





|
|
|
|
|||
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
||||
Block Graft at #6/7 or Immediate
Implant at #5
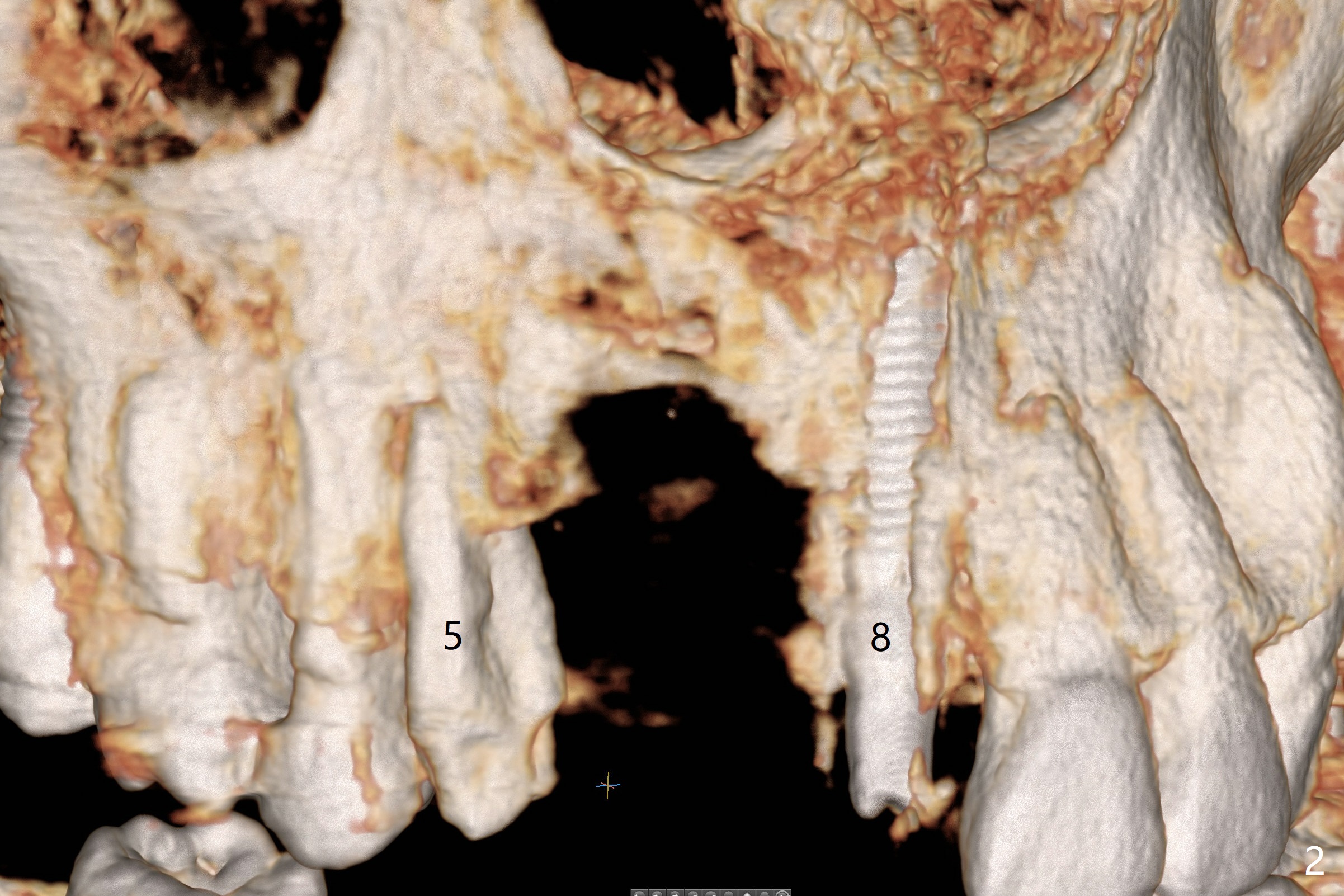
