



|
|
|
|
|
|
|
|
|
|
Bone Expansion in Healed Site
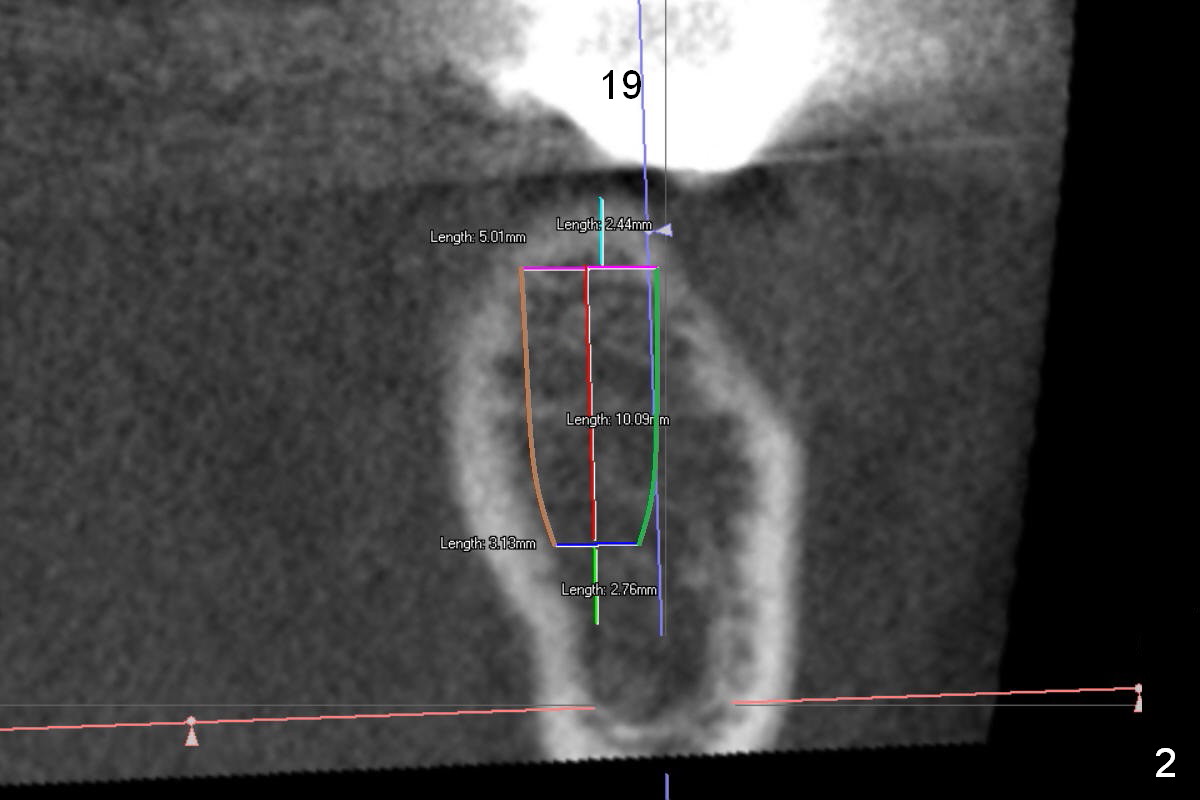
A 68-year-old lady has had a lower right bridge for 10 years (Fig.1,2 (CBCT section), Fig.3 (3 D image)). There is caries underneath #20 retainer (mesiolingual) with symptom. The retainer and the pontic at #19 will be removed. The tooth #20 may need root canal therapy. An implant will be placed at #19, but the crest is narrow (Fig.2 coronal section).
