|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|||||
Soft Bone-Bone Expanders
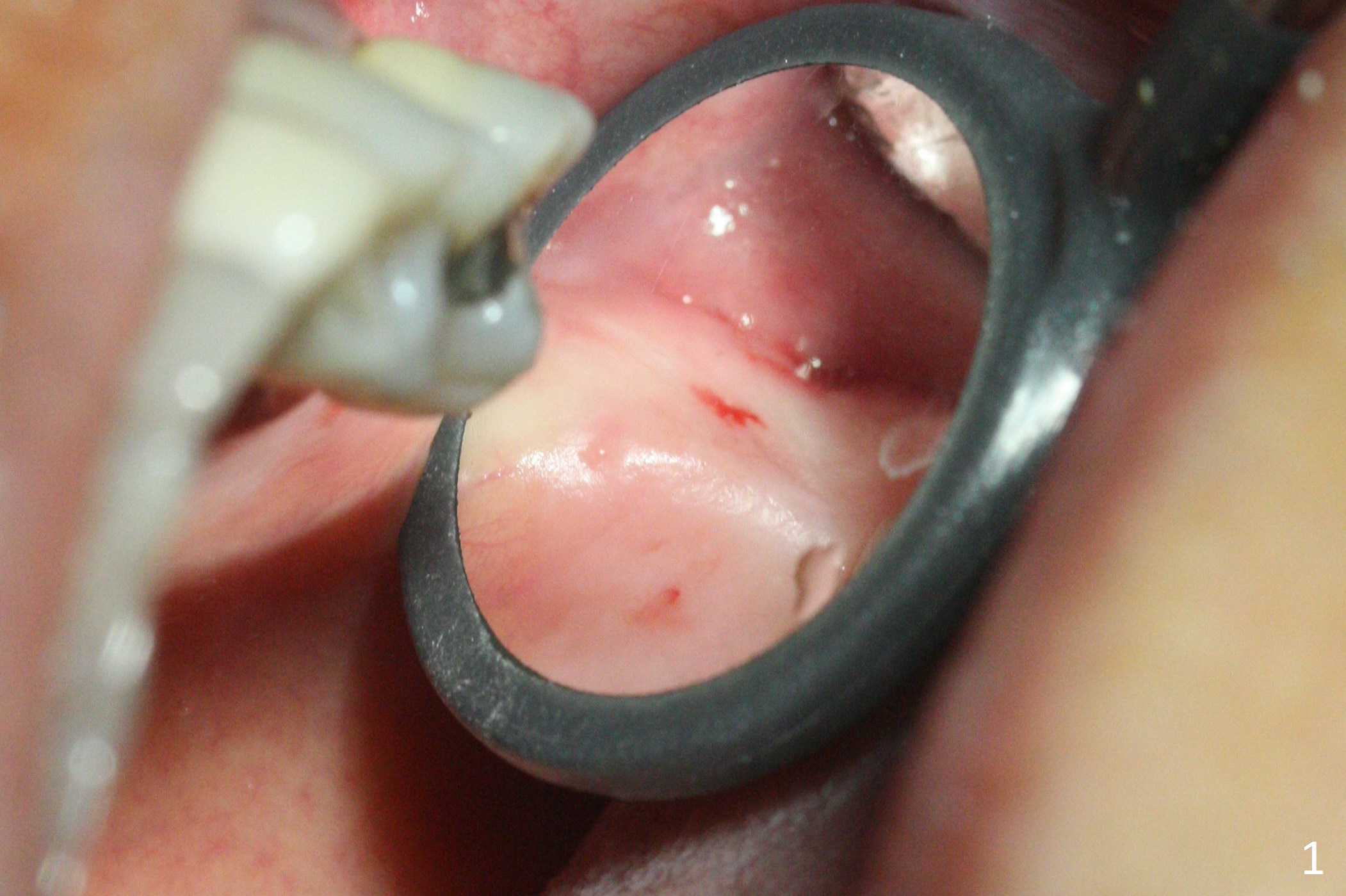