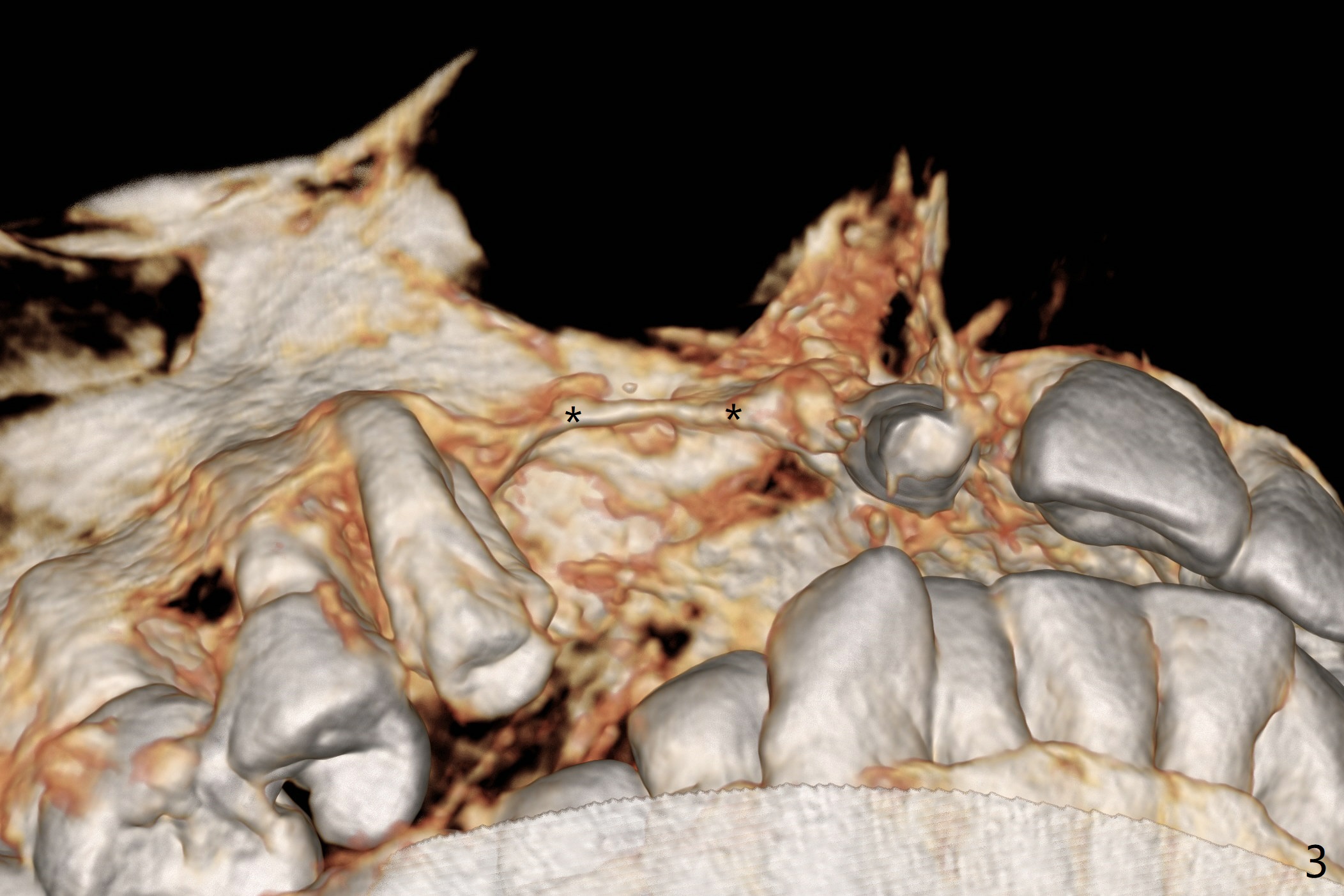
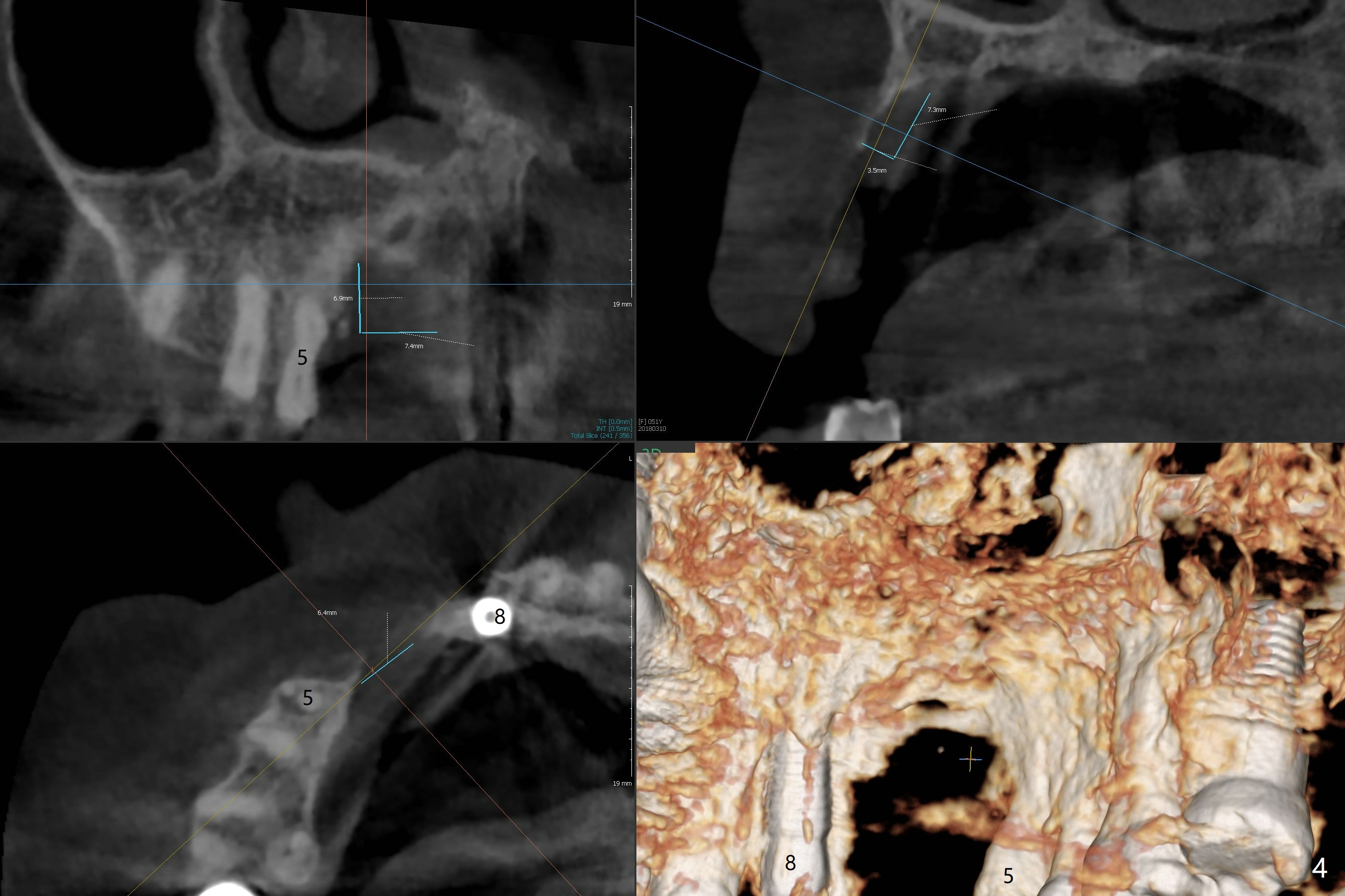
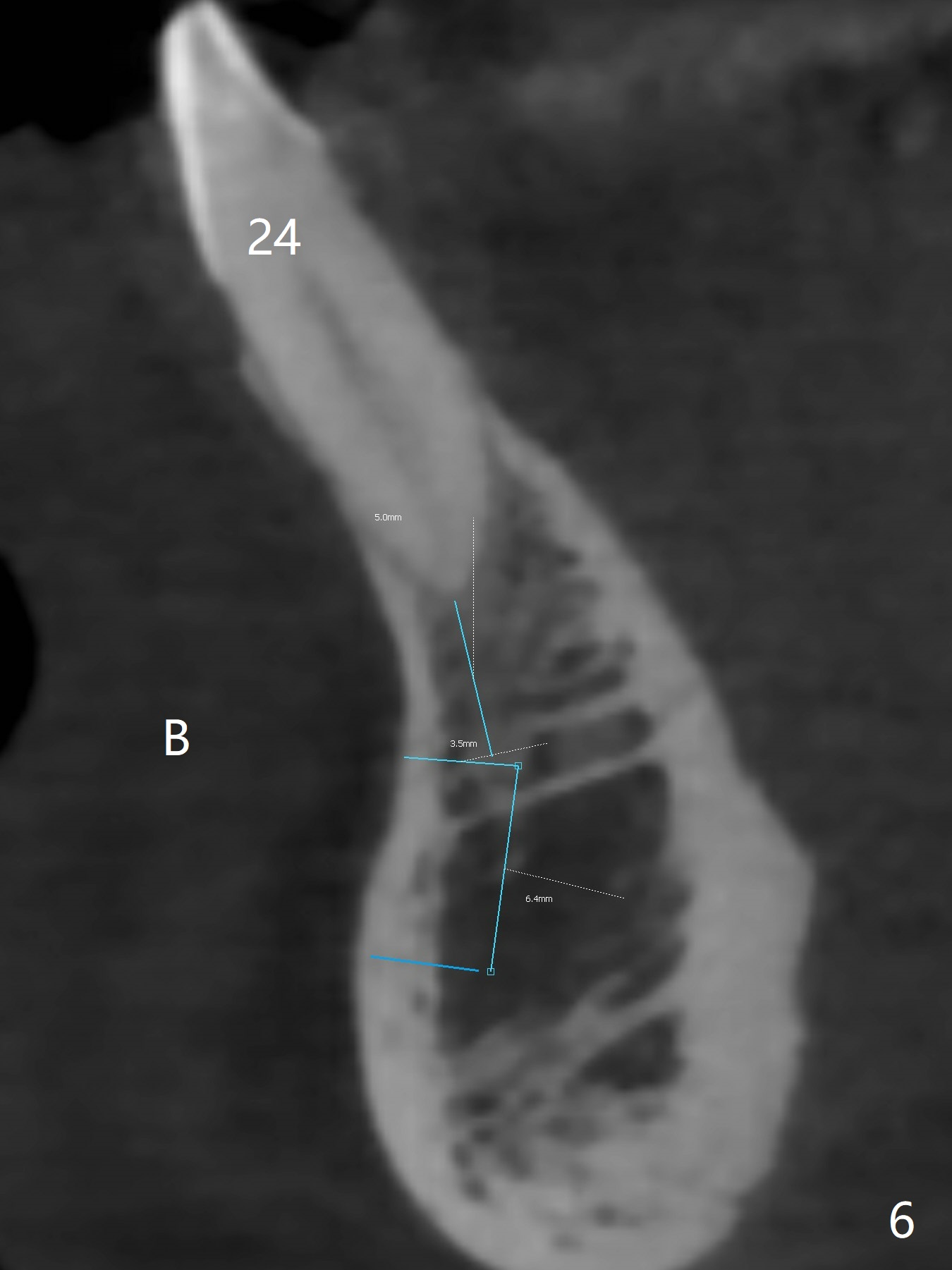
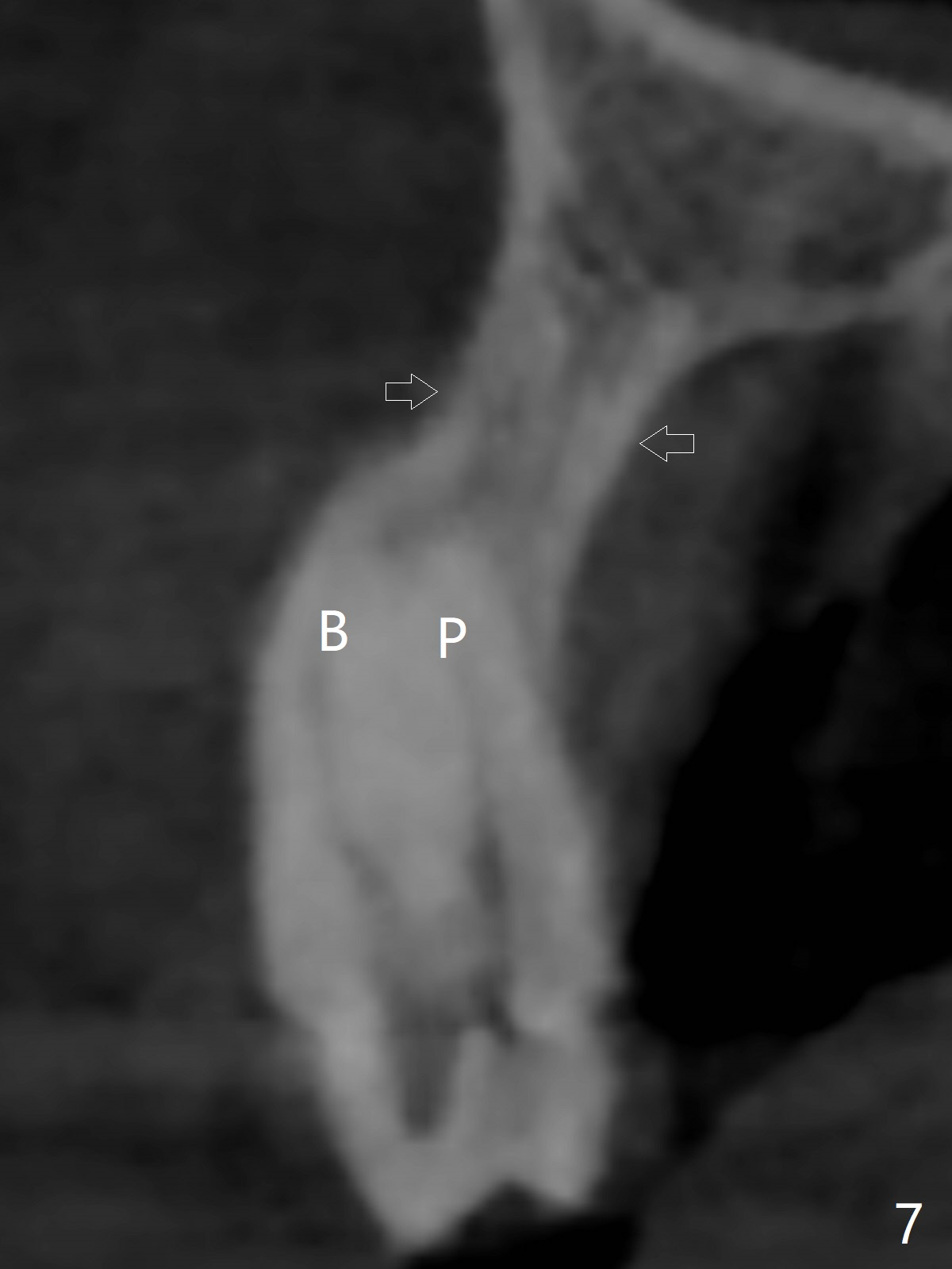
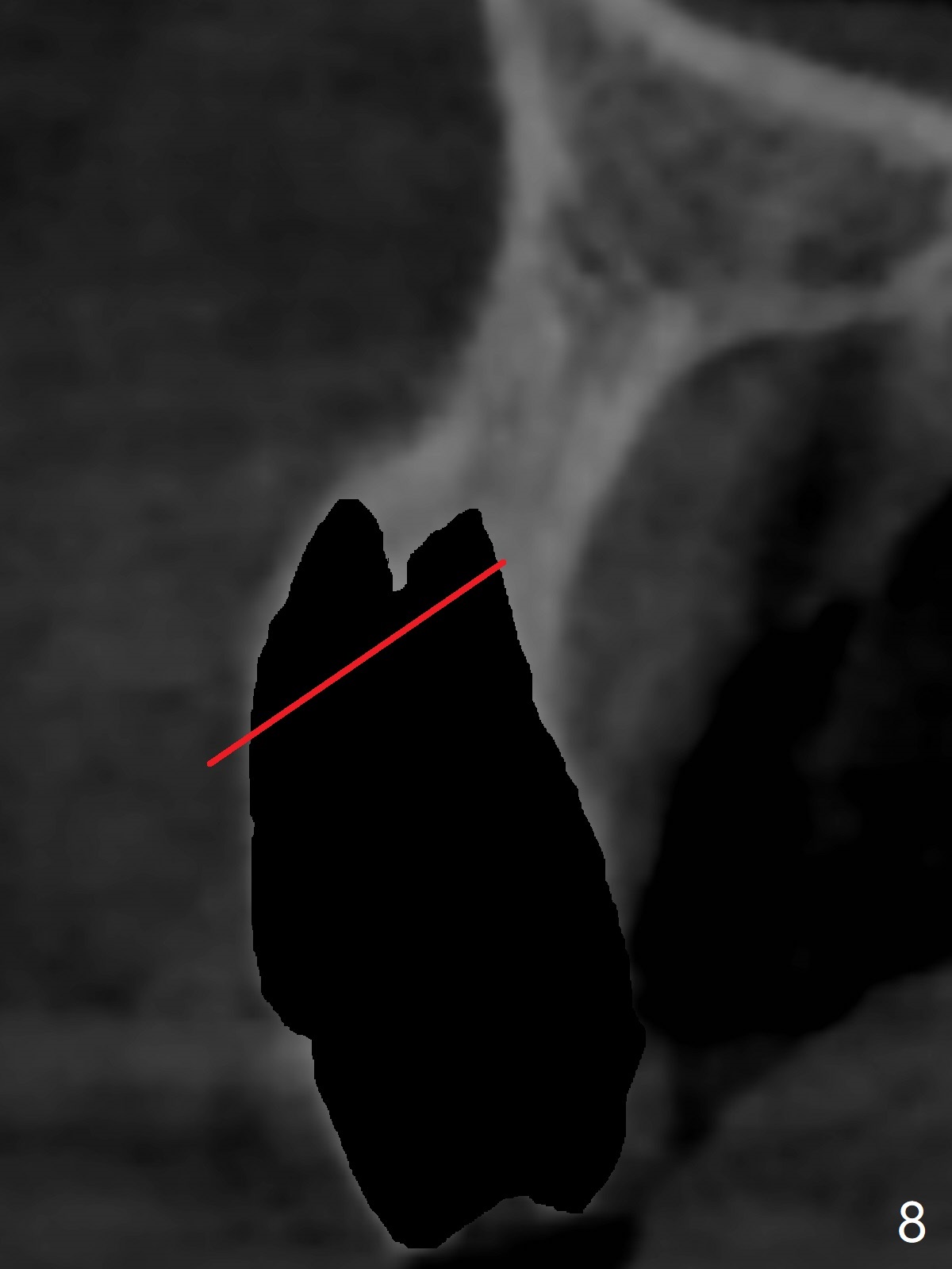
