

%20trimmed,%20.5-1.5%20mm%20allograft.jpg)





|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
||||
Dense, Thin Septal Bone
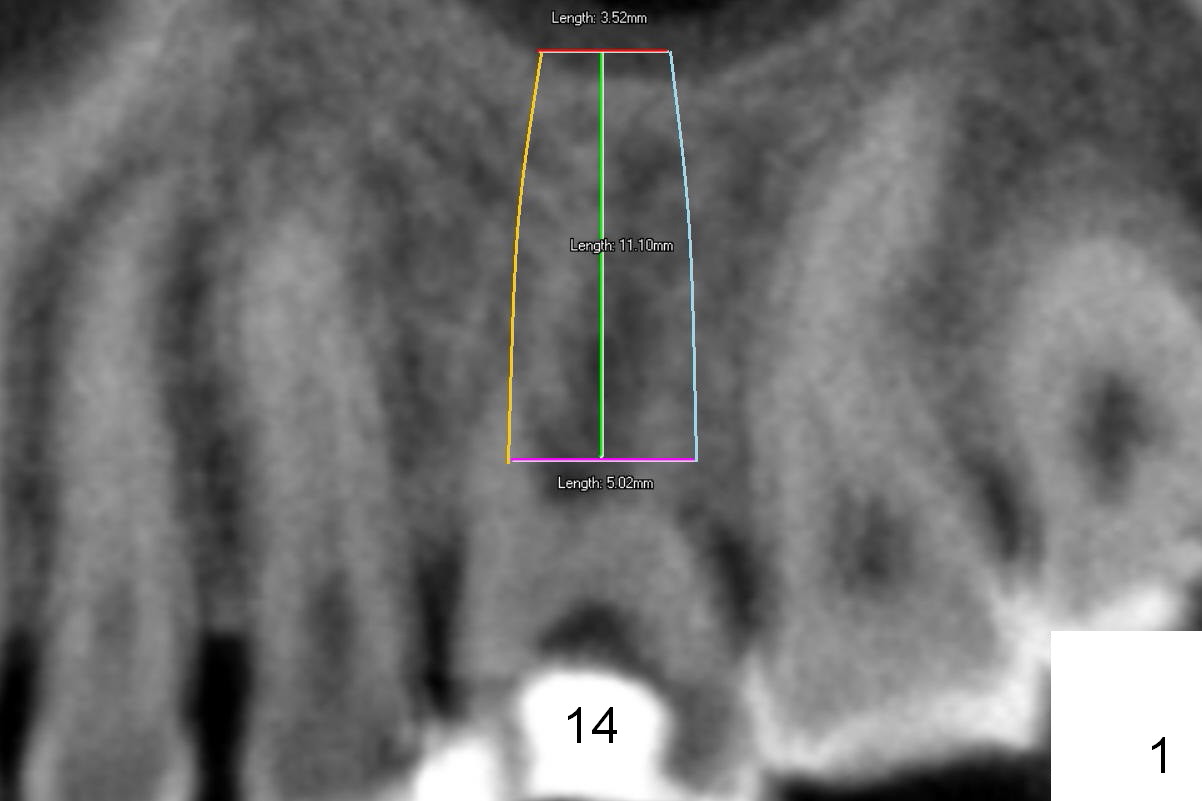
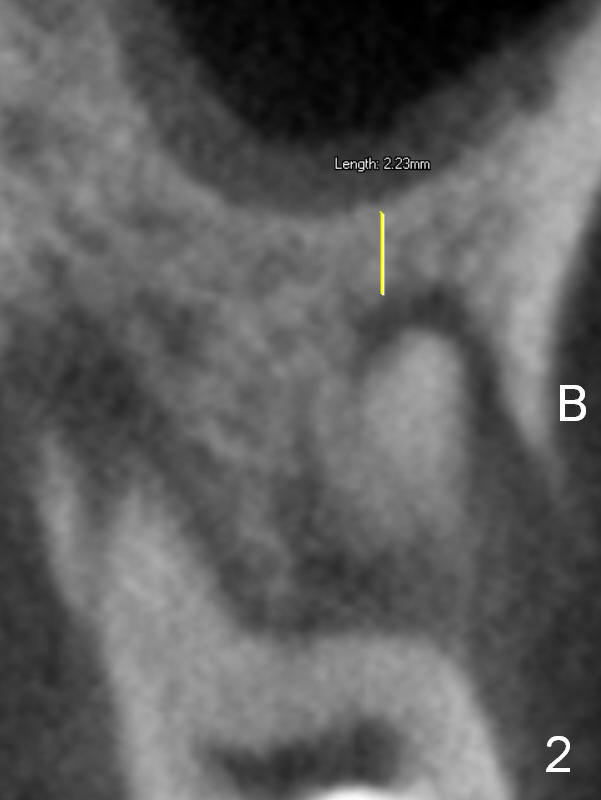
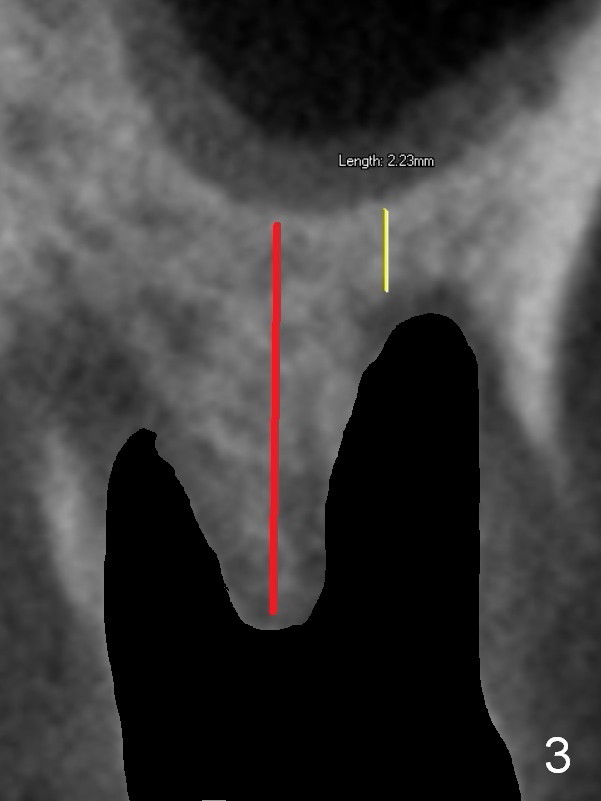
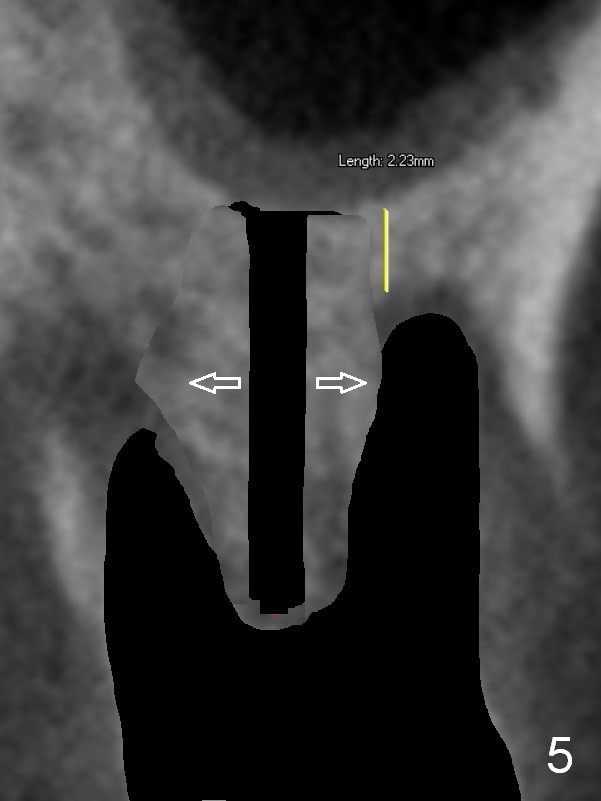
