

|
|
|
|
|
|
|
|
|
|
Root Fracture Post RCT M
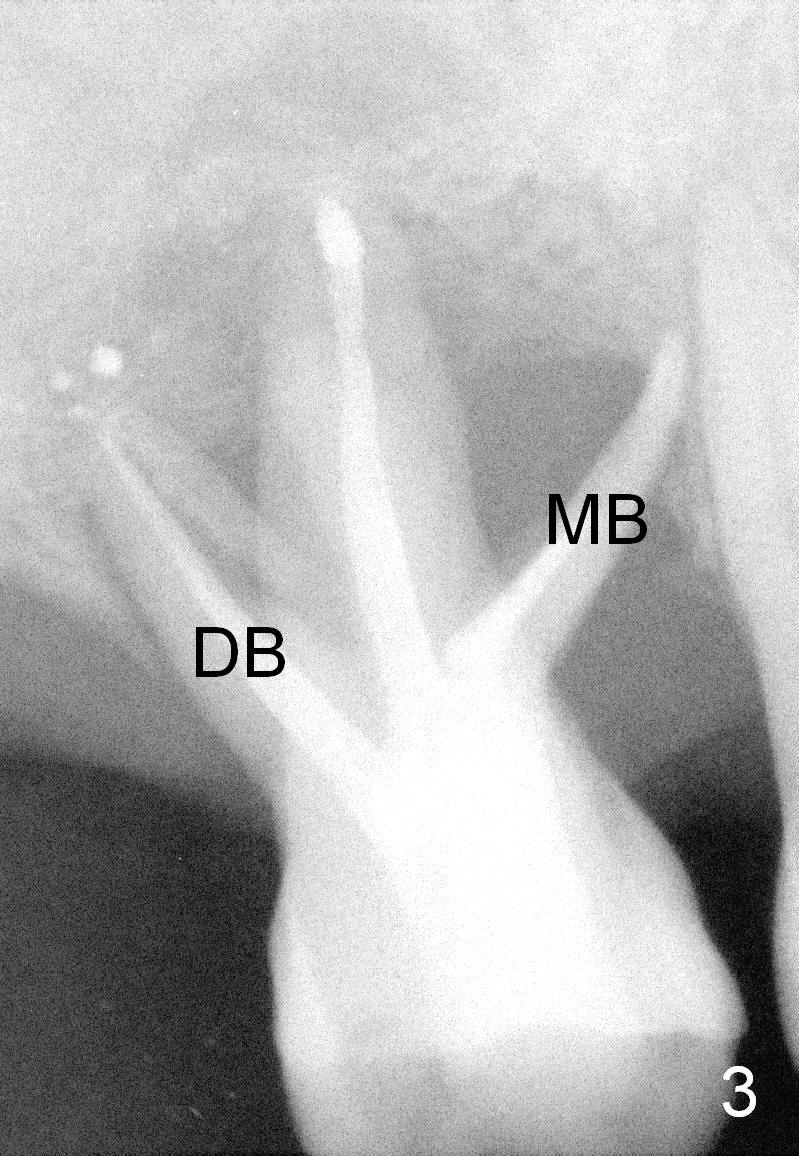
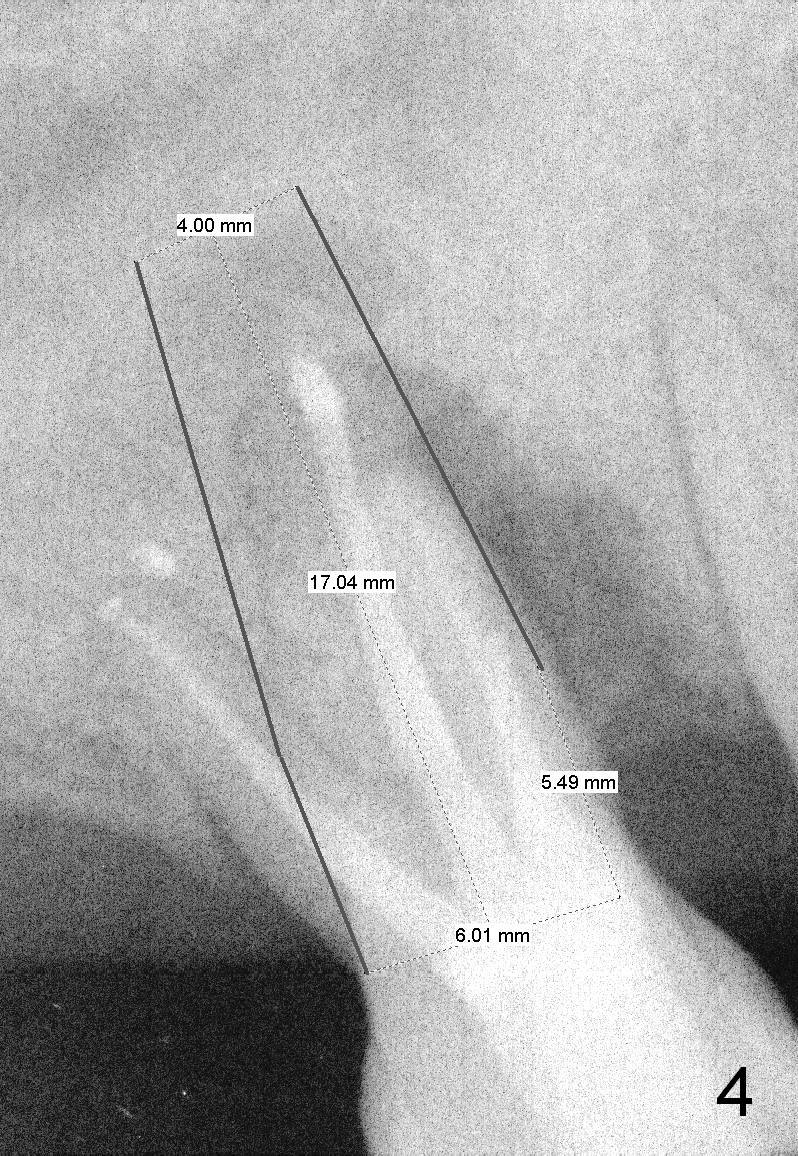
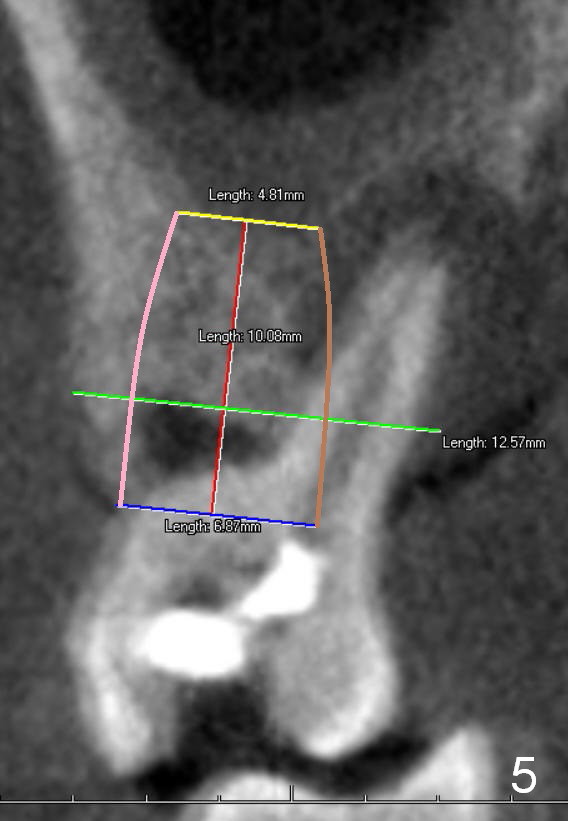
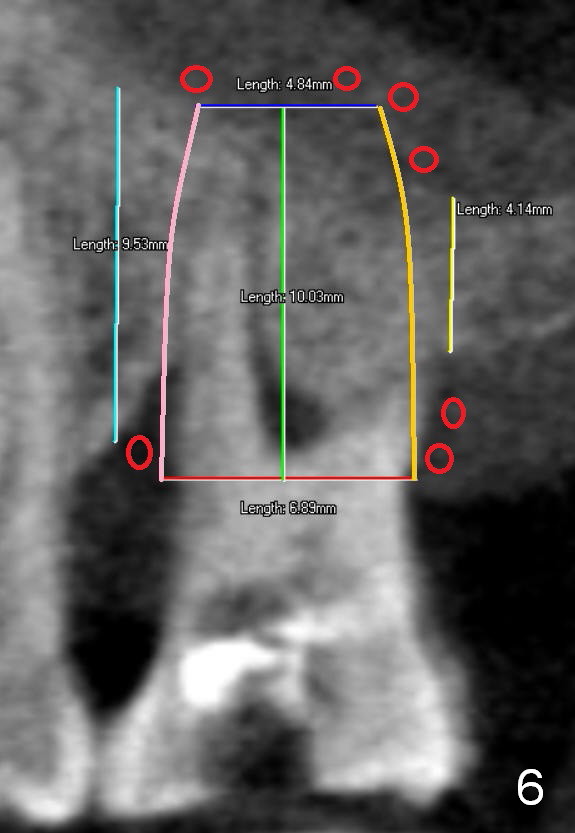
Two years post RCT, there is radiolucency around the MB root of the tooth #3 (Fig.1,2). Eleven days later, there is acute infection associated with MB and DB root fracture (Fig.3). According to the X-ray taken 11 days earlier (Fig.1,4), a long tissue-level implant (6x17 mm) is suitable for the site. In accordance