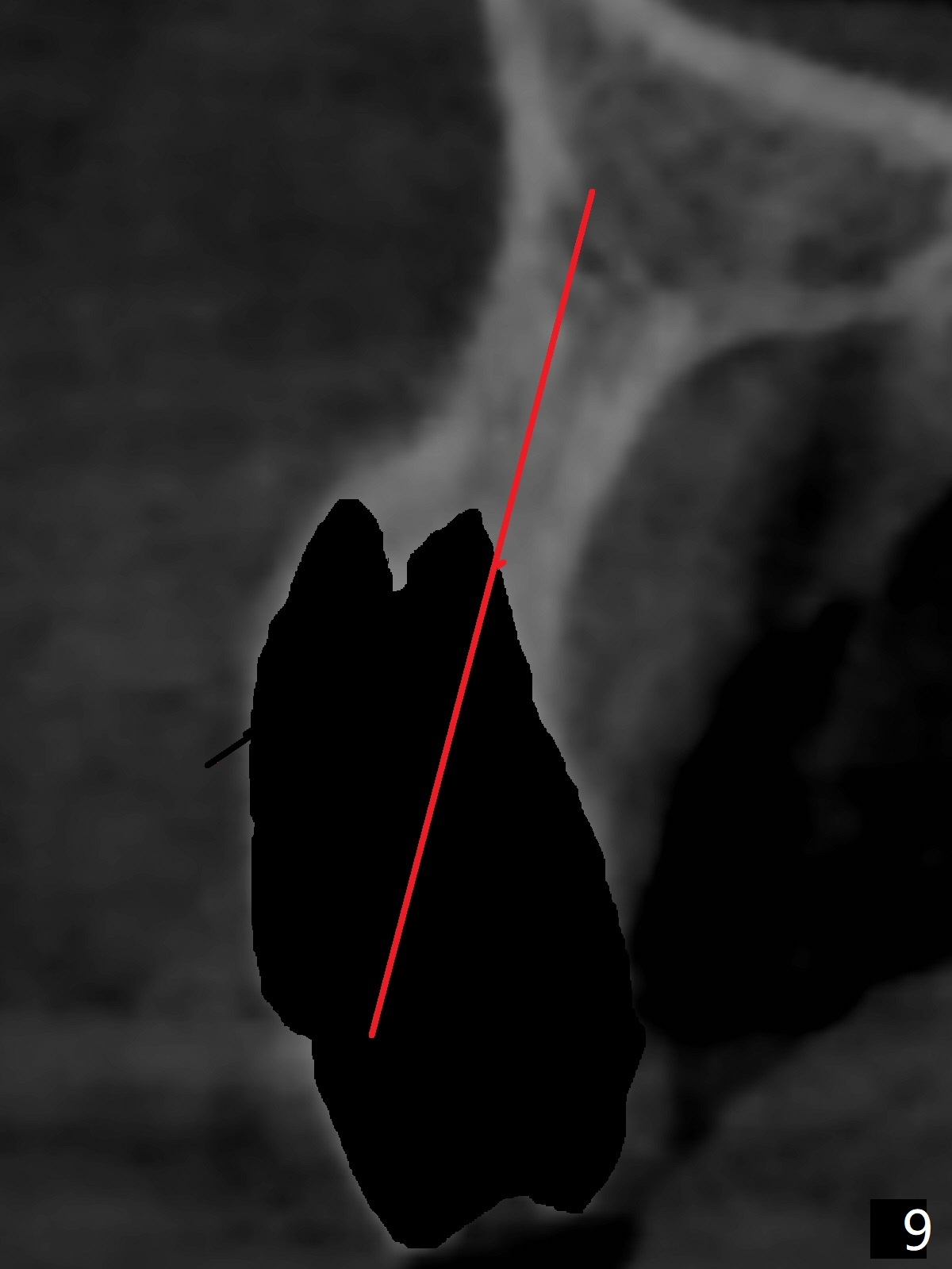
A 51-year-old woman lost the teeth #6 and 7 due to odontoma removal ~30 years ago. The area was restored with a FPD. The latter is removed with immediate implant at #8 8-9 months earlier. Particulate bone graft does not repair the bone deficiency at #6, 7 (Fig.2,3), although the soft tissue looks bulky (Fig.1). It appears that the palatal defect also needs a piece of bone block to fill in (Fig.4). The block will be harvested from the chin (Fig.5,6). If the block graft turns out to be impracticable, the periodontally compromised tooth #5 (bone loss, Fig.2,3,7) will be extracted for immediate implant. Initial osteotomy will be established in the palatal socket (Fig.8,9). Either a 2- (Fig.10) or 1- (Fig.11) piece implant will be placed. After wound healing, impression will be taken for a lab-fabricated provisional FPD.
