

|
|
|
|
|
|
|
|
|
|
|
|
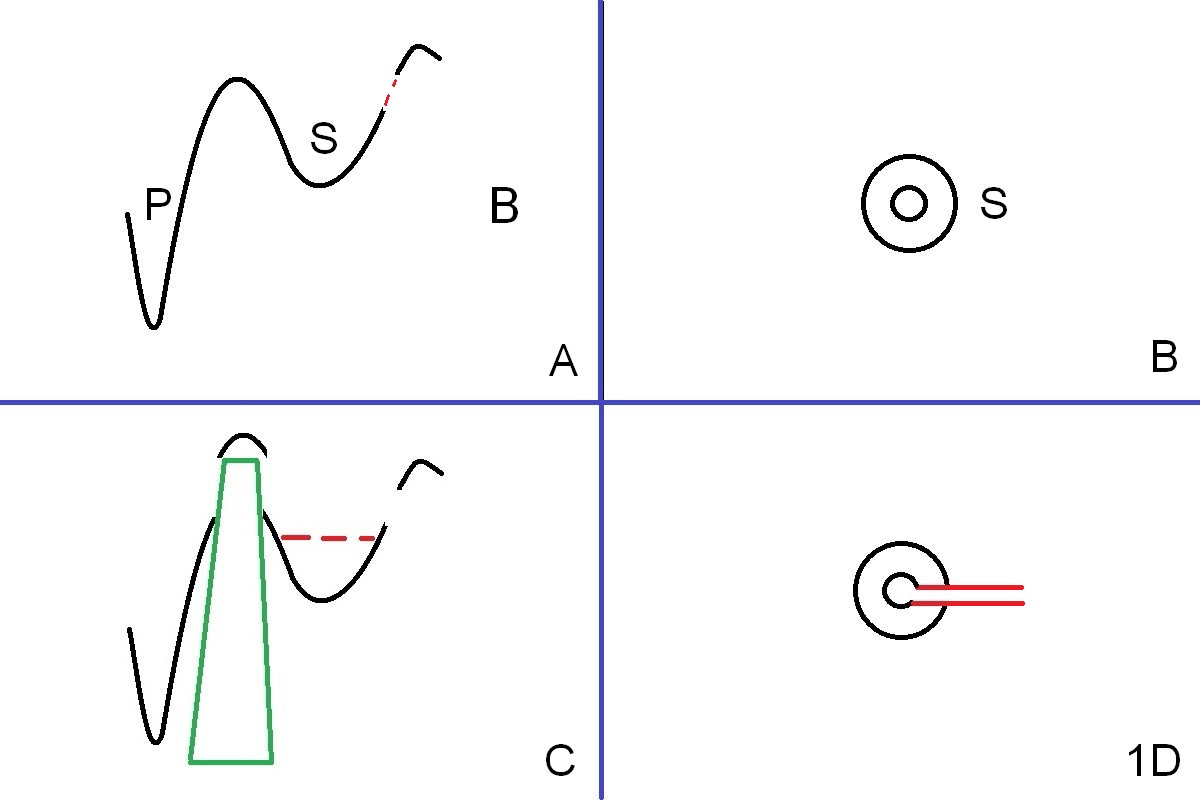
Change in Trajectory
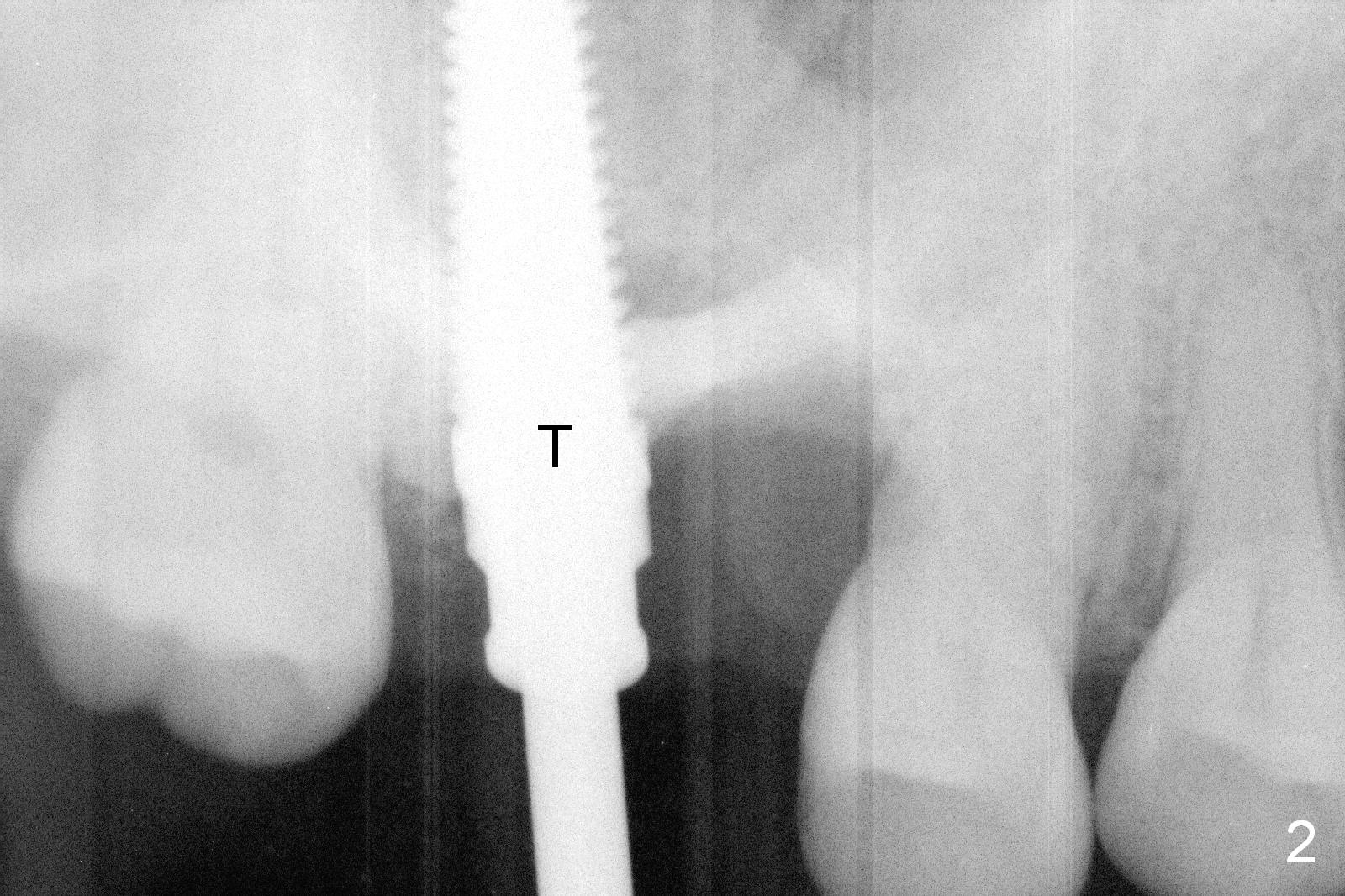
When the affected tooth is extracted, the buccal plate is lost (Fig.1A (coronal section): B). The septum is low (S), while the buccal slope of the septum is perforated (red dashed line). Therefore the palatal socket is the only suitable site for implant. Osteotomes (Fig.1C: green) are used to create osteotomy and sinus lift, followed by taps. Effort to direct the coronal end of the osteotomes and taps (Fig.2 T) in the middle of the socket fails. Fig.1B is the occlusal view of the palatal socket (2 circles) with the septum (S). To facilitate change in trajectory, Lindamann bur is used to make slot the buccal wall of the palatal socket and the septum (Fig.1C,D red lines).
