,%20Vanilla.jpg)





|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
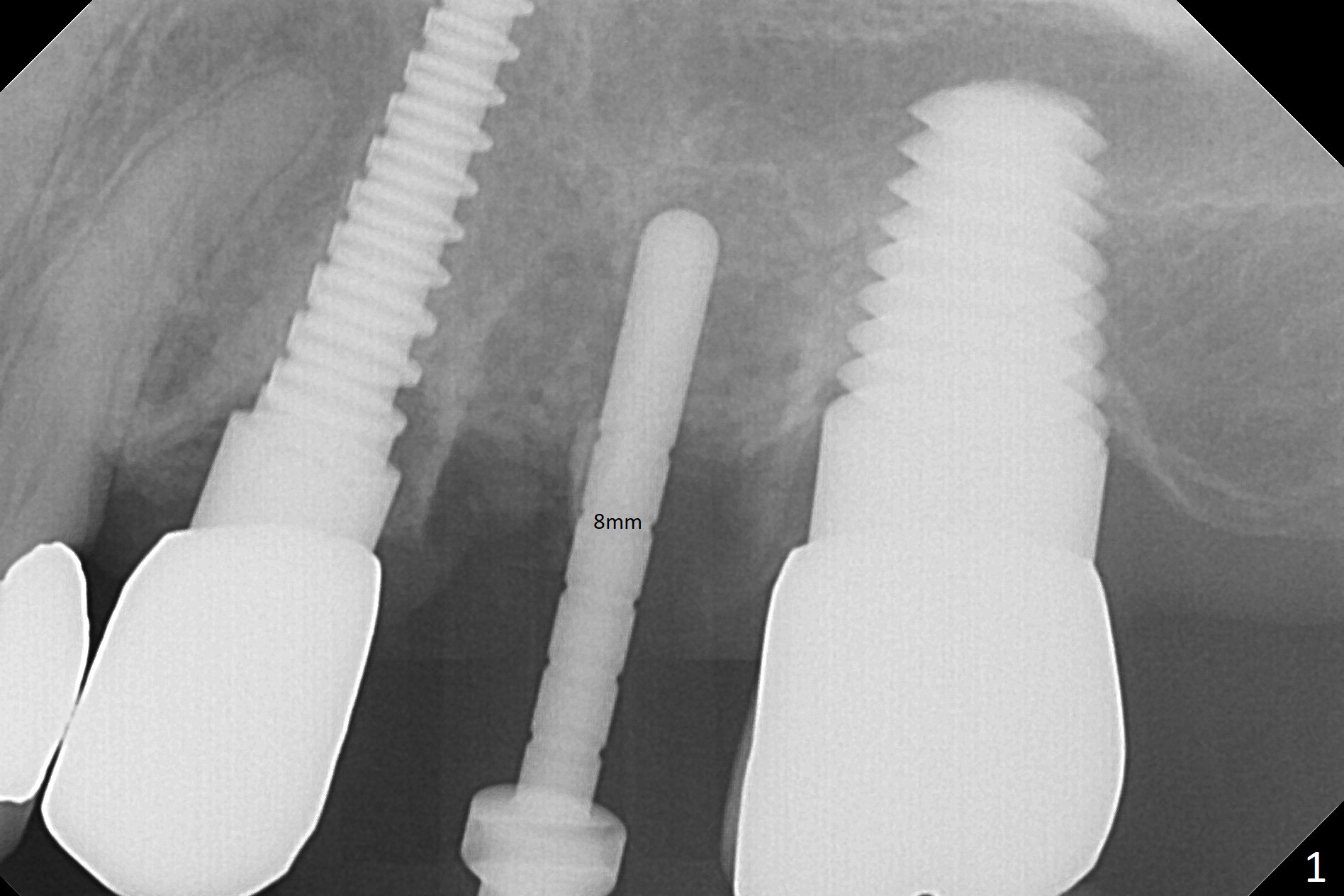
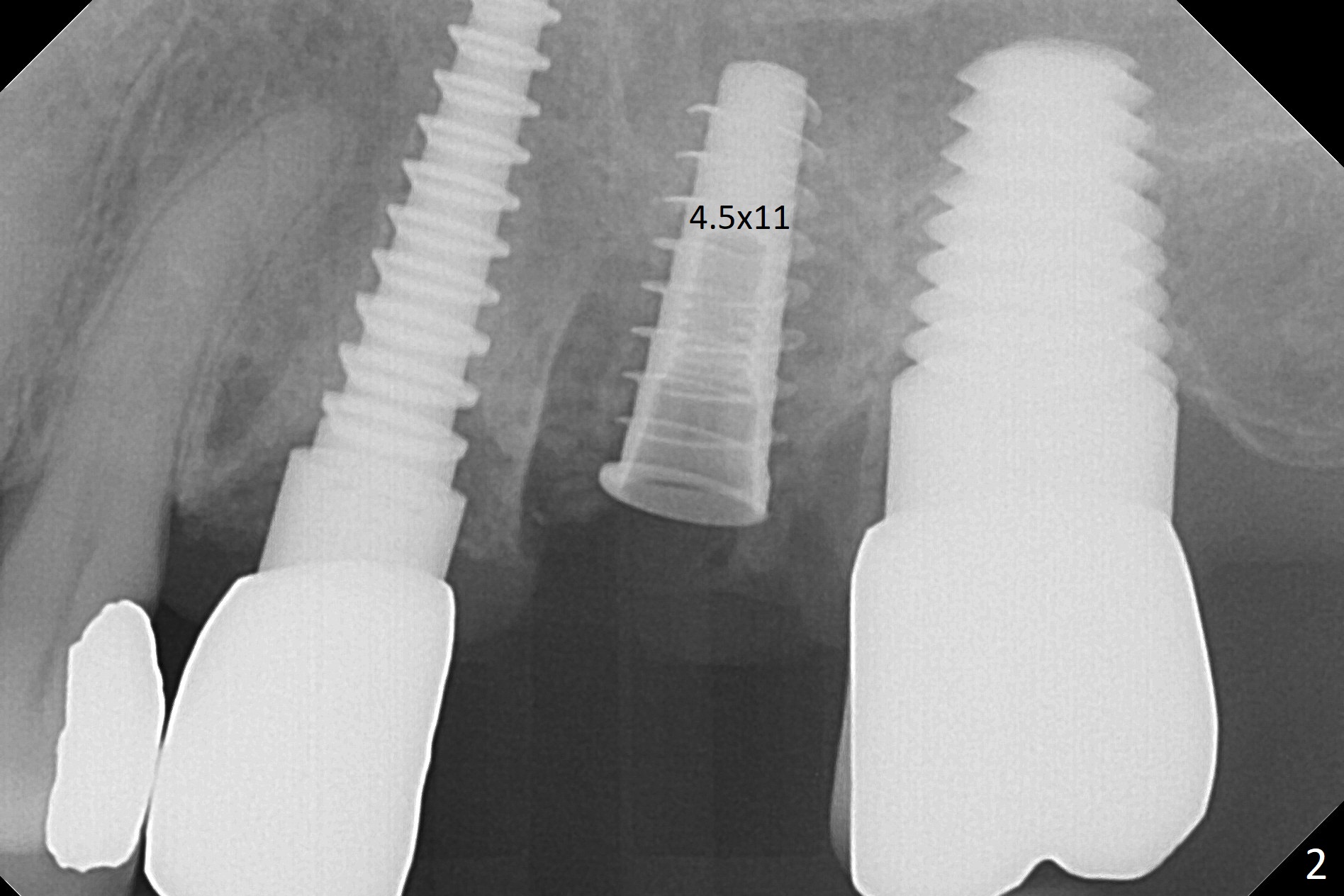
Use Implant for Sinus Lift
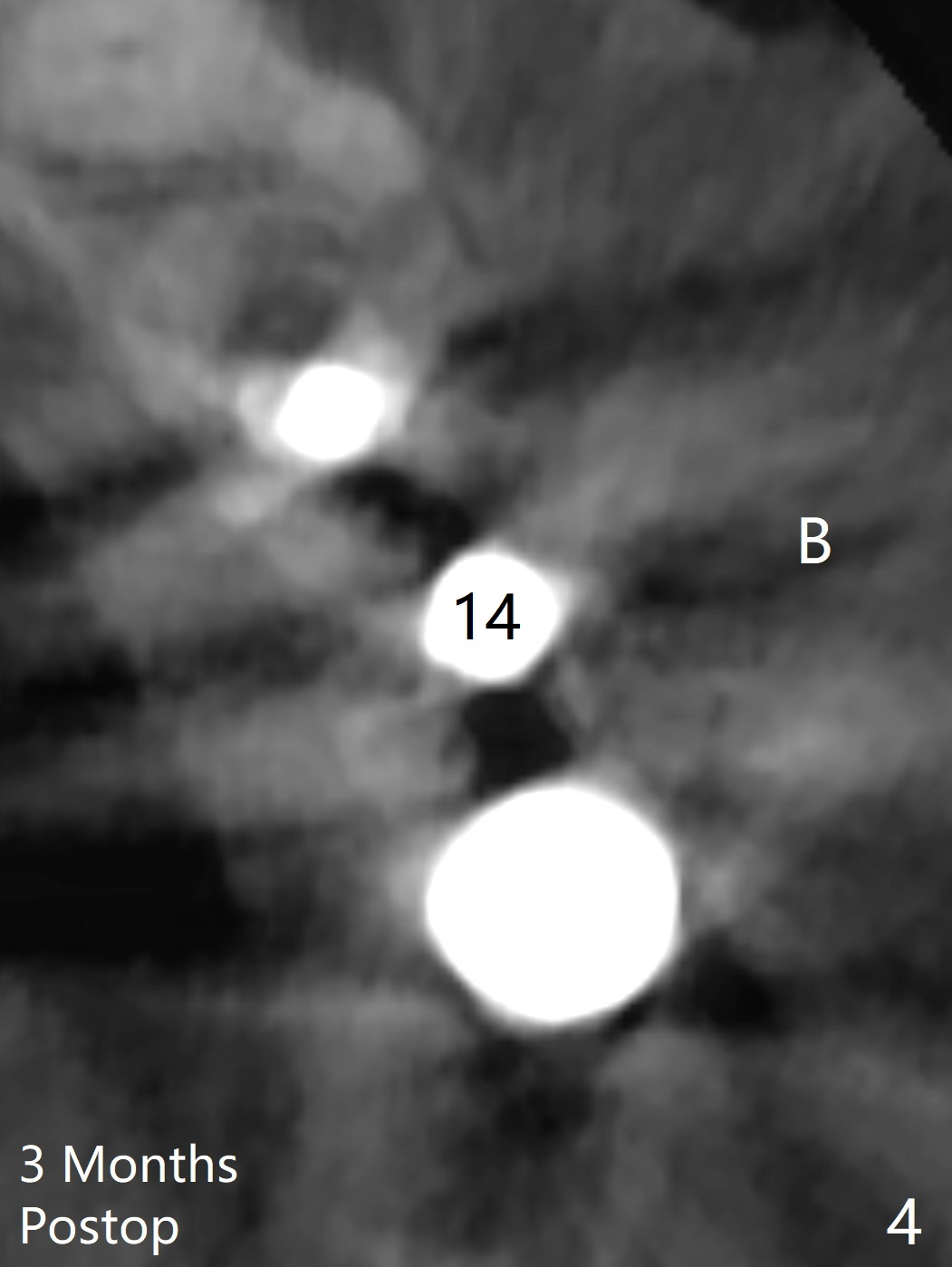
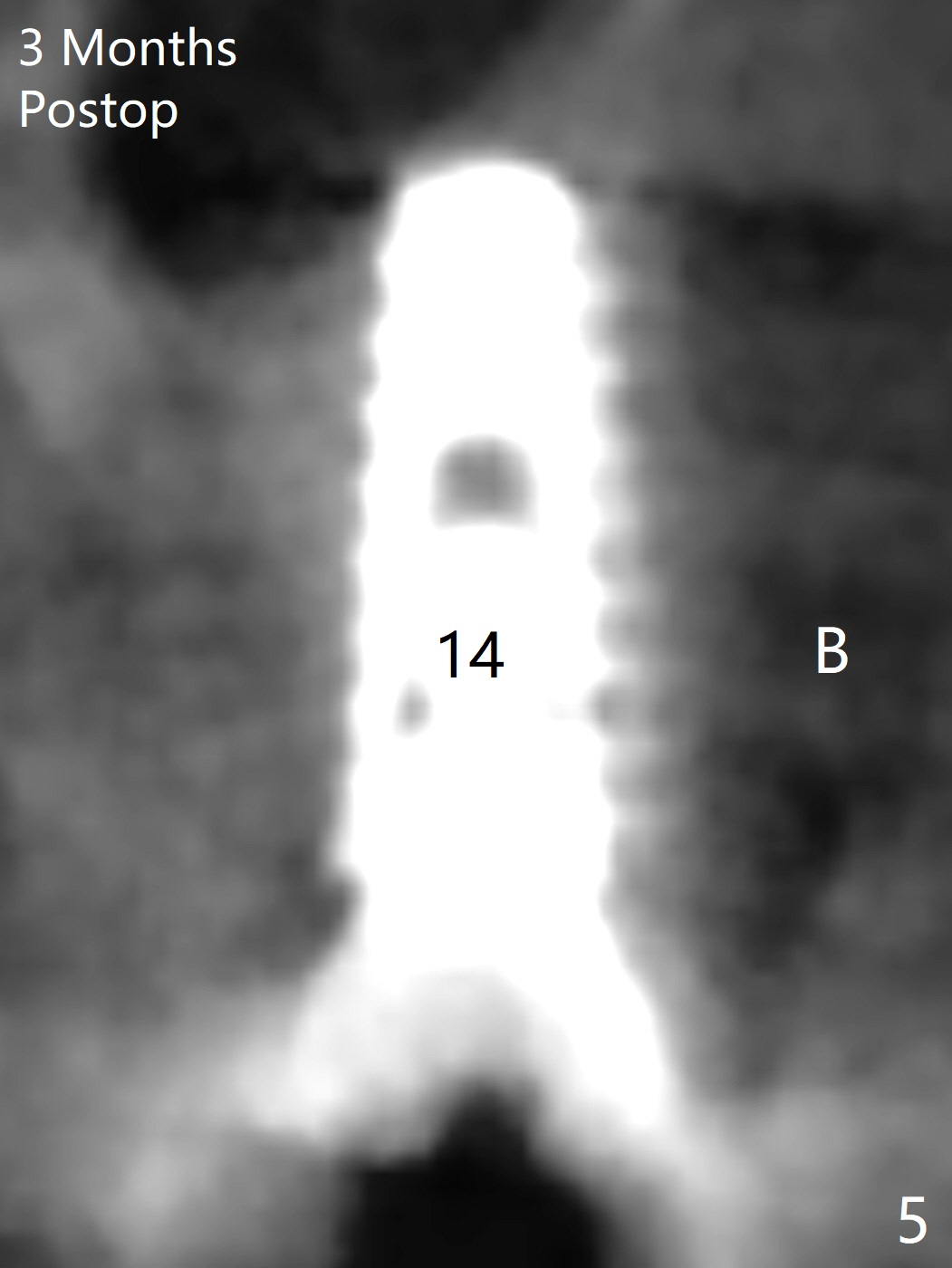
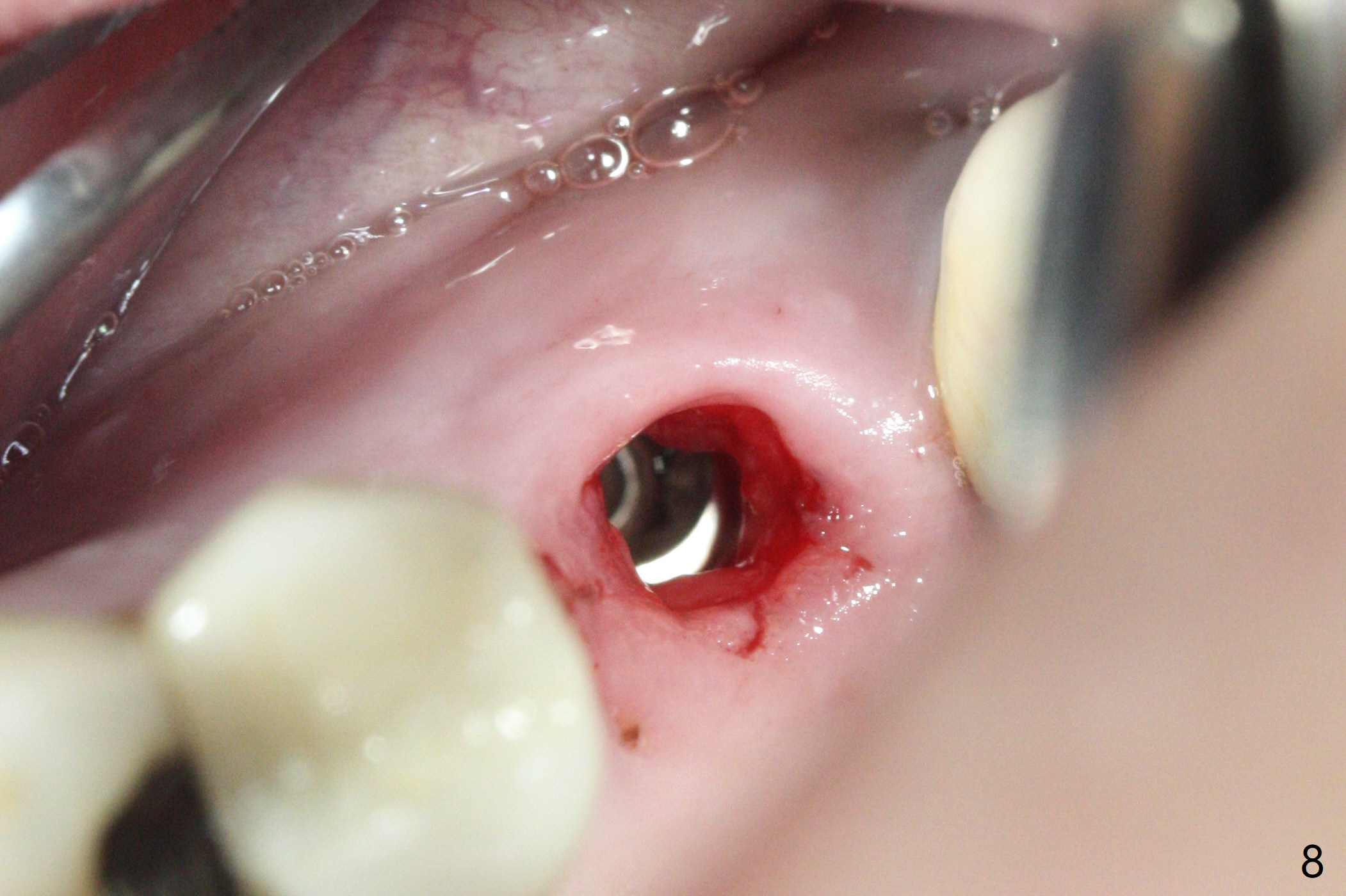
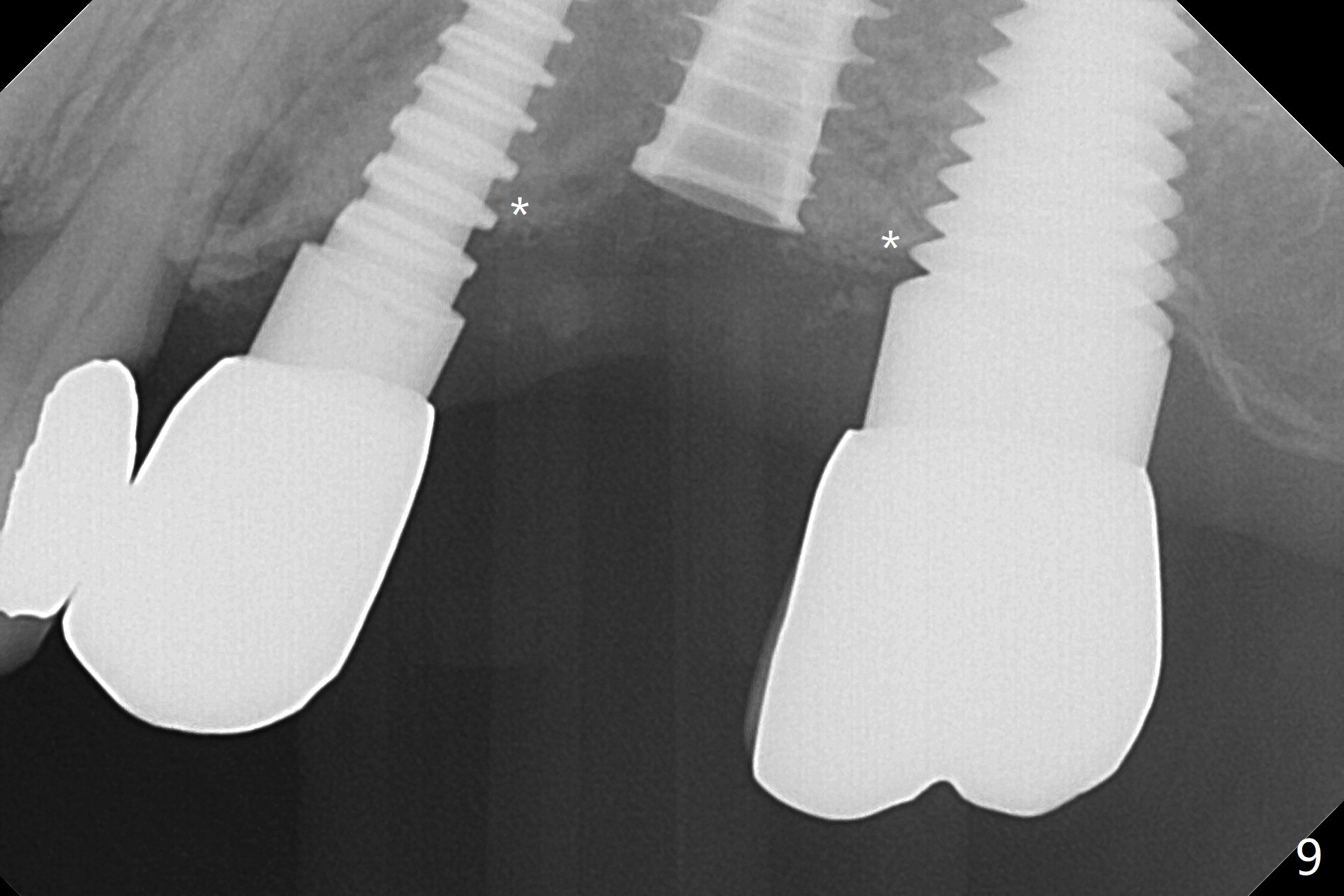
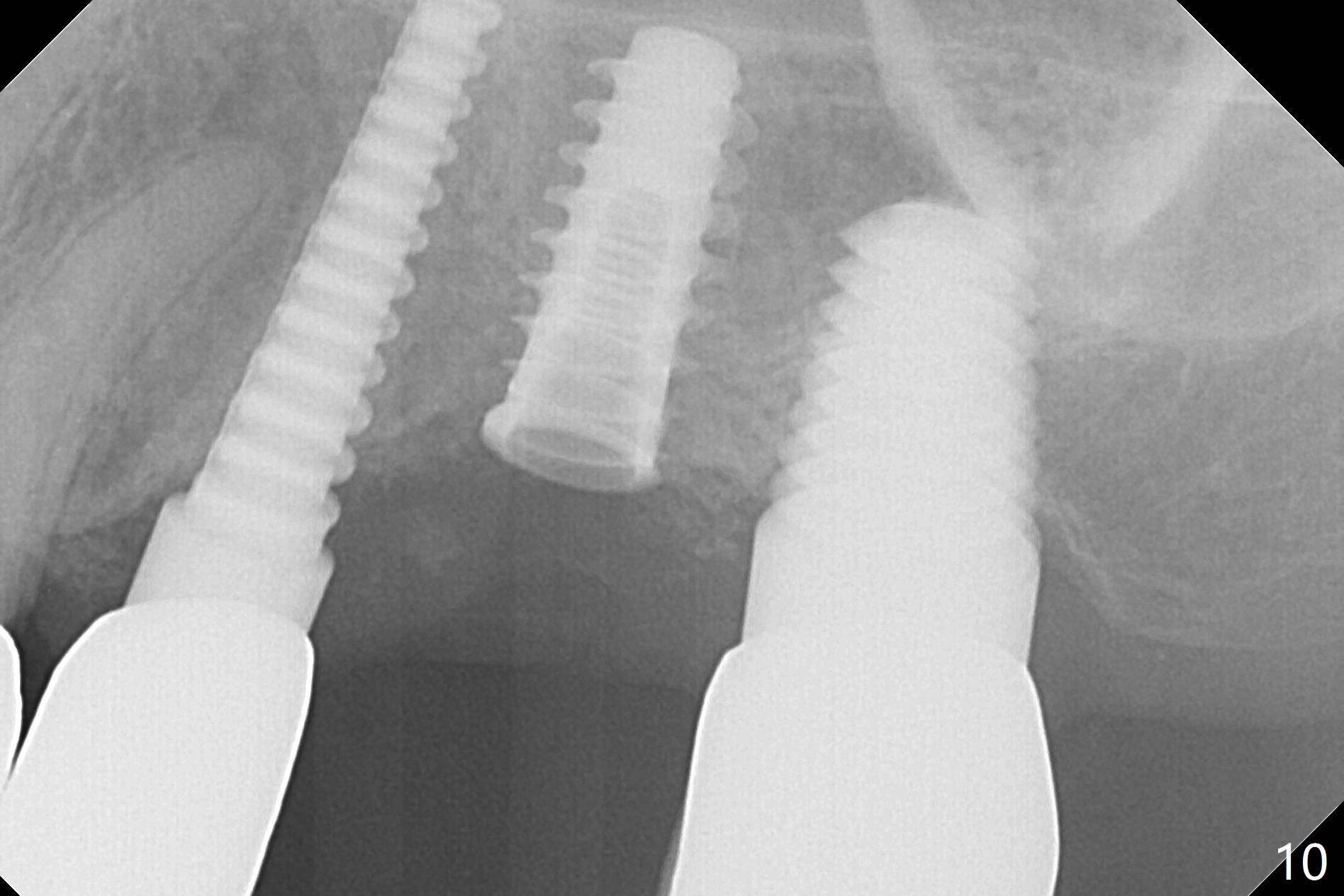
