
,%20later%20(5).jpg)

|
|
|
|
||
|
|
|
|
|
|
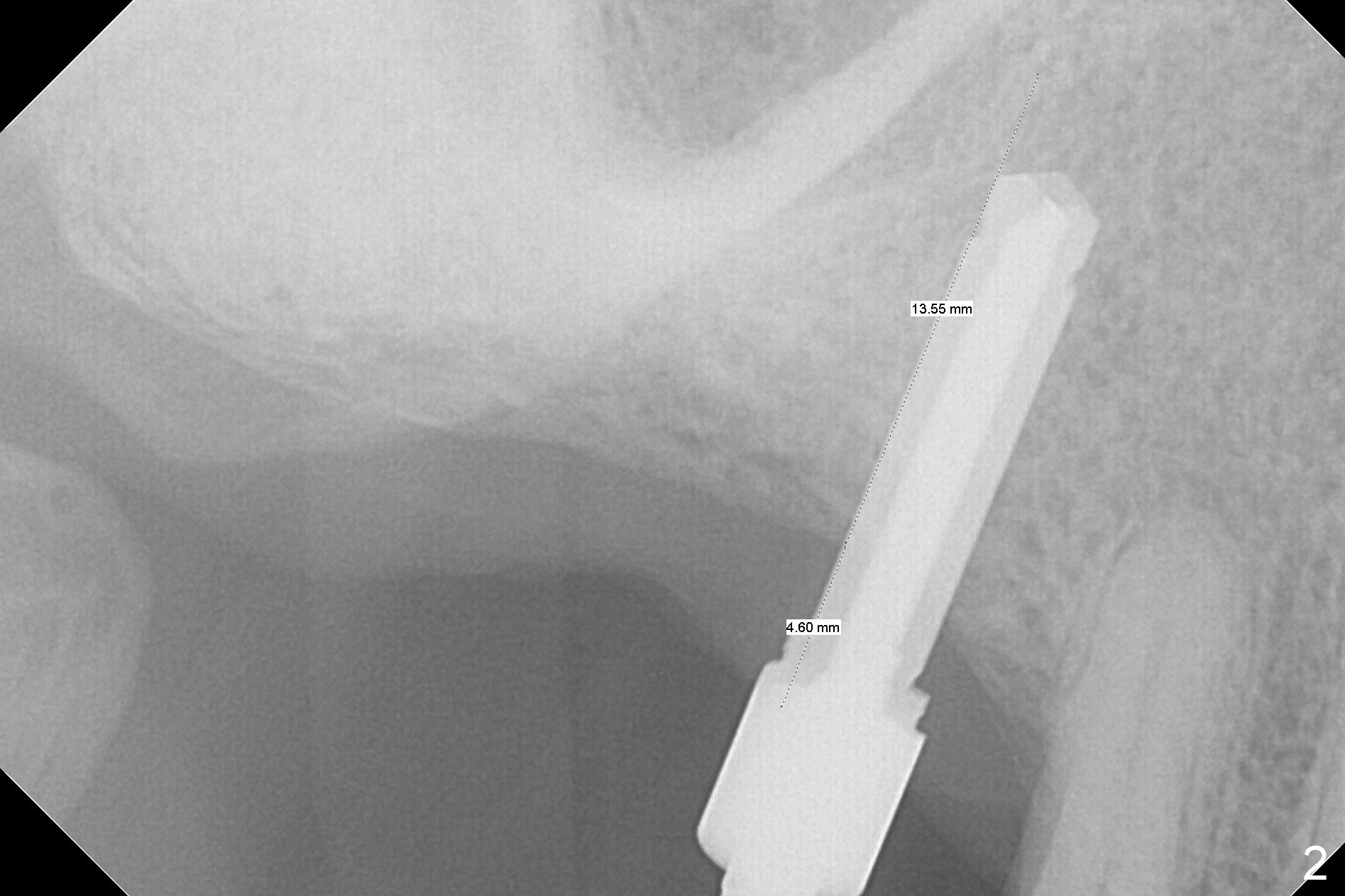
Bone Expansion Alternates with Drill
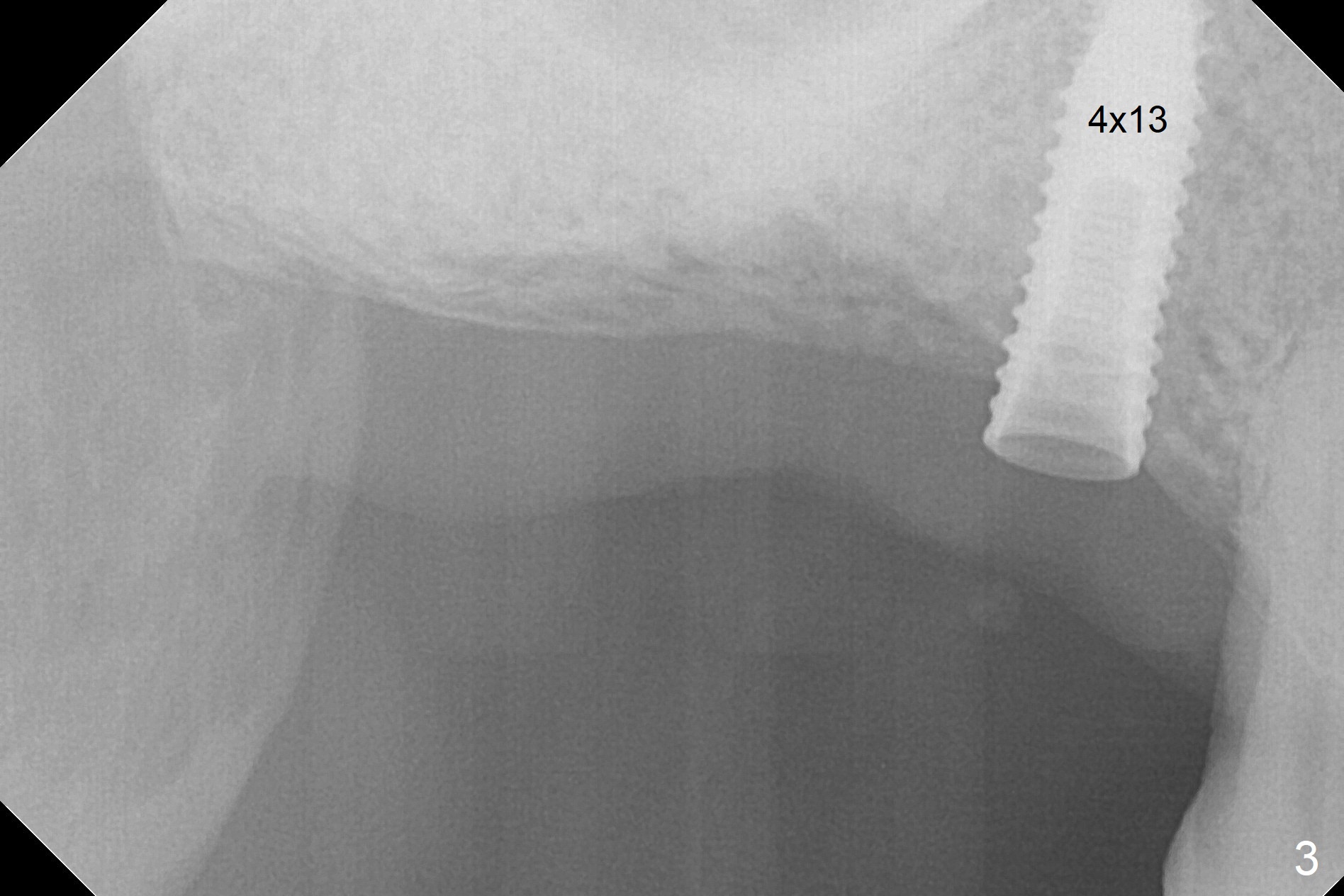
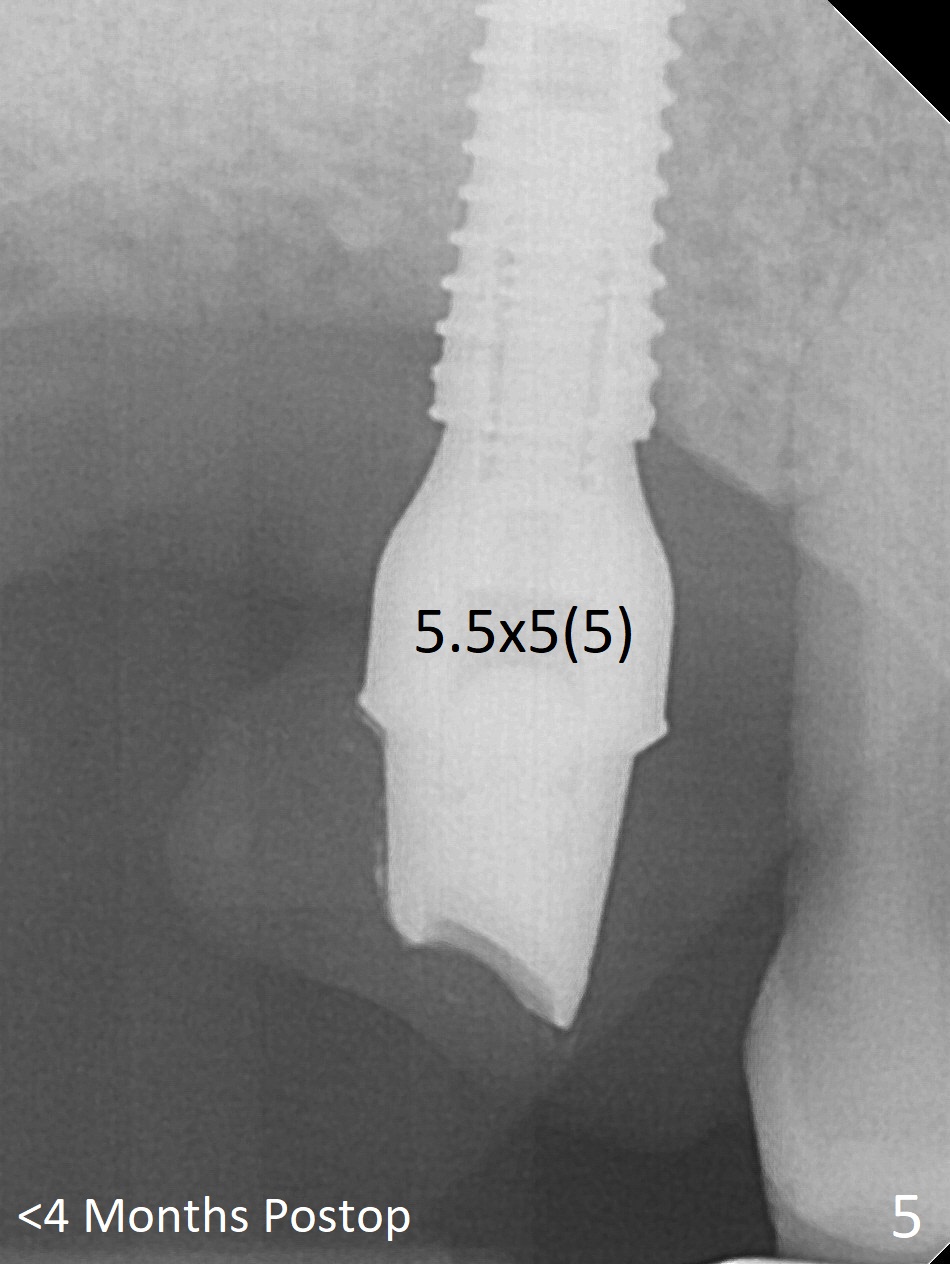
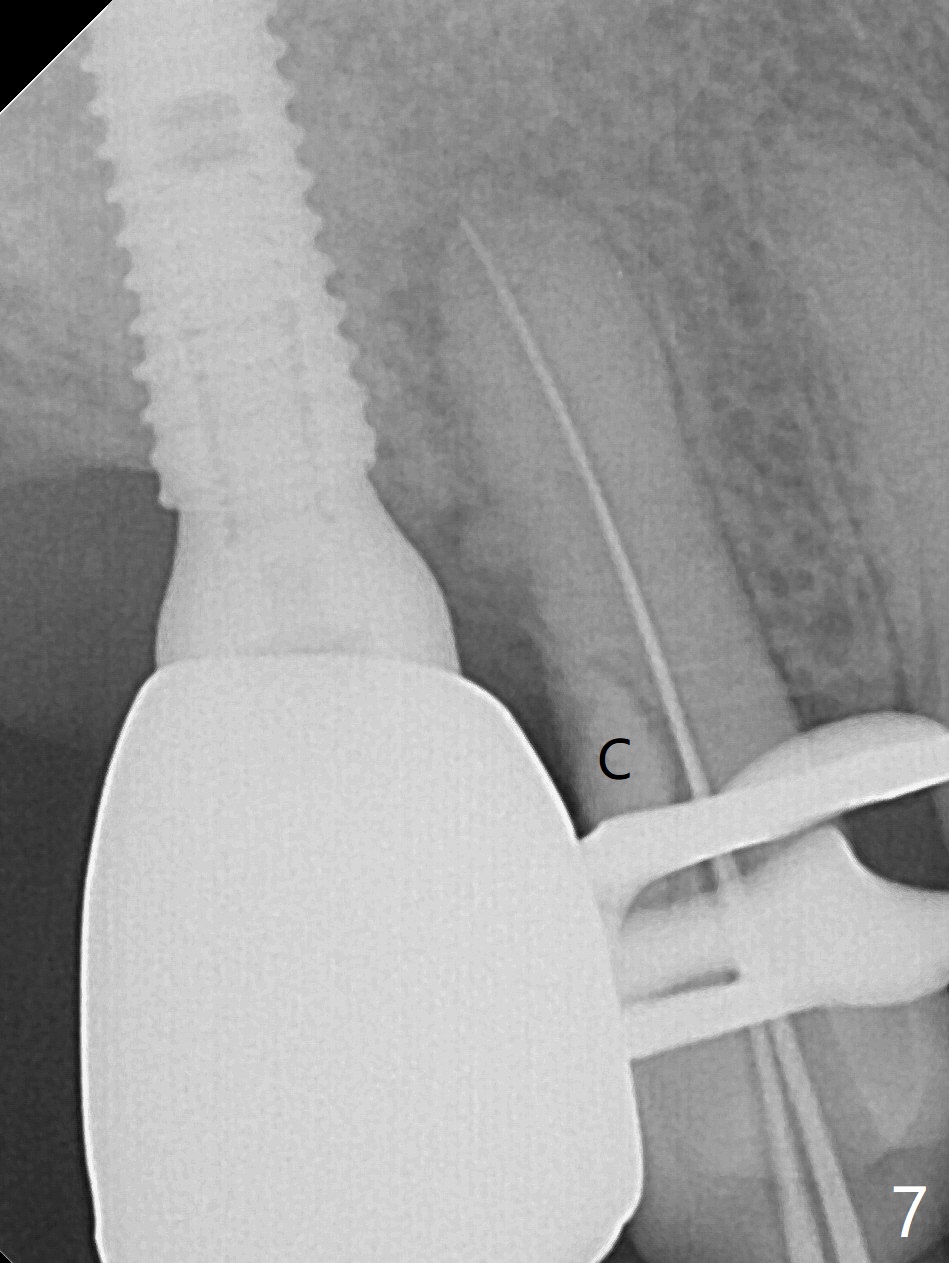
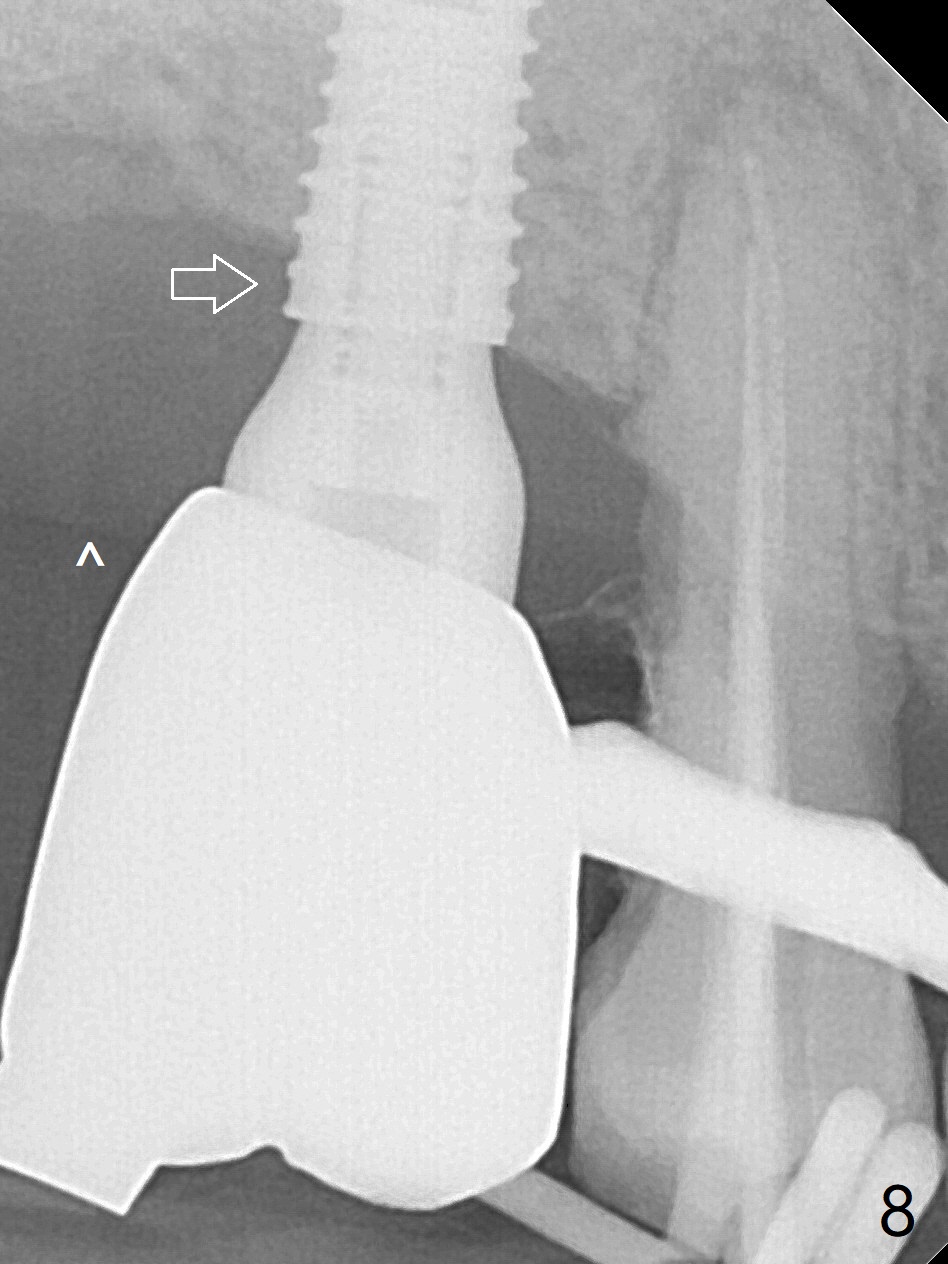
Since the ridge crest at #3 is narrow, Tatum bone scalpels are used to get