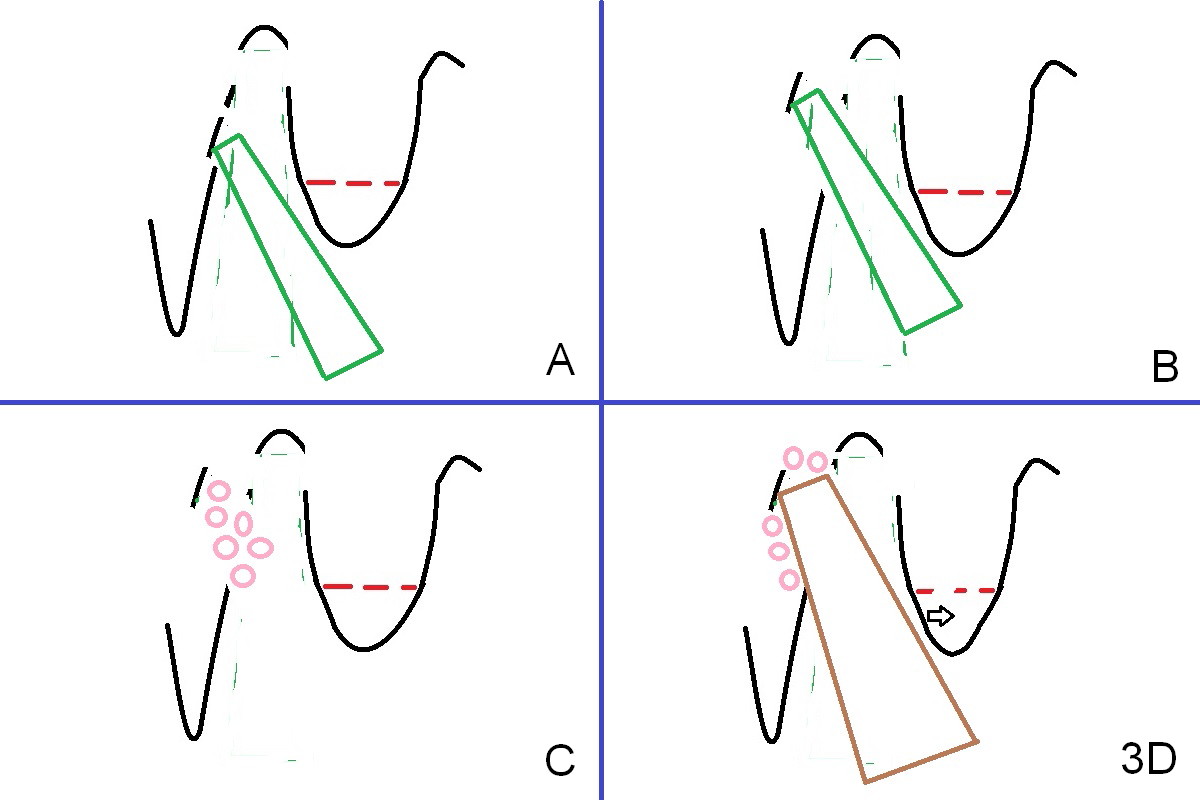
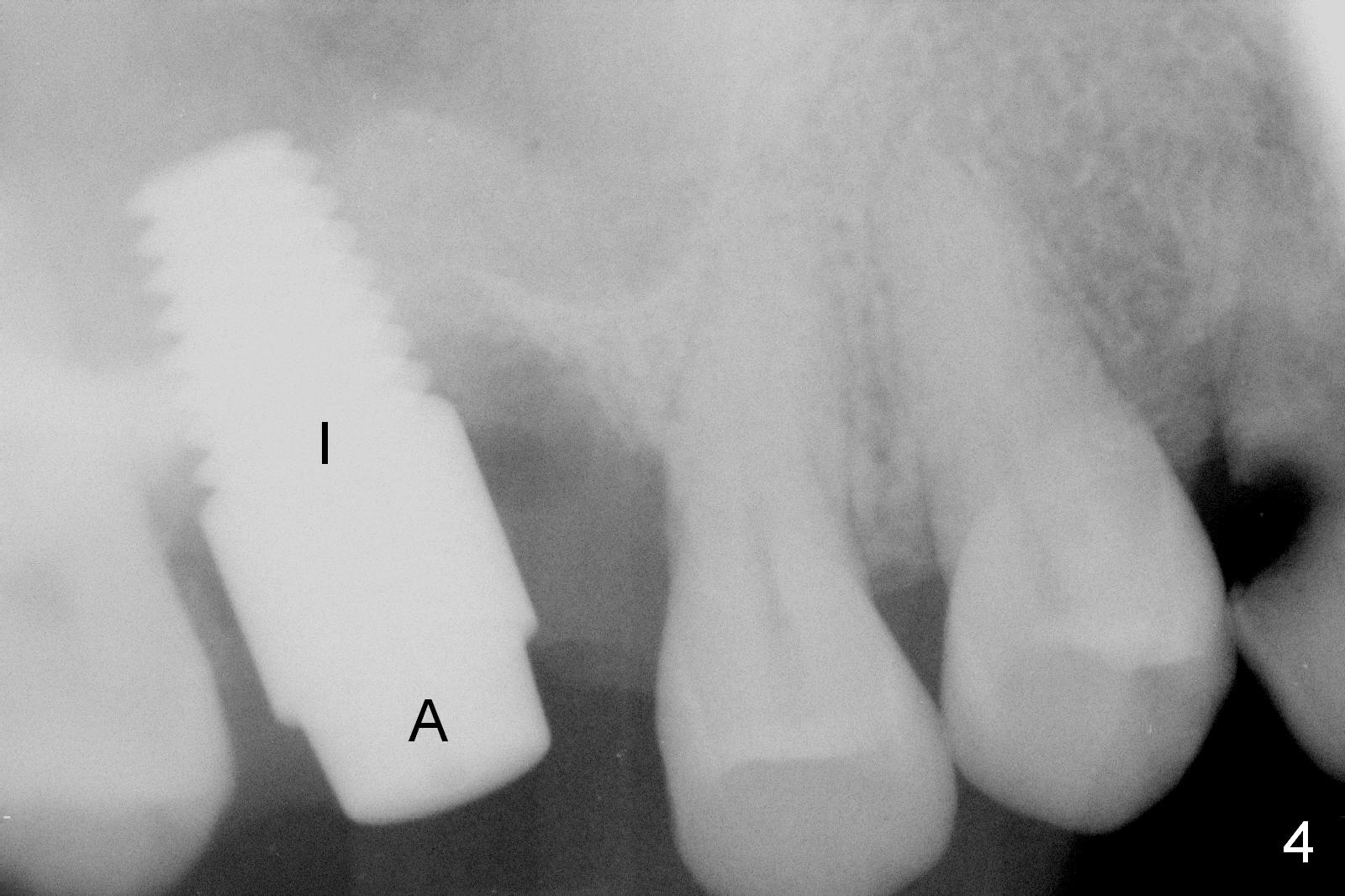
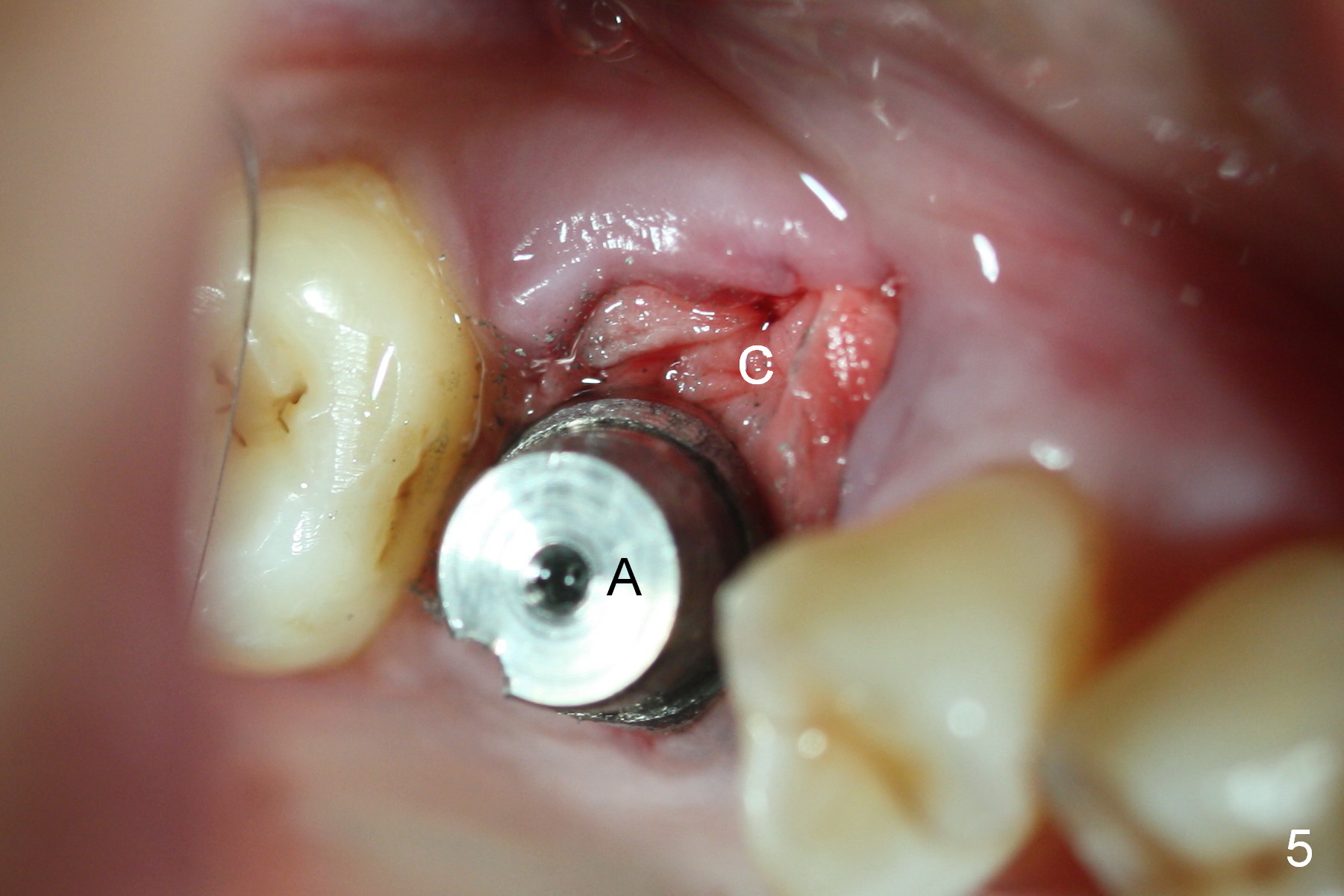
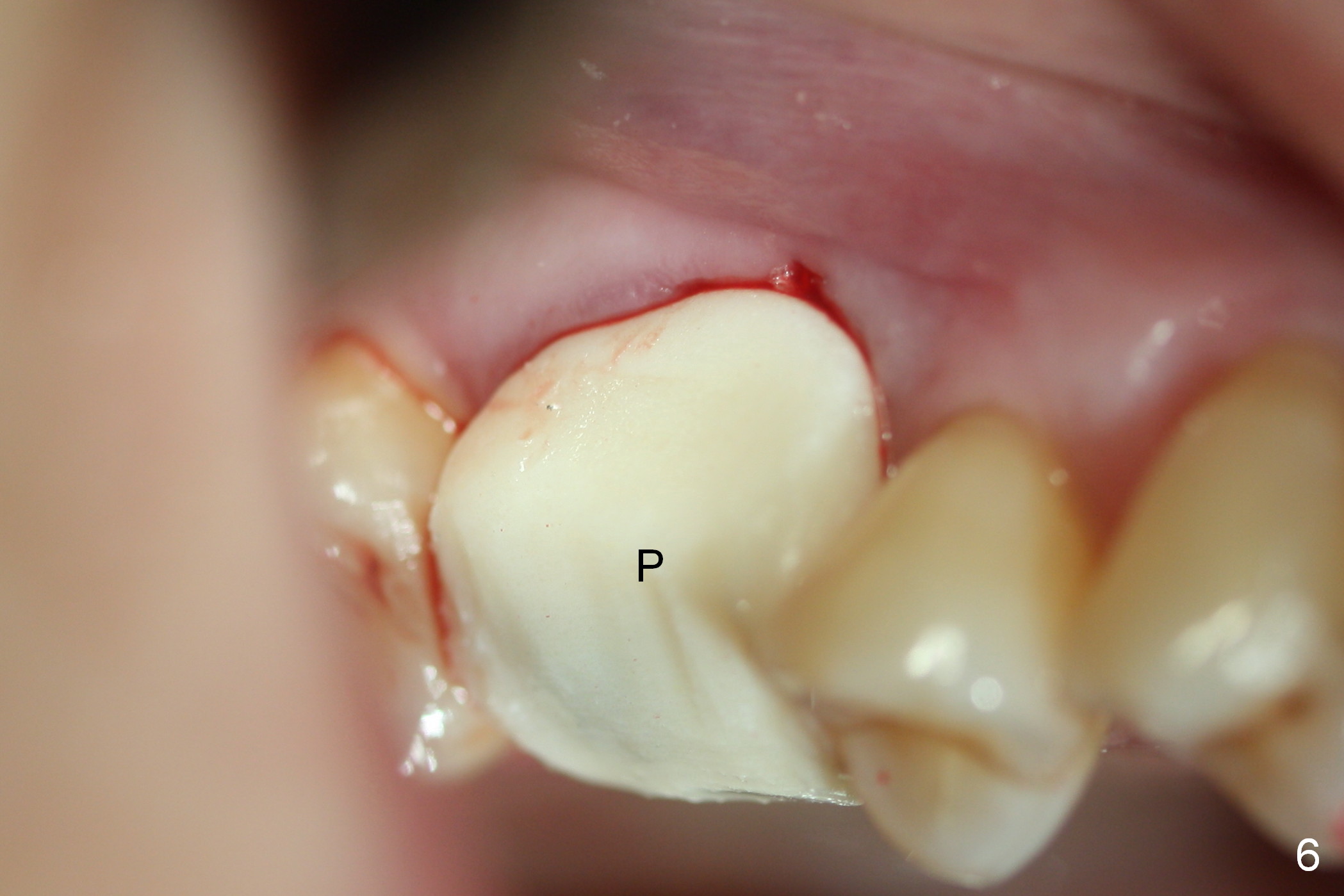
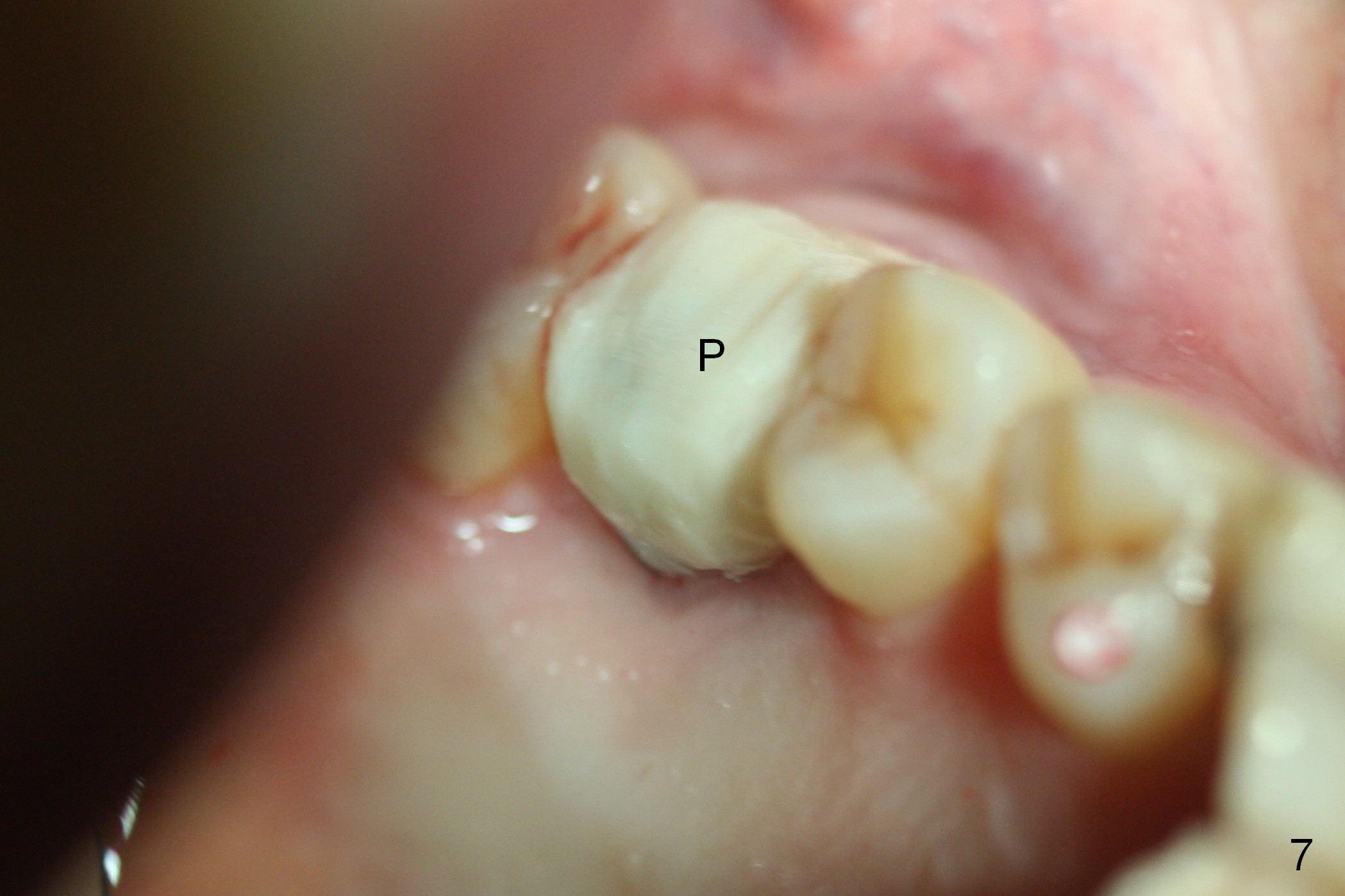
When a new osteotomy is formed in the palatal wall of the palatal socket (Fig.3 A, B), it is possible to control the coronal end of the