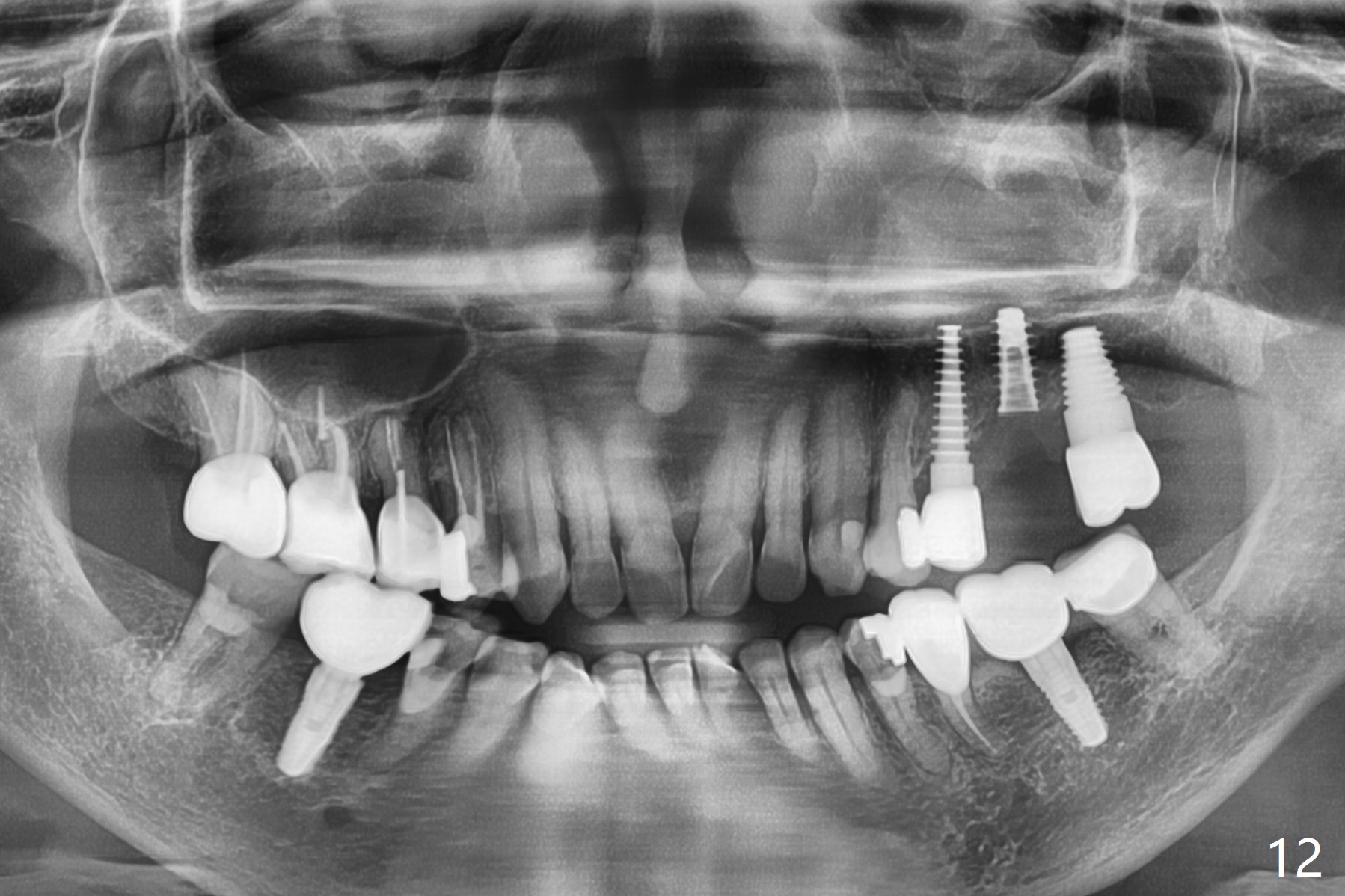
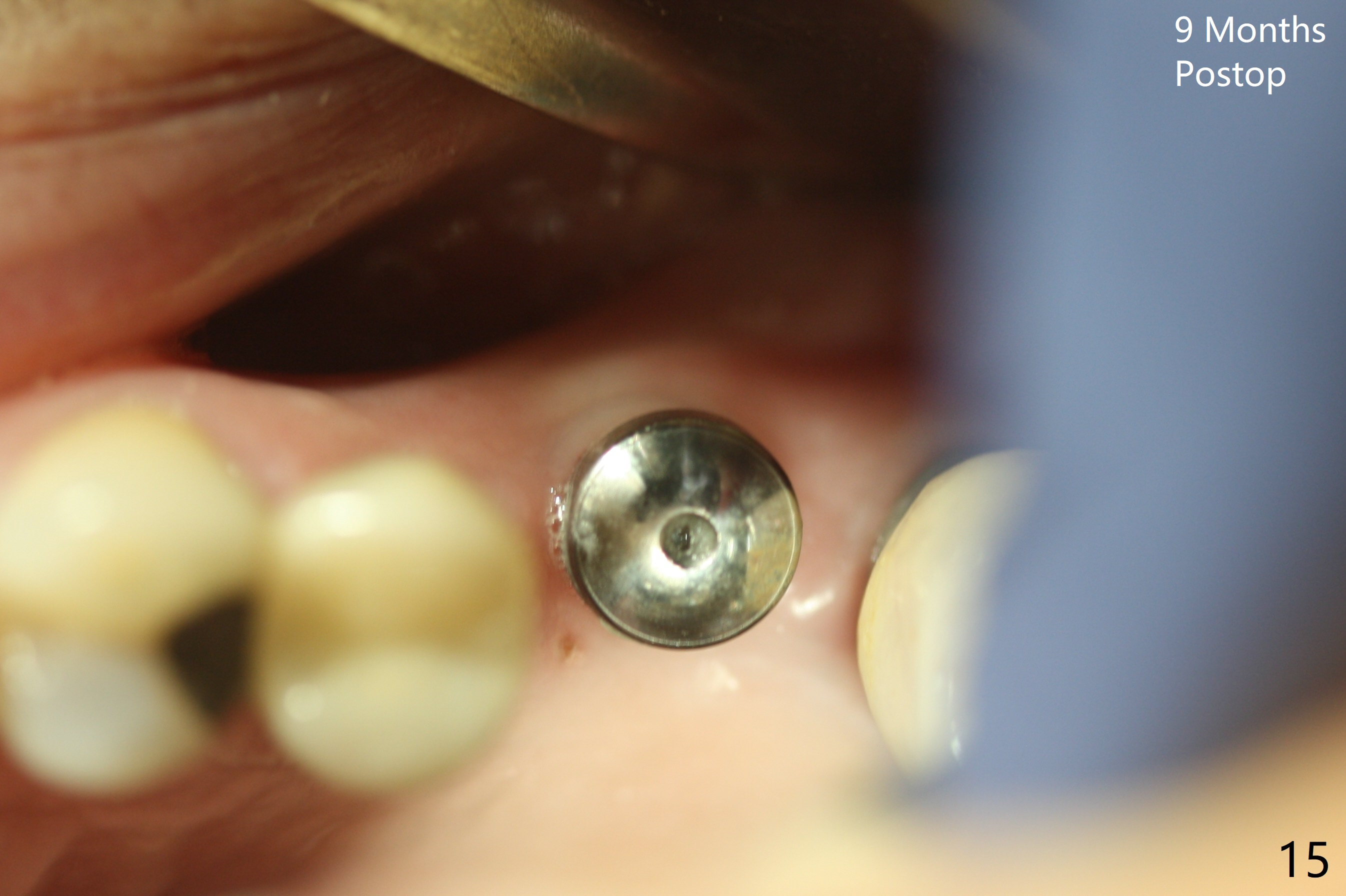
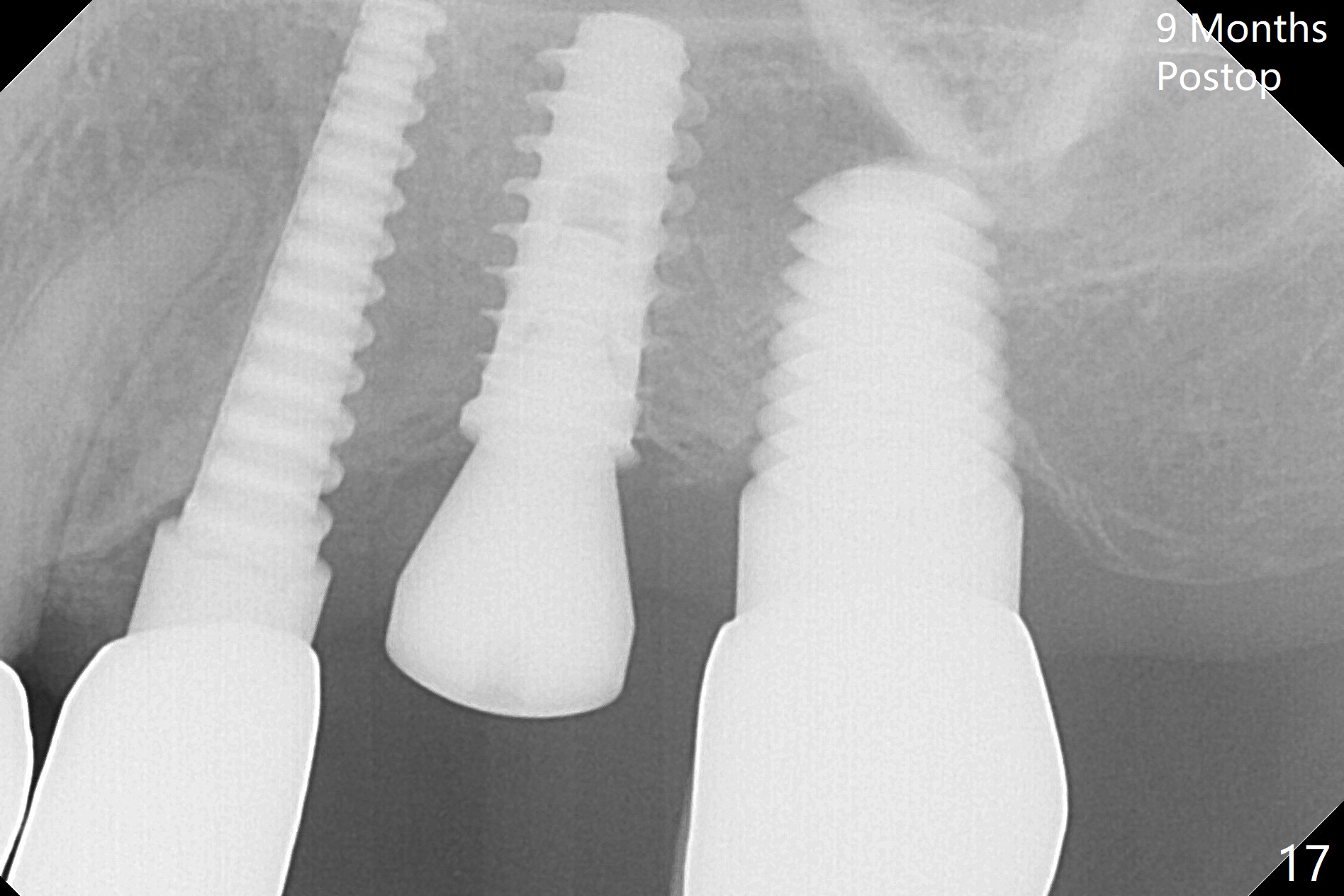
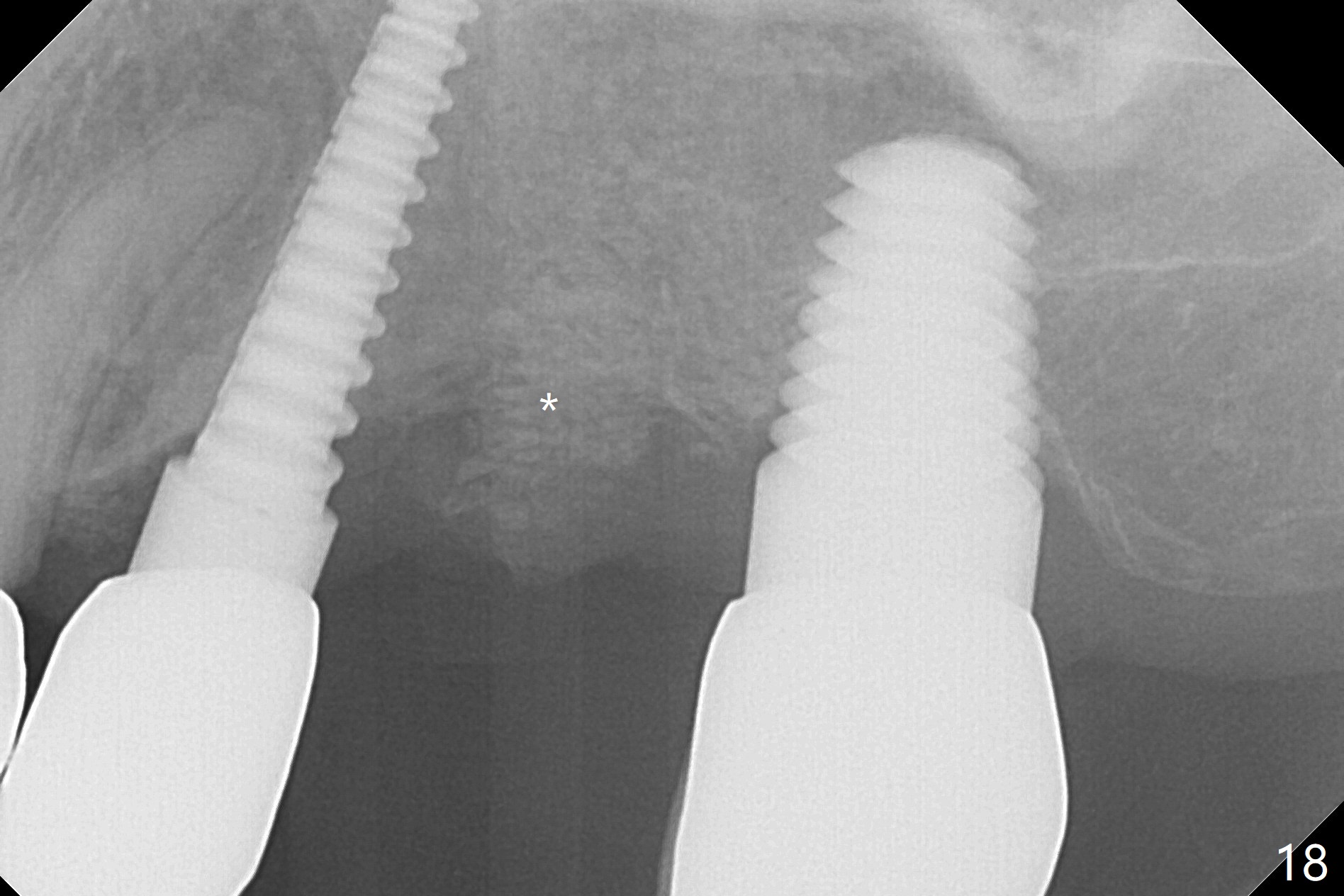
Initial osteotomy in the septum of the tooth #14 is 9 mm, approximately 2 mm from the sinus floor (Fig.1). Subsequent osteotomy depth is 11 mm, followed by insertion of a 4.5x11 mm dummy implant (Fig.2). After use of Magic Drill (MD) 4.8 mm for 9 mm, a 