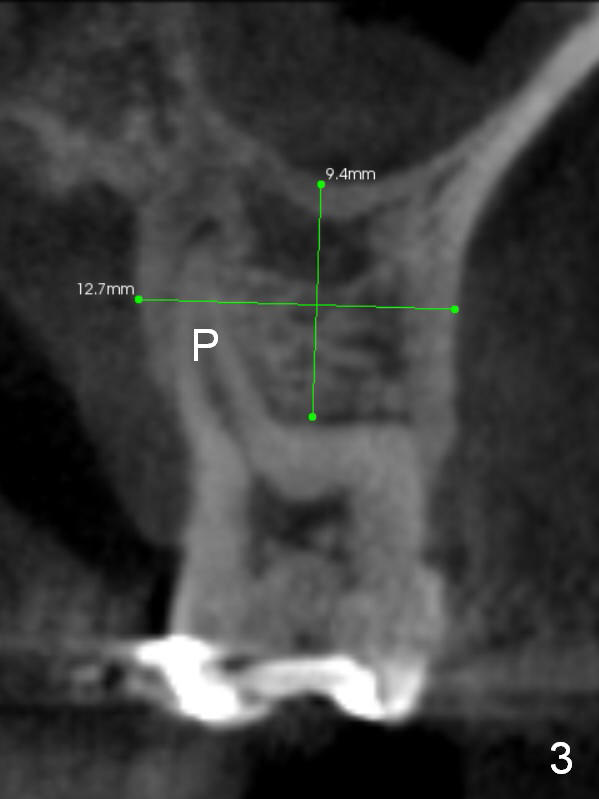
It is noteworthy that the tooth #14 was less affected than #15 22 months earlier (Fig.1 (CBCT sagittal section), 2 (axial), 3 (coronal)). Calculus on the surface of the palatal root (Fig.6 P) is associated with the palatal abscess (Fig.5 P). S: septum.
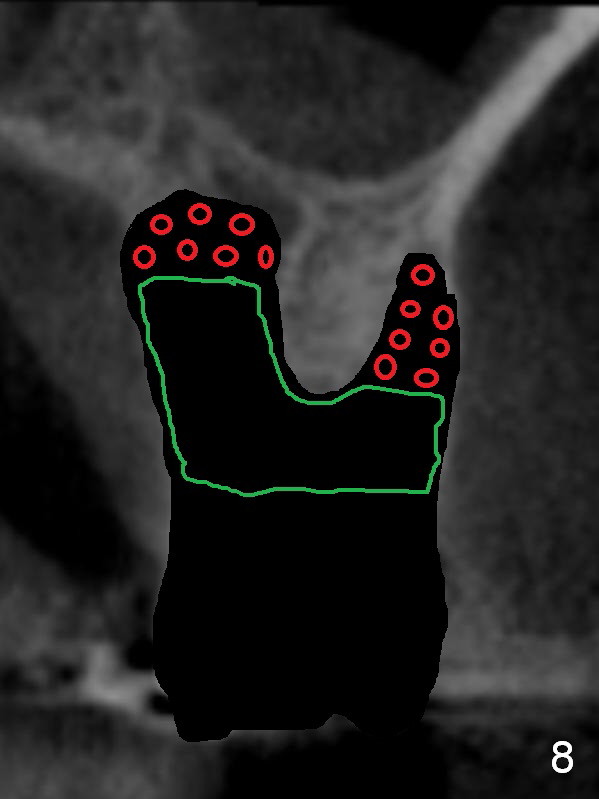
Serrated curette is used to remove granulation tissue mainly from large palatal socket, followed by copious irrigation, and placement of Clindamycin gauze x2 in the sockets. There is apical perforation of the MB socket. In the deep portion of each socket placed is ~.03 CANCELL Oss (Mineralized Cancellous Human Allograft, distributed by Impladent LTD, .850-1 mm, 03-0494763, Product Code 06412201) and equal amount of Osteogen into socket (Fig.8 red circles), covered with Osteogen plug (20x10 mm, Fig.8 green outline). The latter is fixed in placed by 4-0 Chromic gut suture (figure-8, Fig.9), followed by perio dressing, 2x2 gauze, hemastatic.
The socket preservation of this case is assisted by Ms. Suniti Tripathi until evening. With her heart and wisdom, I feel that I could provide the best dental care to my patients.