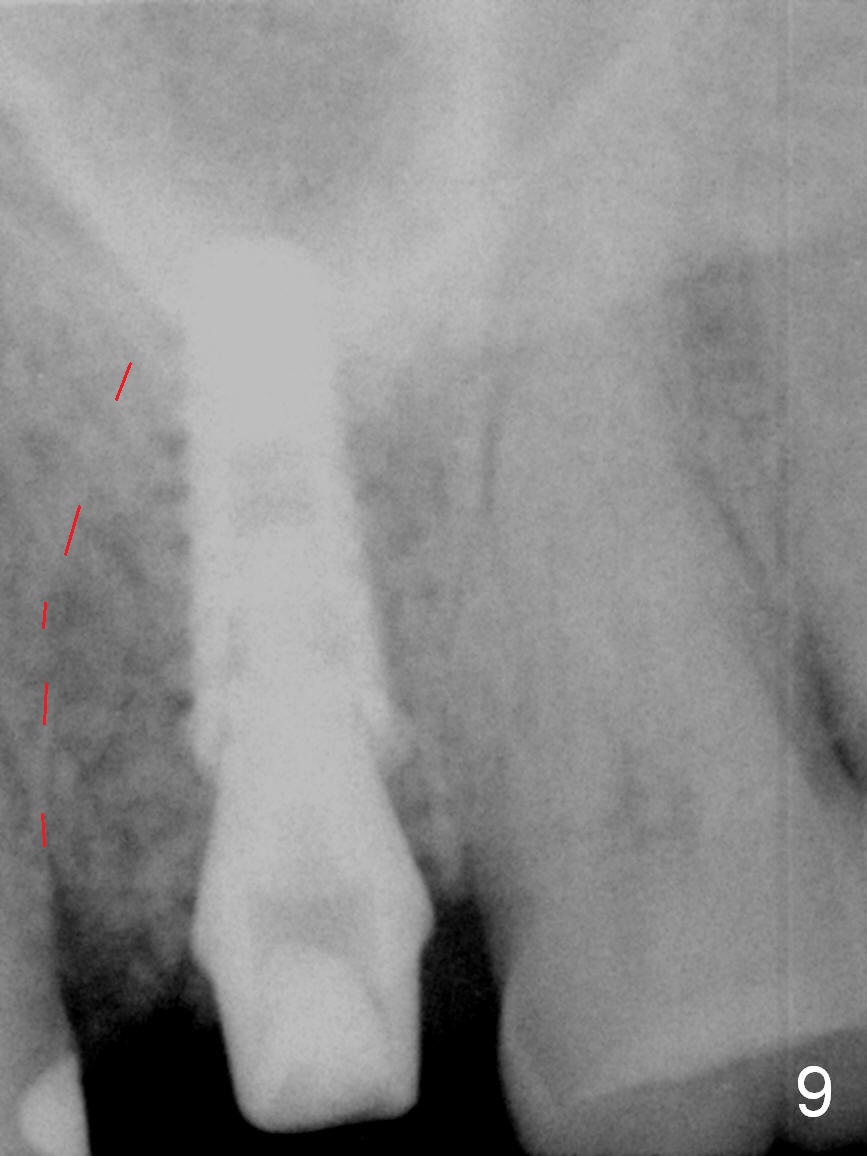
Preop CT shows that the septum appears to be able to hold a 11 mm long implant (Fig.1 sagittal section). There are periapical radiolucent lesions of the buccal (Fig.2 (coronal section) B) and palatal roots; bone height above the buccal apex is ~ 2 mm (Fig.3). When the tooth #14 is extracted, a 1.6 mm pilot drill is used to start osteotomy in the middle of the fairly thin septum (Fig.3 red line, Fig.4 S). It is hoped that Magic Expanders (ME) can enlarge the osteotomy by pushing the buccal and palatal bone plates of the septum outward (Fig.5 arrows).