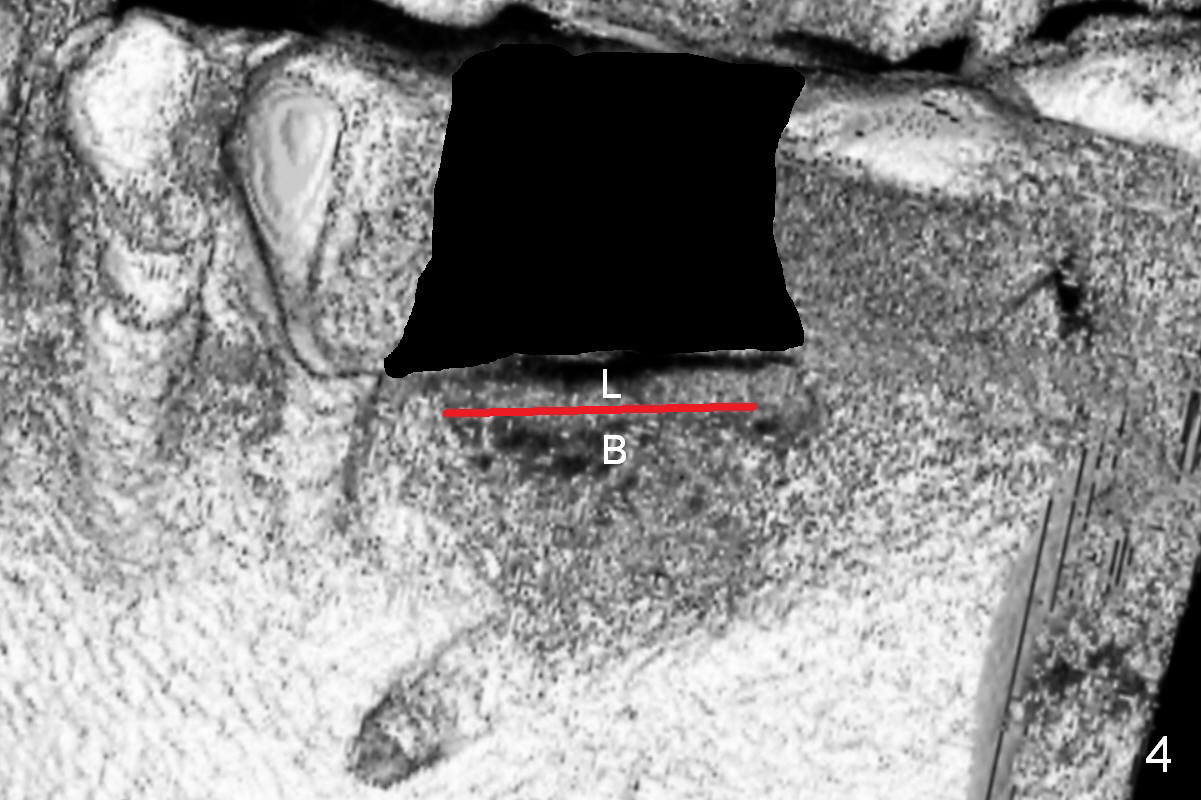
Bone density at the crest appears to be low (Fig.3 arrowheads). After pontic removal (Fig.4 black area) and incision, use #15 scalpel, bone scalpels and bone blades to start bone expansion (red line). Bone expansion continues with D osteotomes (Fig.5 red area) which mainly moves the buccal plate (B) buccally. The 3rd step of bone expansion is to use RT (round tapered) osteotomes or bone expanders (Fig.6 white circle); the buccal plate keeps being expanded more the lingual one (L). When an implant is placed, the lateral spaces created by expansion will be filled with bone graft. If the depth of osteotomy is not enough, use drills to reach the desired one.