access and initiate bone expansion, followed by bone blades and RT 2. It seems that the osteotomy starts mesially; bone height being increased (Fig.1). When the apical end of the osteotomy tilts mesially, more bone height is obtained. Drills are alternatively applied because of the hard bone (Fig.2). A 4x13 mm UF implant is placed initially with the distal threads unburied (Fig.3, >50 Ncm). With further seating of the implant, a 5.5x5(4) mm abutment is used (Fig.4), which closes the access. No suture is warranted. An immediate provisional is fabricated for the patient's comfort and psychological effect. In fact, the abutment cuff changes to 5 mm prior to temporarization. There appears no bone loss <4 months postop (Fig.5). Pulpitis develops at #4 due to DO caries 1 year 5 months post cementation (Fig.6 *). The crown at #3 is removed for easy and conservative distal carious removal and Cavit temporary restoration to prevent sodium hypochlorite leakage. Then occlusal access is made for pulpotomy. When RCT finishes, no crown will be made, but occlusal reduction is required. The patient returns for RCT 1 month later (Fig.7,8). Cavit remains in place (Fig.7 C). Although 2 threads are exposed distal (Fig.8 arrow), there is no sign or symptom of periimplantitis, which may be related to the thick gingiva (arrowhead). Return to Upper Molar Immediate Implant, IBS, #14 (Tissue Punch) Xin Wei, DDS, PhD, MS 1st edition 08/25/2017, last revision 09/08/2019