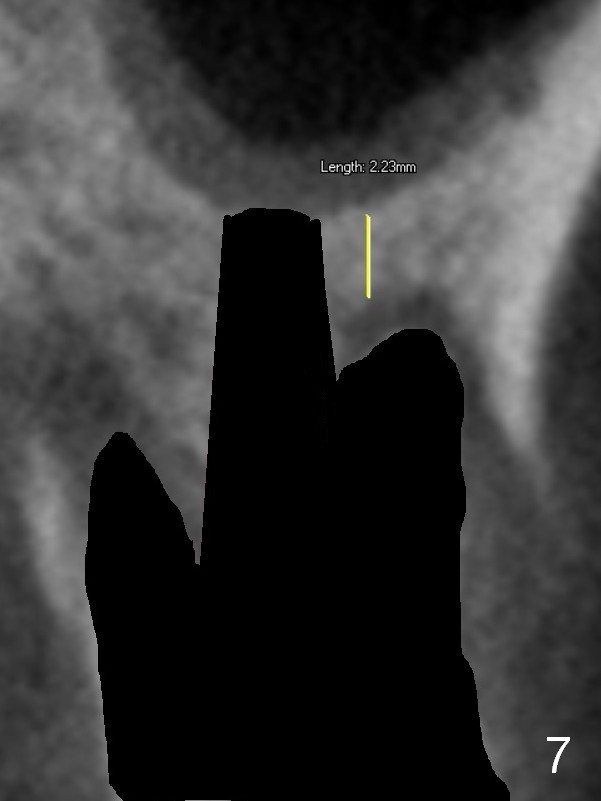
The septal bone is dense and the osteotomy is enlarged by alternating use of drills and expanders. By the time 3.8 mm ME is tapped in (Fig.6), the buccal plate of the septum is perforated. The ME is stable, in spite of the fact that it is only supported by 2-3 mm bone buccally (Fig.7). Continuously alternating use of MEs and drills leads to placement of a 5x11 mm implant with 30 Ncm insertion torque and sinus lift. After placement of bone graft (Fig.8 *) and 5x4(3) mm pair abutment (A), an immediate provisional is fabricated. Red dashed lines in Fig.6,9 represent the mesial outline of the socket, whereas black dashed in Fig.6 sinus floor. It suggests that the implant is stabilized by relatively small amount of native bone. Although IBS implants have aggressive thread patterns, a proper apical osteotomy should be prepared in the depth (perforates the sinus floor in this case) and diameter (4.3 mm drill) prior to placement.
Mild palatal swelling is present around the former fistula 9 days postop (Fig.10 *). No treatment is rendered. There is small buccal gap with exposure of the bone graft (Fig.11 <). Periodontal dressing is applied to prevent further loss of bone graft (Fig.12).