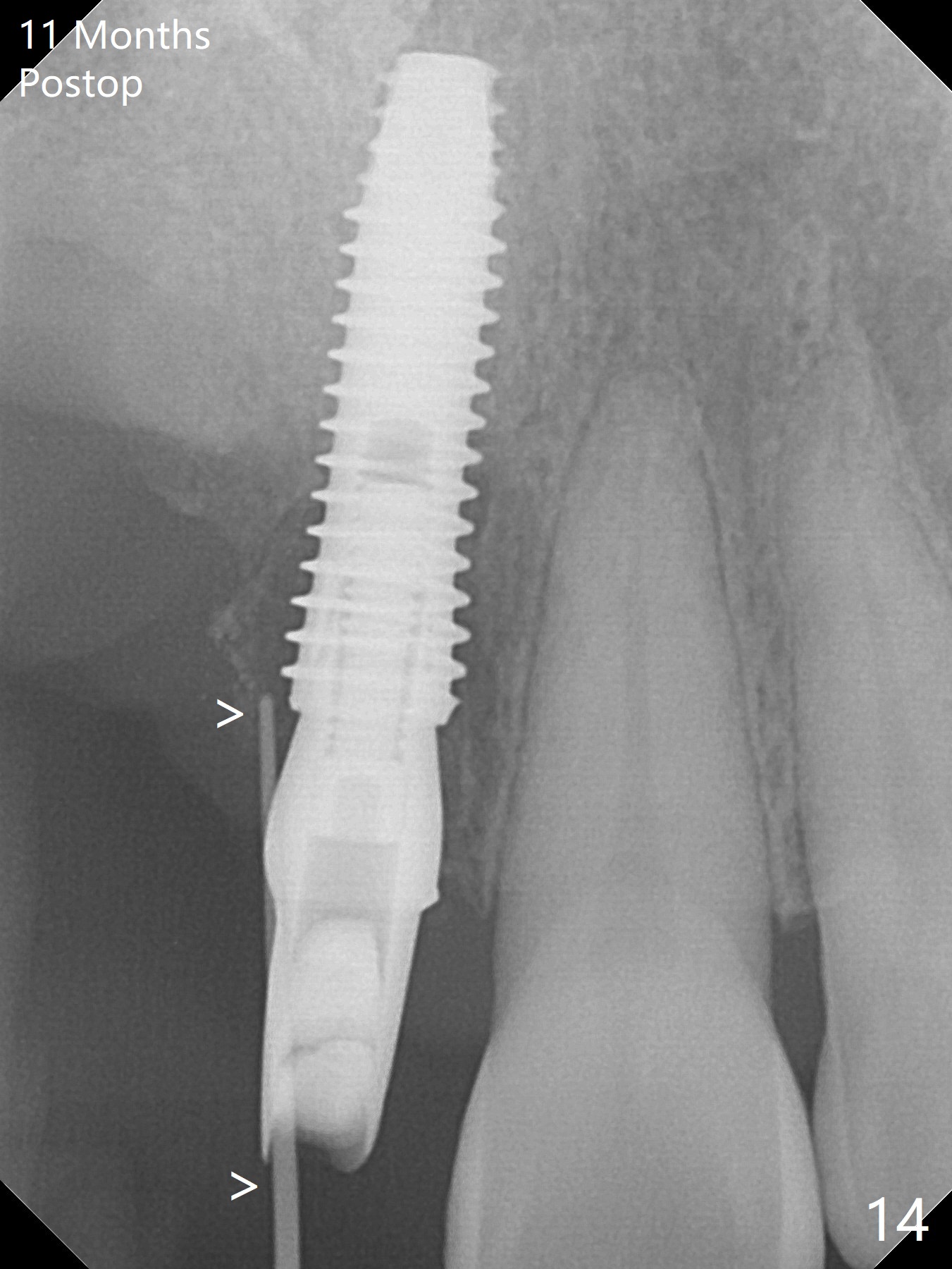
An asymptomatic erythema develops at #8 10 months postop (Fig.12 *). A fistula forms 11 months postop (Fig.13 < ) and is associated with implant thread exposure (Fig. 14 >, as compared to Fig.2). It appears that bone graft and possible block graft are needed with PRF after debridement with Titanium brush.
Return to
Upper
Canine Immediate Implant, Armaments,
Metronidazole, #2,14,15
Xin Wei, DDS, PhD, MS 1st edition 05/28/2018, last revision 07/26/2018