
|
|
|
|
|
|
|
|
|
|
|
|
Fully Compact Peri-implant Gaps with Bone Graft M
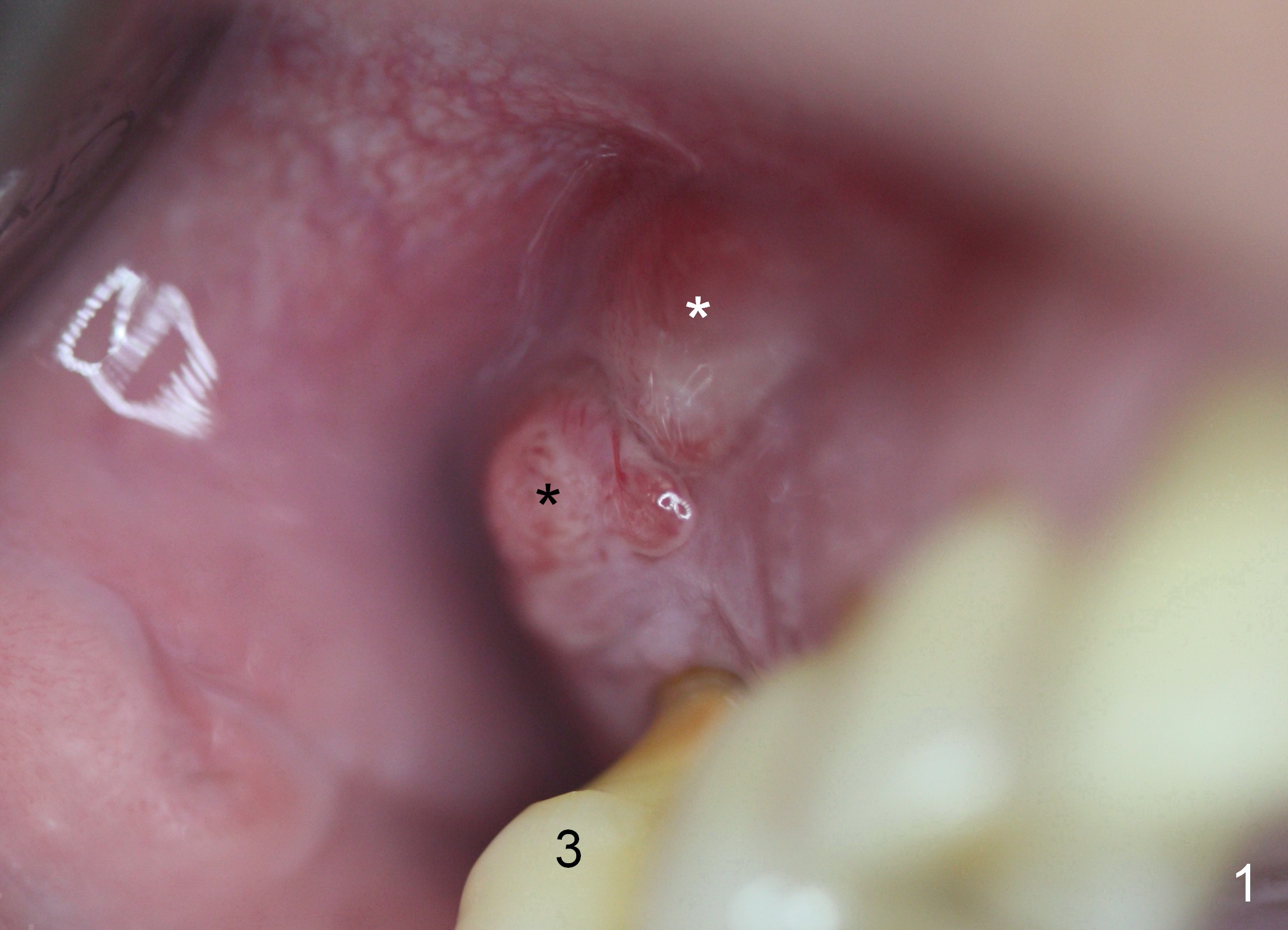
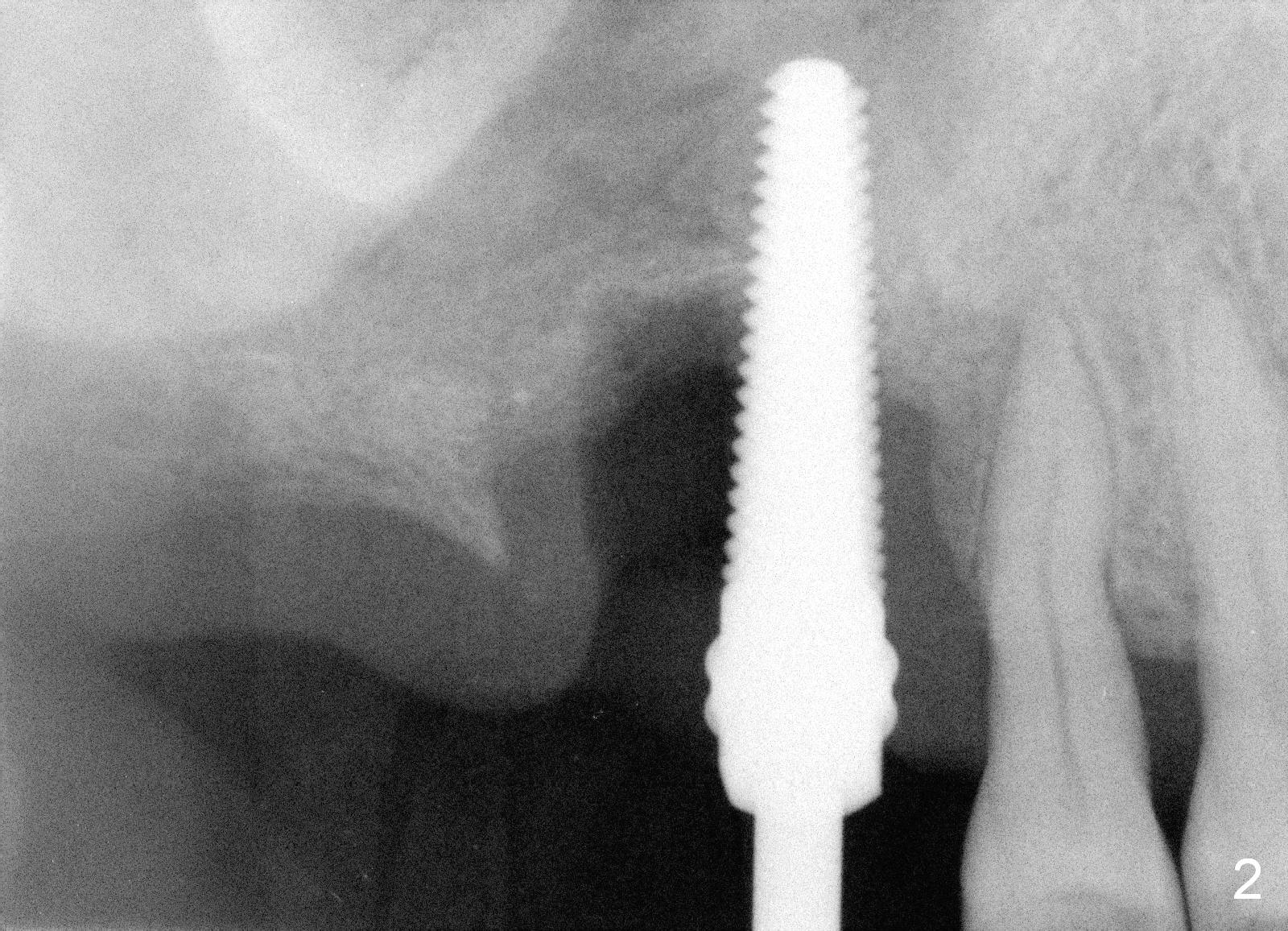
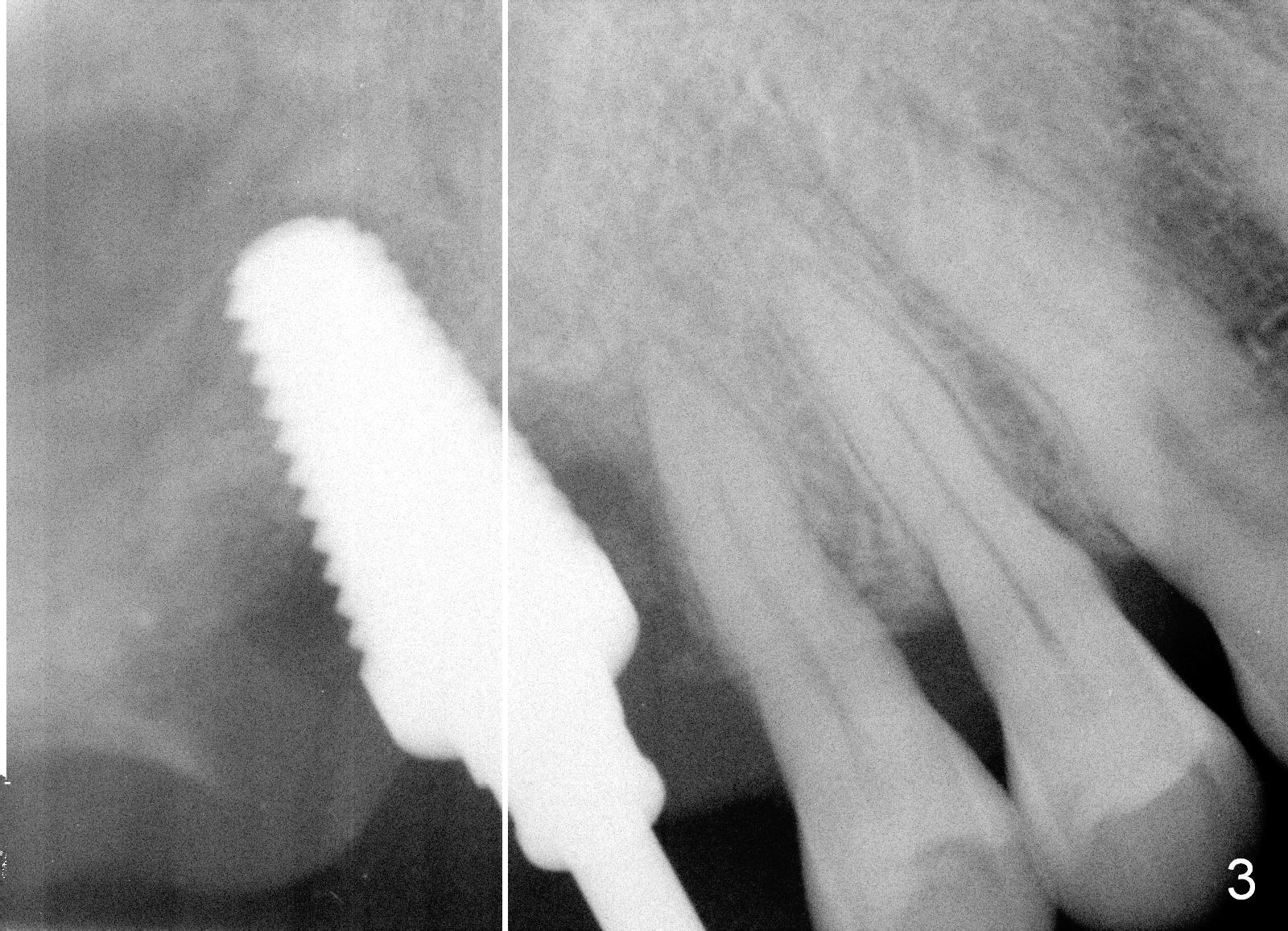
When the patient returns for #3 extraction and immediate implant, there is severe buccal swelling in spite of 2-week oral Amoxicillin (Fig.1 *). The extraction is relatively easy, including removal of the mesiobuccal and distobuccal root fracture fragments. But removing granulation tissue is time consuming. The buccal plate is lost. Osteotomy is initiated in the buccal slope of the septum with osteotomes, followed by insertion of taps to test stability (Fig.2,3). The sinus membrane is found to be perforated and repaired by insertion of collagen dressing prior to placement of a 8x17 mm tissue-level implant (Fig.4).