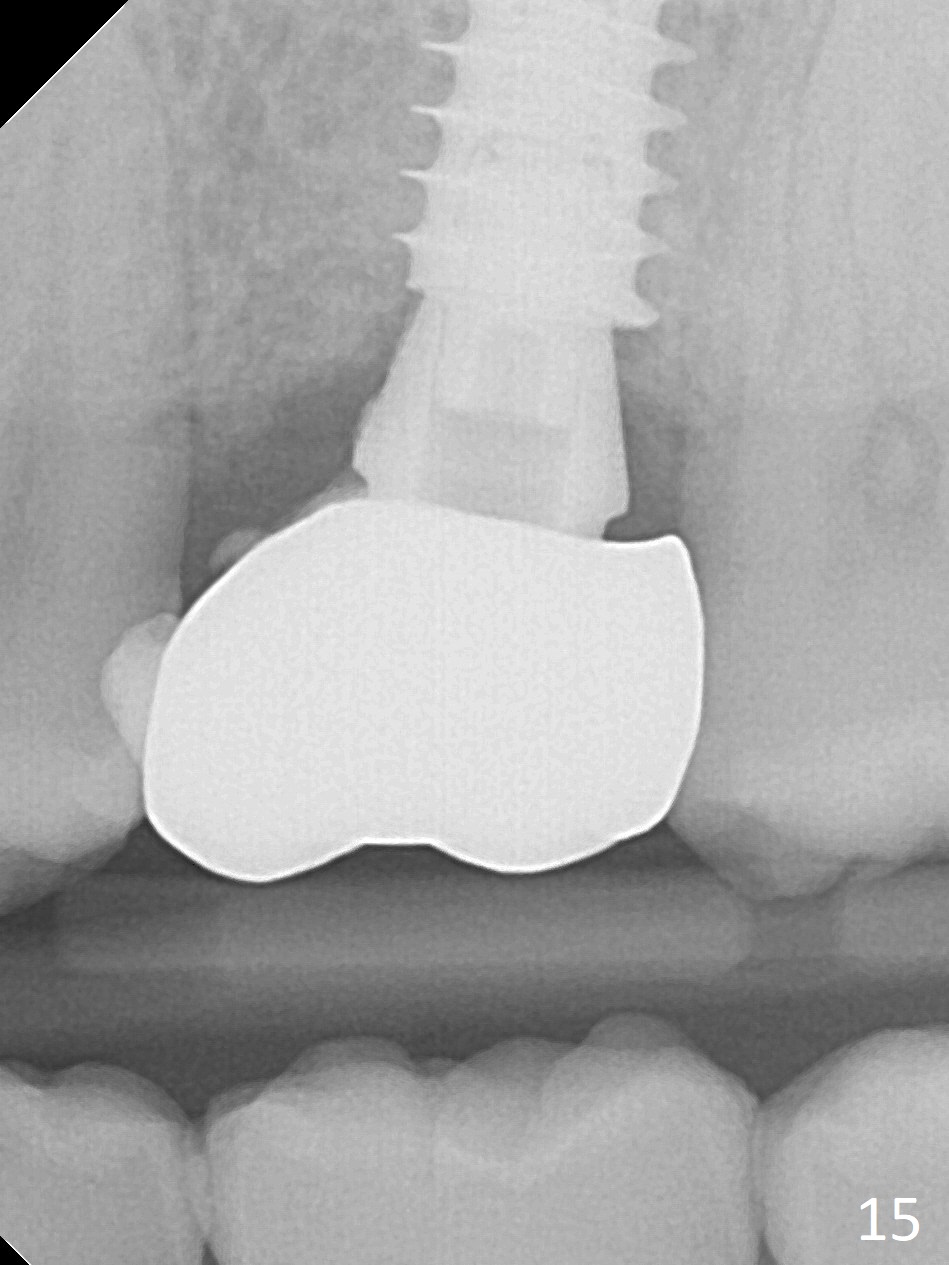
It seems that the provisional traps food. The former has been removed by the patient by the time she returns 3.5 months postop. The gingiva around the implant is healthy. The organization of the bone graft has changed (Fig.13, as compared to Fig.8,9). The implant has osteointegrated. Take photos to show the buccal and palatal gingival margin before impression. In fact the newly formed gingiva covers the margin of the abutment 5 months postop (Fig.14). Laser gingivectomy is performed prior to impression. Provisional should be kept in place with good oral hygiene. The crown dislodges 8 months post cementation, probably due to bruxism, small, short abutment and open margin (Fig.15 (taken after recementation; the residual cement is removed later)).
Return to
Upper
Molar Immediate Implant,
Prevent Molar Periimplantitis (Protocols,
Table), IBS
Xin Wei, DDS, PhD, MS 1st edition 08/02/2016, last revision 08/30/2018