5x11 mm IBS implant is placed with sinus lift without additional bone graft (Fig.3 *). In contrast, autogenous bone (from MD) and Vanilla Graft are meticulously placed in the remaining socket (+) before and after placement of a 6.5x5.7(2) mm abutment. An immediate provisional is fabricated to close the sockets. There is buccal tenderness 1-3 months postop. There is distopalatal implant thread exposure. A healing abutment (5.5x2 mm) is placed. CT confirms thin buccal plate (Fig.4,5). It appears that the implant should have been as palatal as possible. The tenderness remains for the next 2 weeks. When the healing abutment is removed, the implant seems to have been placed shallow, ~ 1 mm subgingival (Fig.6). With local anesthesia, the implant is reversed to clean the coronal threads with Titanium brush and copious irrigation (Fig.7). The implant is then placed ~4 mm subgingival (Fig.8) and slightly subcrestal (Fig.9,10). It appears that the postop bone loss (Fig.9 *, as compared Fig.1,2) makes the implant look to be placed too shallow. When the implant is being placed deeper, the buccal plate feels intact. The early periimplantitis is apparently due to postop bone loss more than buccal placement, although certain degree of buccal bone resorption must occur. A 6x4 mm healing abutment is placed. Left facial swelling develops 2 days post implant elevation (Fig.11,12, as compared to preop (Fig.13)). The left maxillary sinus cloud (Fig.12) appears to be a false positive finding, since the same feature exists prior to implant elevation (Fig.13). Both sinuses look clear prior to implant elevation (Fig.14). Amoxicillin switches to Augmentin and Flagyl, since the patient is reluctant to have the implant removed. Finally the sinus infection is under control. The patient feels left facial swelling 9 months postop (5 months post elevation) and reports left nasal discharge ~ 1 month earlier. There is mild buccal plate tenderness. The implant seems to be buccally placed (Fig.15,16), although there is no significant change radiographically (Fig.17). The implant is removed with bone graft (Fig.18 *). To avoid complication and failure, an immediate implant at the upper 1st molar should be short and placed deep.
Return to
Upper
Molar Immediate Implant, Prevent
Molar Periimplantitis (Protocols,
Table), Armaments
#19,
30 (Plan)
Xin Wei, DDS, PhD, MS 1st edition 11/10/2017, last revision 12/28/2018