with CBCT (coronal (Fig.5) and sagittal (Fig.6) sections) taken prior to RCT, a short bone-level implant (6.9x10 mm) is a more reasonable choice.
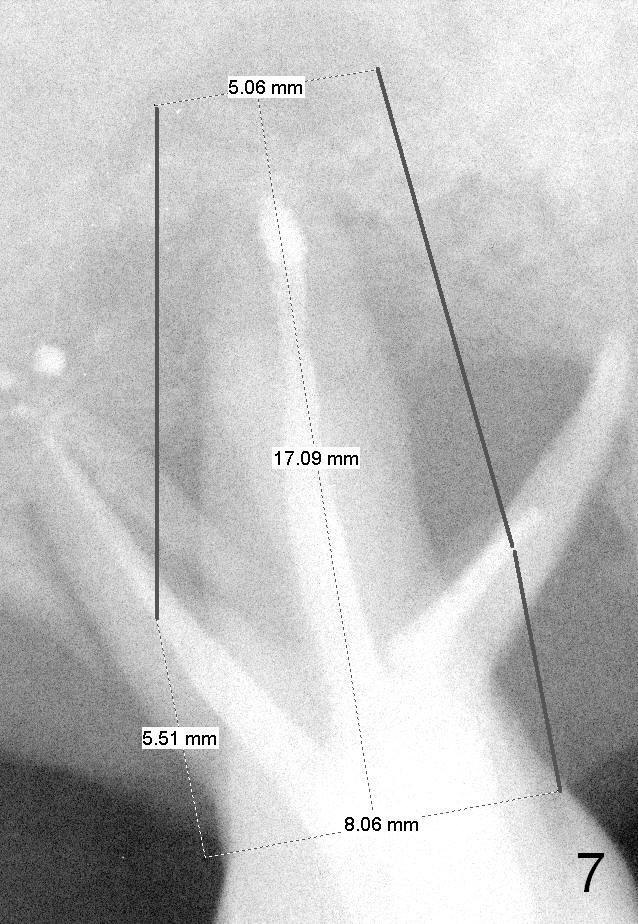
After extraction, the socket will be studied to determine where the bone is and where bony defects are for the site of the initial osteotomy. Start with 2 mm pilot drill or RT2, apparently ~ 6 mm depth, followed by reamers 2.5-3.5 mm and Tatum taps 4.5-7x17 mm (14 mm depth from gingival margin). Use a latch adapt with the torque wrench. Due to severe bone loss, the tap should not be too large (6 mm). If insertion torque is high and bone morphology is favorable, change to DIO taps and take necessary PAs to decide the length of the implant relative to the sinus floor and trajectory. If the depth is 10 mm or less, use SM; 12 mm UF. Based upon the most recent X-ray (Fig.3 with large lesion), the implant should be large and long (Fig.7: 7x17 mm).
Return to
Upper Molar Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 05/03/2015, last revision 12/26/2019