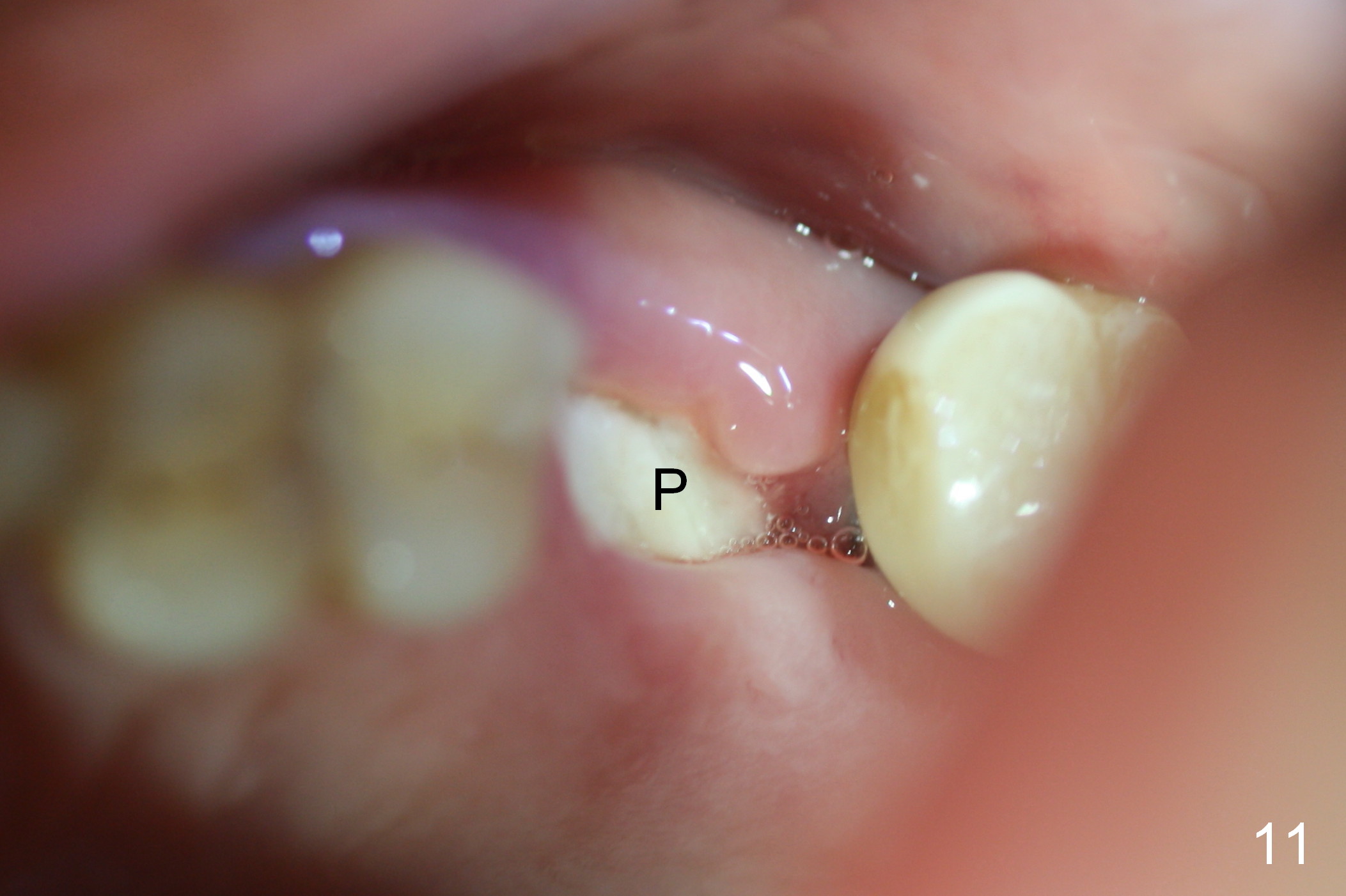
There is no palatal erythema or edema 9 days post extraction (Fig.10 *) with shrinkage of the socket opening. The Osteogen plug remains in place (Fig.11 P). The patient will return for implant placement 6 months post socket preservation.
Return to
Upper Molar Immediate Implant #2,6,
15
Xin Wei, DDS, PhD, MS 1st edition 06/25/2015, last revision 05/28/2018