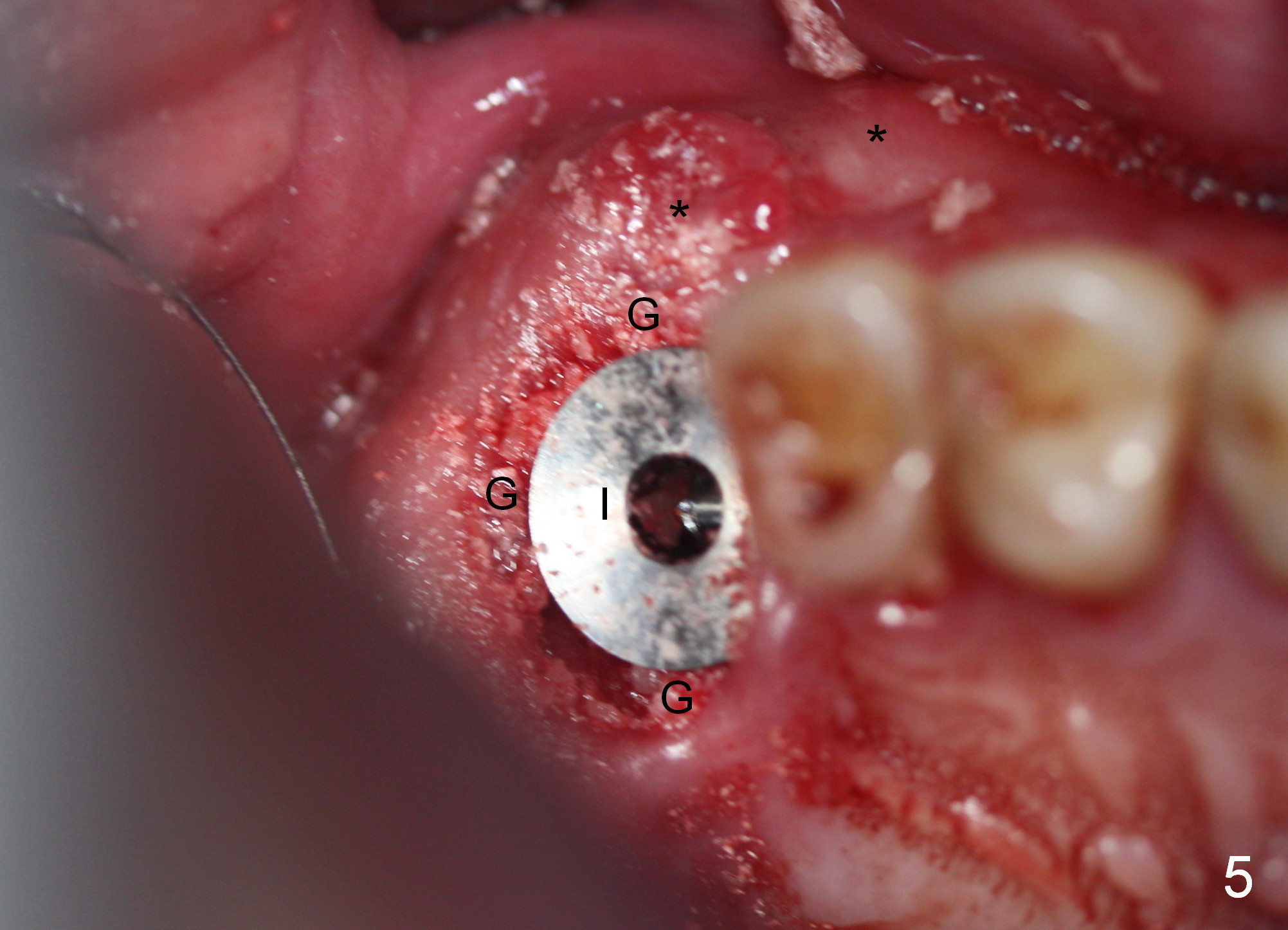
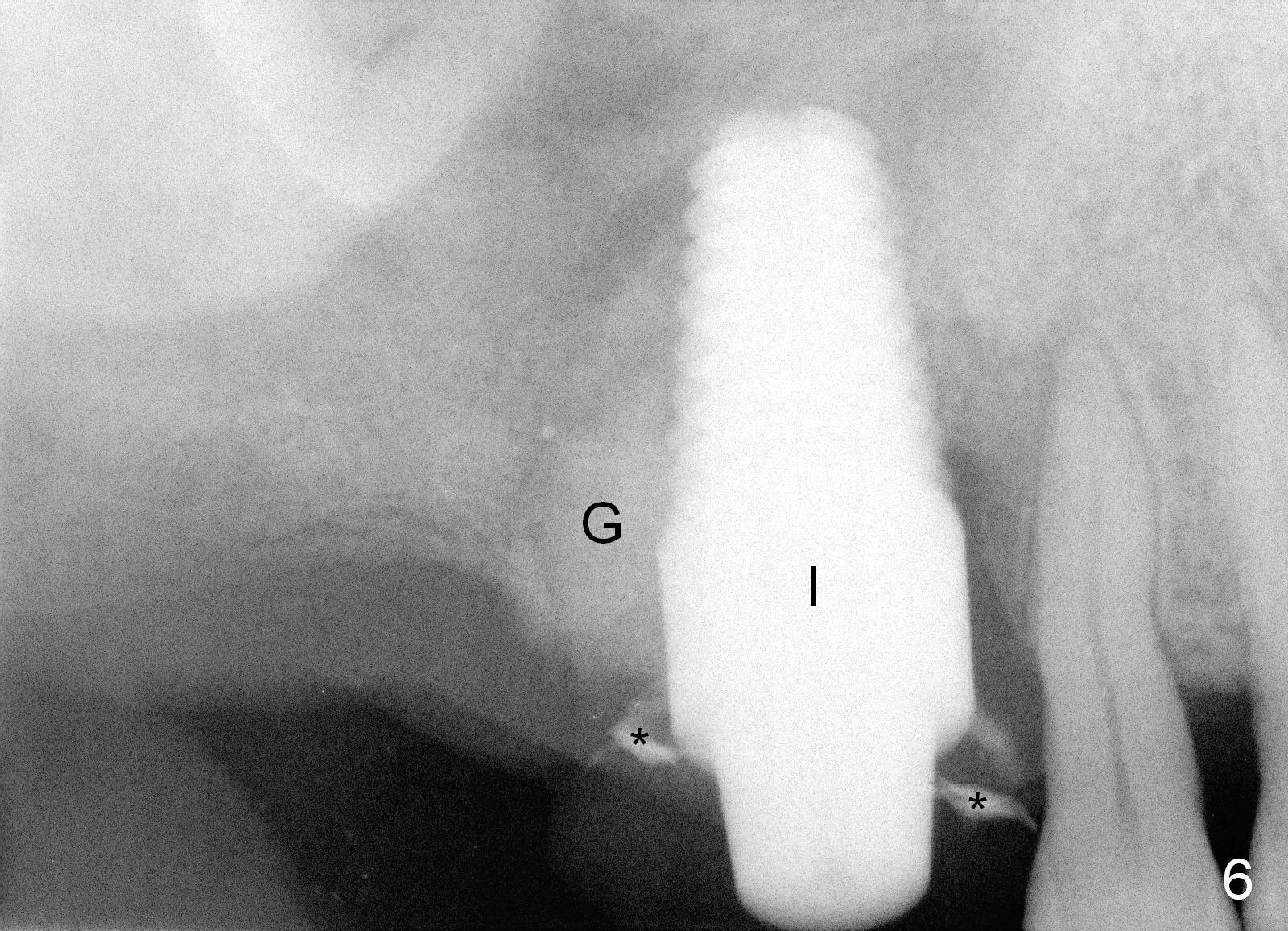
The buccal plate repair involves insertion of Osteotape (collagen membrane with Osteogen) and a large amount of allograft mixed with Osteogen (Fig.5,6 G) around the implant (I). There is no buccal gingival collapse (Fig.5 *). The graft is held in place by collagen dressing and an immediate provisional (Fig.6 *: temporary cement).