osteotomes in the middle of the extraction socket. Although a 6 mm tap has achieved enough stability, a 7 mm tap is inserted, since the socket seems to be extremely large. Nose blowing test is performed after each step of osteotomy. Bone graft is placed in the osteotomy (Fig.3C: pink circles) before placing a 7x14 mm implant (Fig.3D: brown; Fig.4 I). A 6x3 mm abutment (Fig.4,5 A) appears in a proper position for restoration. After placing bone graft and collagen membrane (Fig.5 C), an immediate provisional is fabricated to keep the graft and membrane in place (Fig.6 P). Once again, Fig.7 shows the appropriate position of the provisional over the implant and abutment. Light nasal hemorrhage occurs a few hours postop, probably due to over-insertion of the tap (Fig.2).
When the patient returns for the definitive restoration 3.5 months postop, the immediate provisional has partially fractured. There is bone growth in the mesial socket (Fig.8 *). The buccal plate collapse seems to be minimal (Fig.9*). Six months post cementation at #3, the patient is pleased for mastication with the new implant crown and plans to convert the lower RPD into implant restoration (#20, 25, 26, 28, 29).
Return to
Upper Molar Immediate Implant,
Posterior Immediate Provisional
Buccal Root Exposure
Xin Wei, DDS, PhD, MS 1st edition 10/29/2015, last revision 12/25/2018