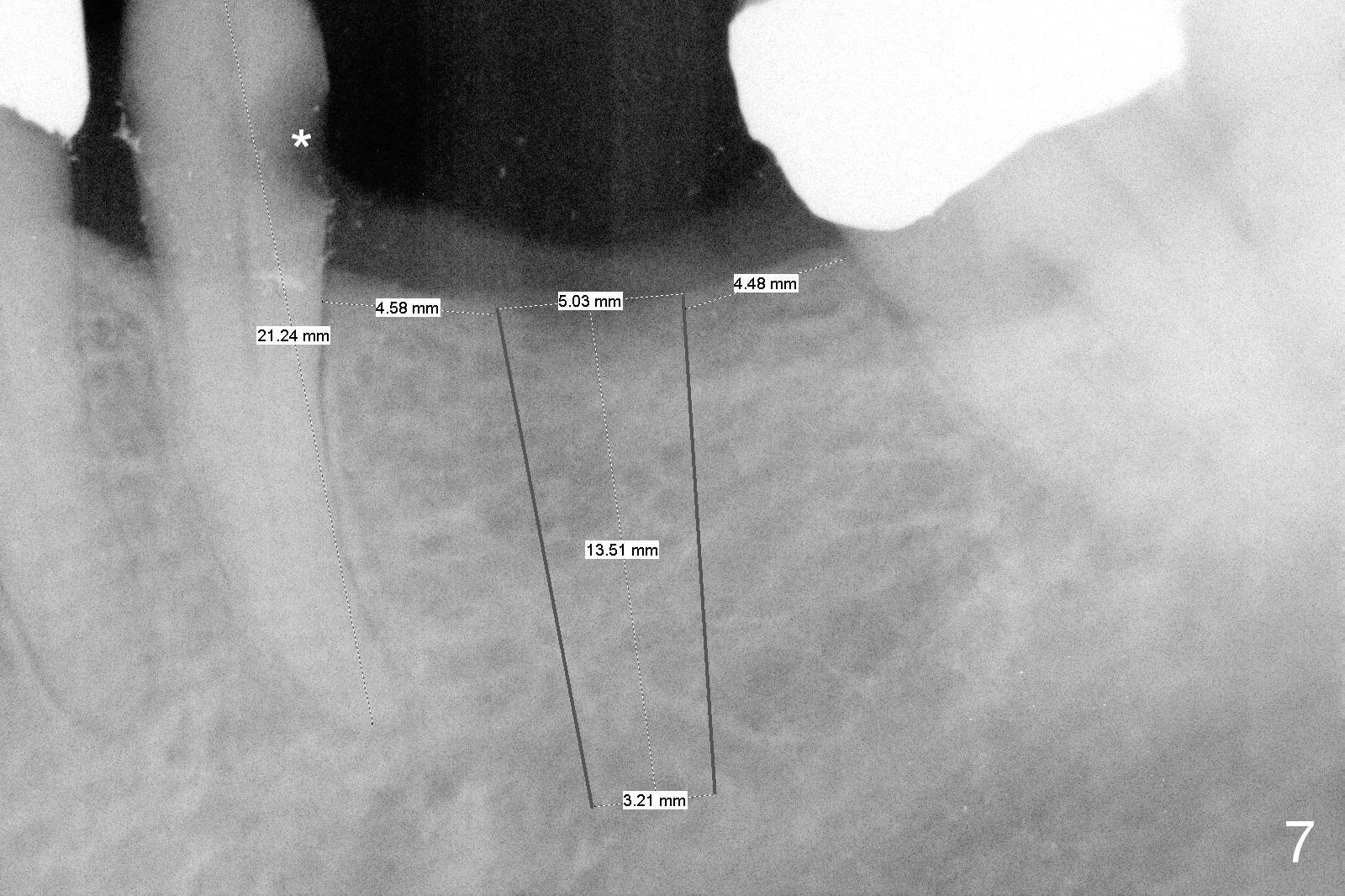
Because of pain, the bridge has been removed partially. Caries in the tooth #20 (Fig.7 *) is confirmed; root canal therapy has been done. With bone expansion, the bone level implant can be placed at the crest. That is, it can be longer (Fig.7: 13.5 mm) than the one placed subcrestally (Fig.2: 10 mm).
Take photos prior to surgery to show the narrow crest, as compared to #30 extraction socket of the same patient. Use SM cassette; initial depth is 12 mm.
Return to Lower Molar Immediate Implant
14
Xin Wei, DDS, PhD, MS 1st edition 09/05/2015, last revision 02/23/2018