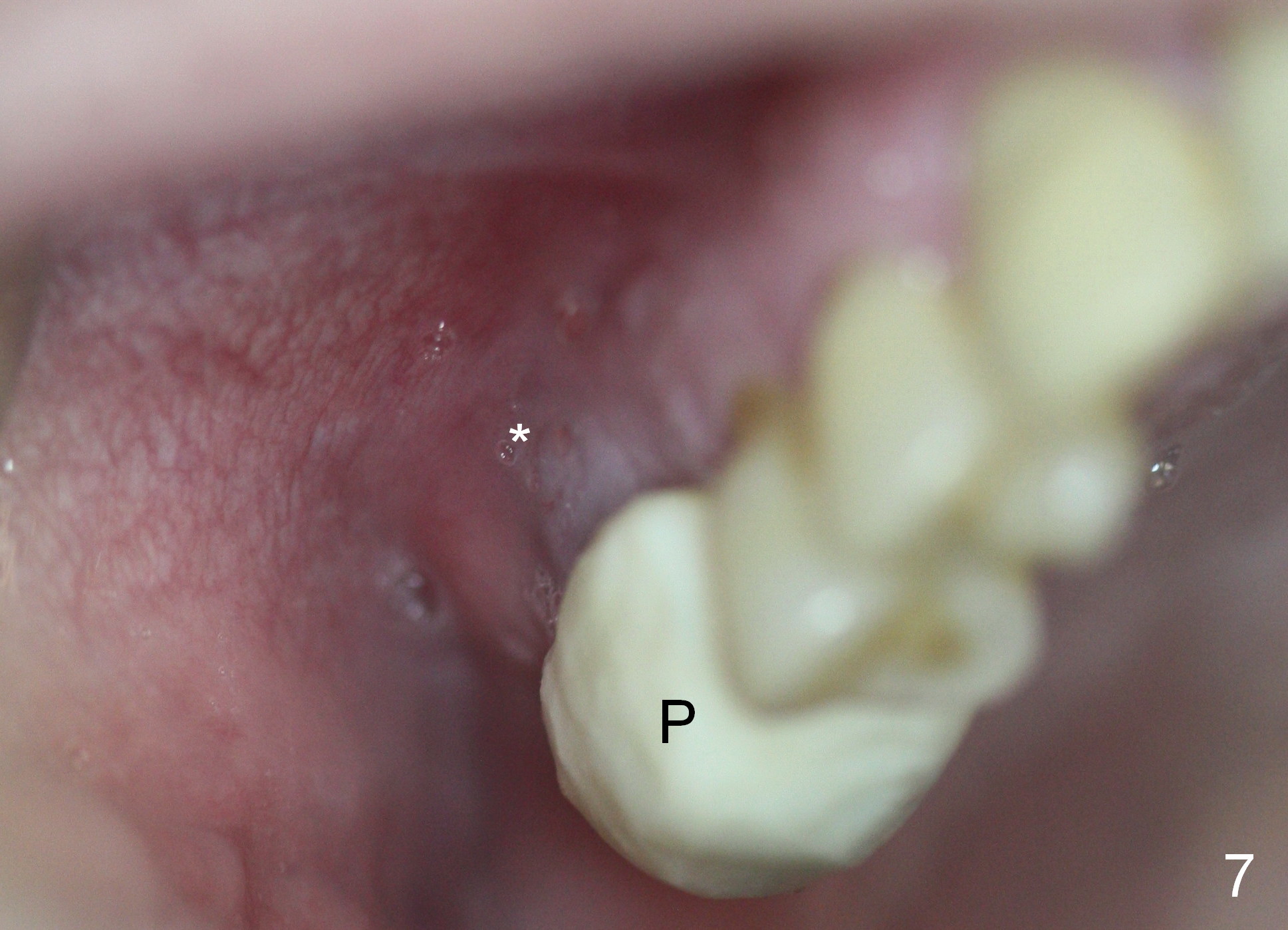
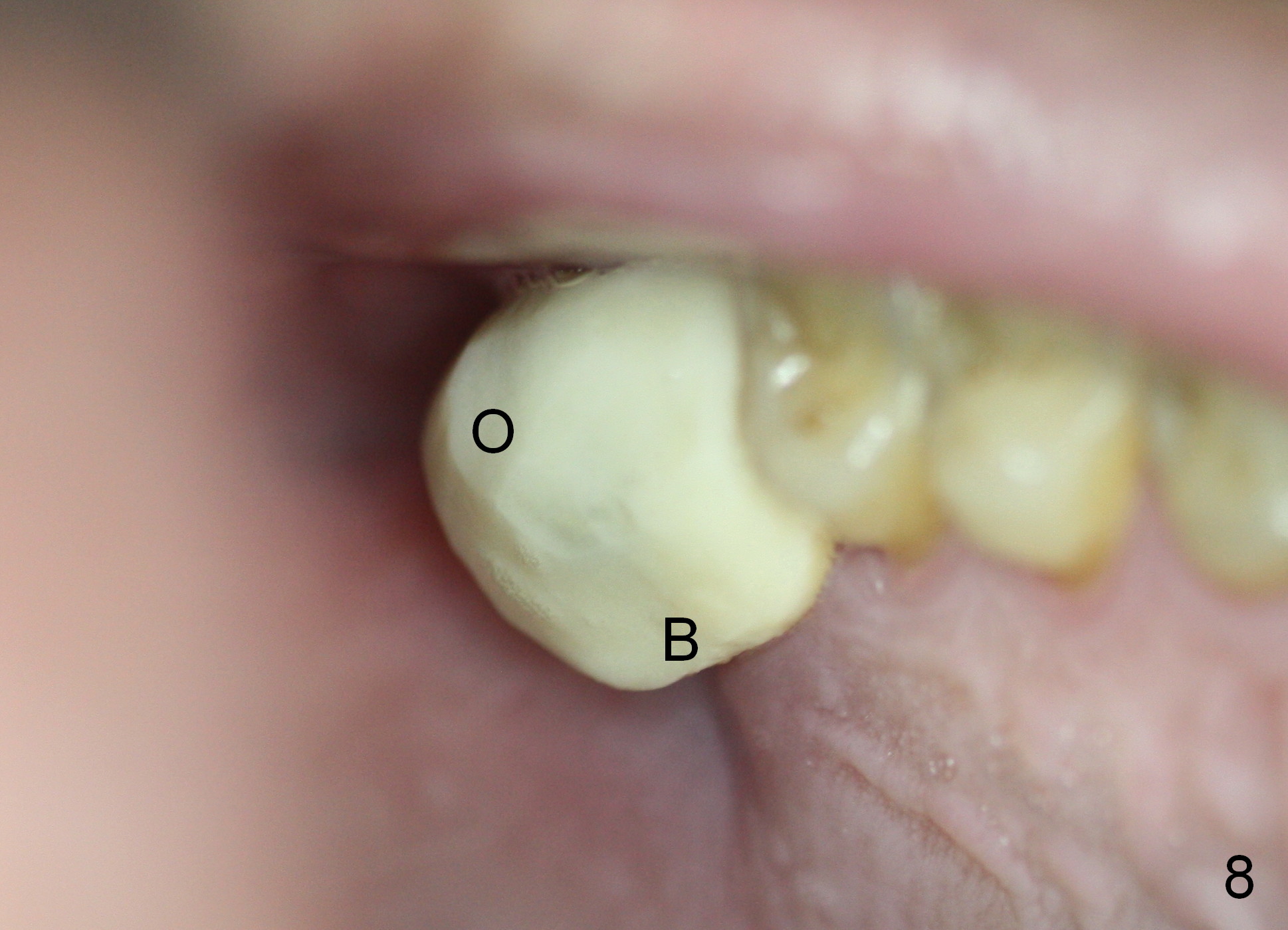
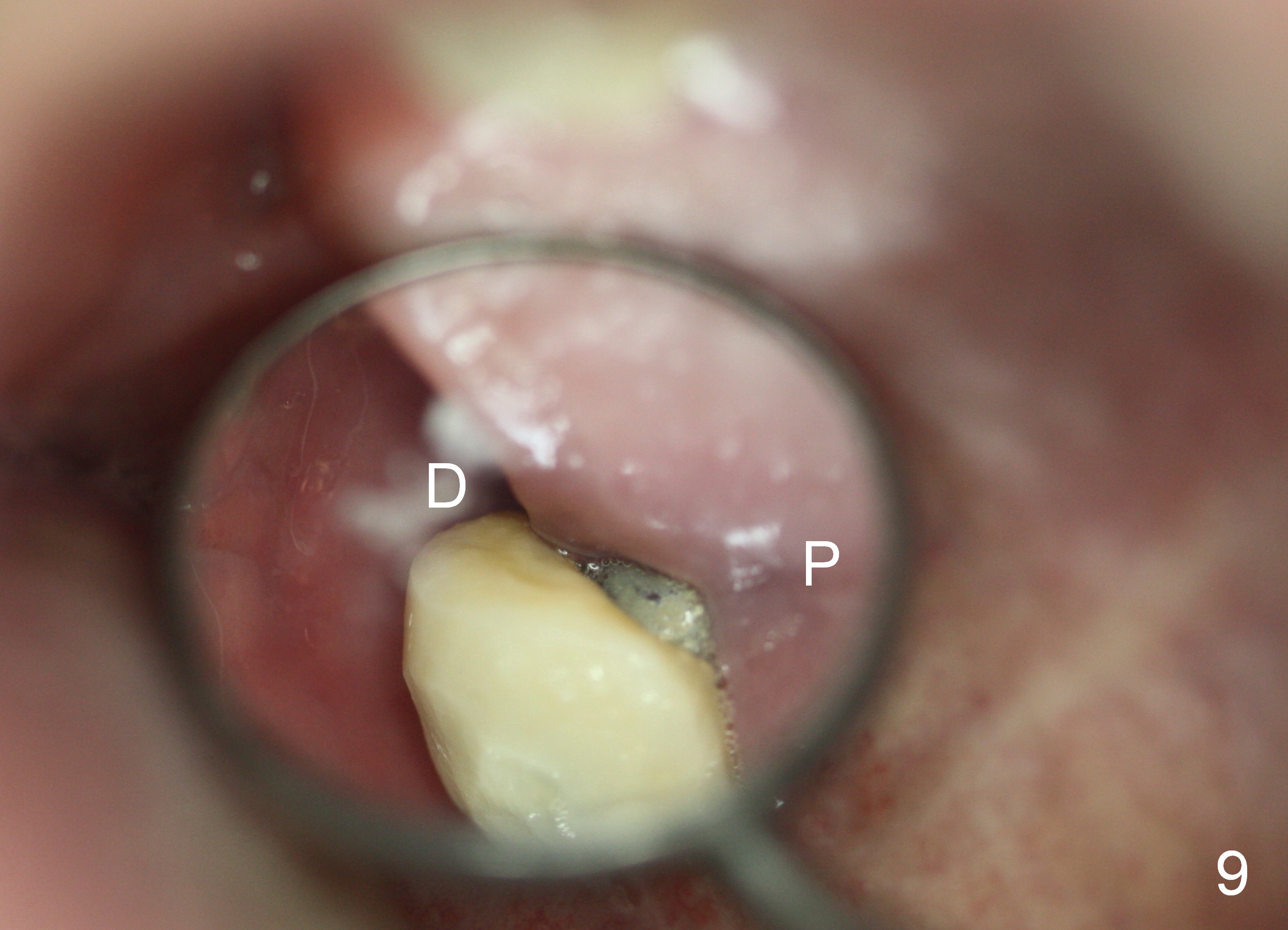
There is no buccal swelling 8 days postop (Fig.7 *; P: provisional). The occlusal table of the provisional (Fig.8 O) should be as small as possible to reduce occlusal contact, whereas the base (B) be as large as possible to keep the graft in place. In one area (such as palatal (Fig.9 P; D: distal)), the provisional does not contact the gingiva. Sometimes perio dressing is required for further seal. In fact, the implant has to be removed 1 month postop.
Return to Upper Molar Immediate
Implant,
Posterior Immediate Provisional,
Immediate Implant Complications
Xin Wei, DDS, PhD, MS 1st edition 05/09/2015, last revision 12/26/2019