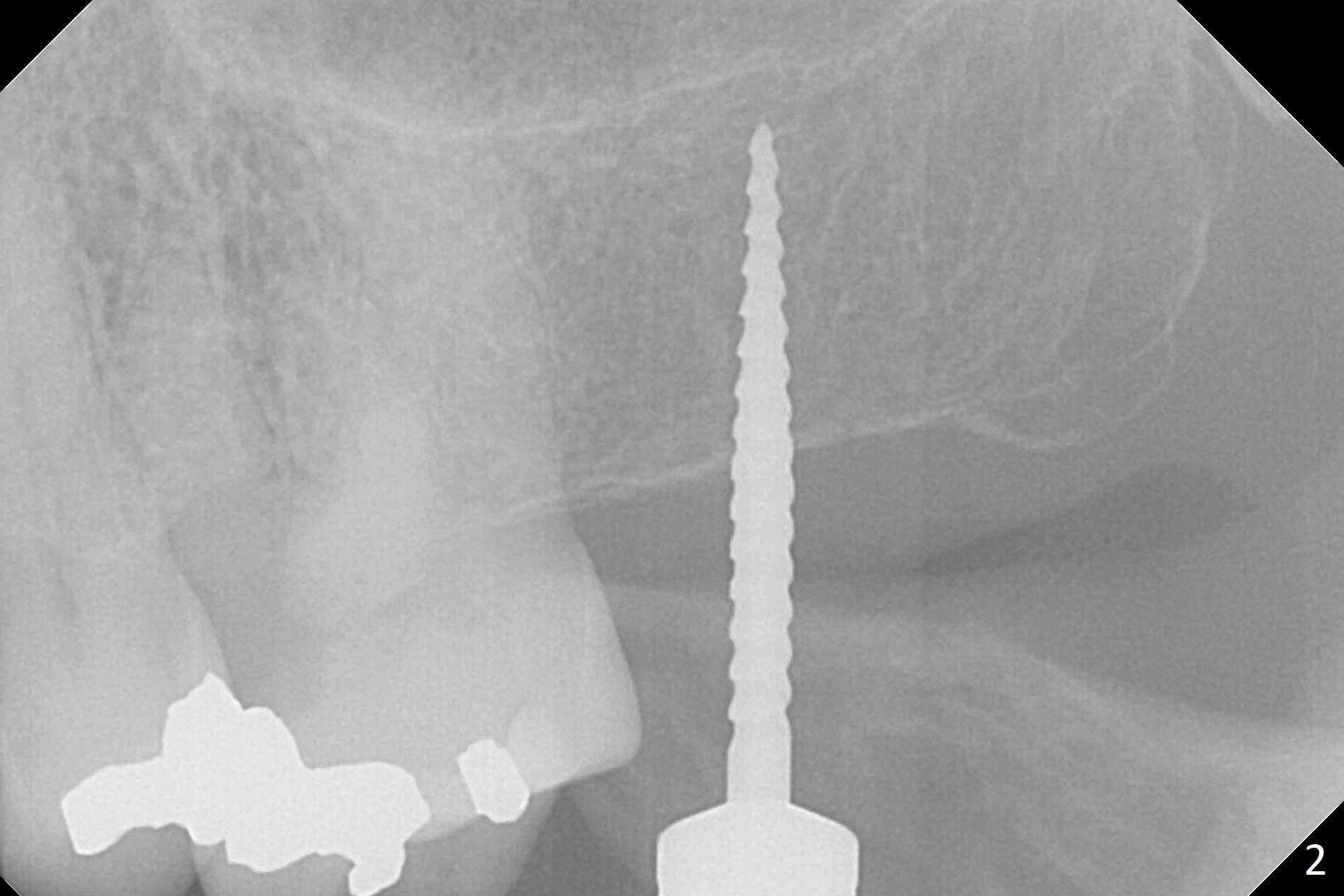
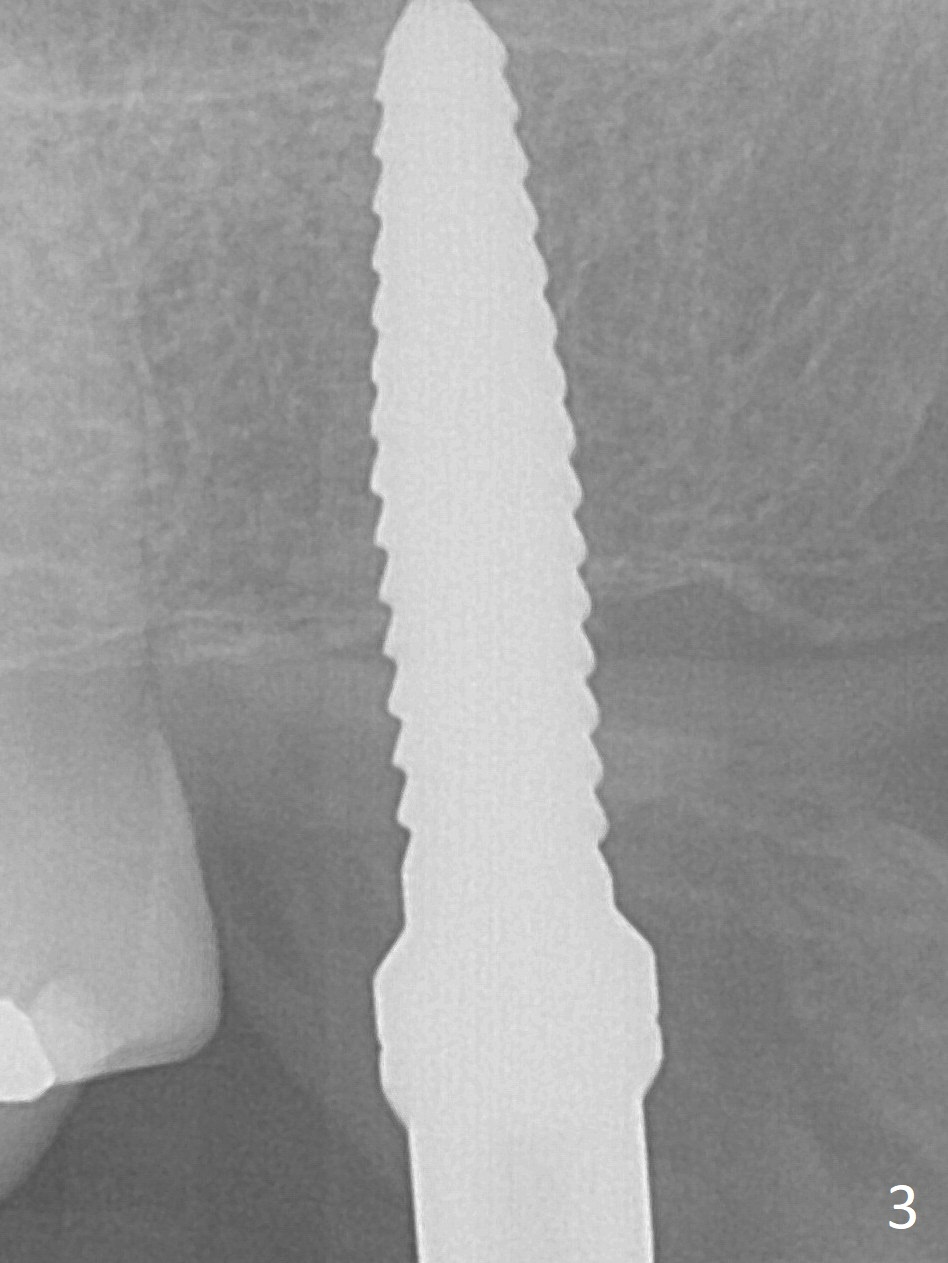
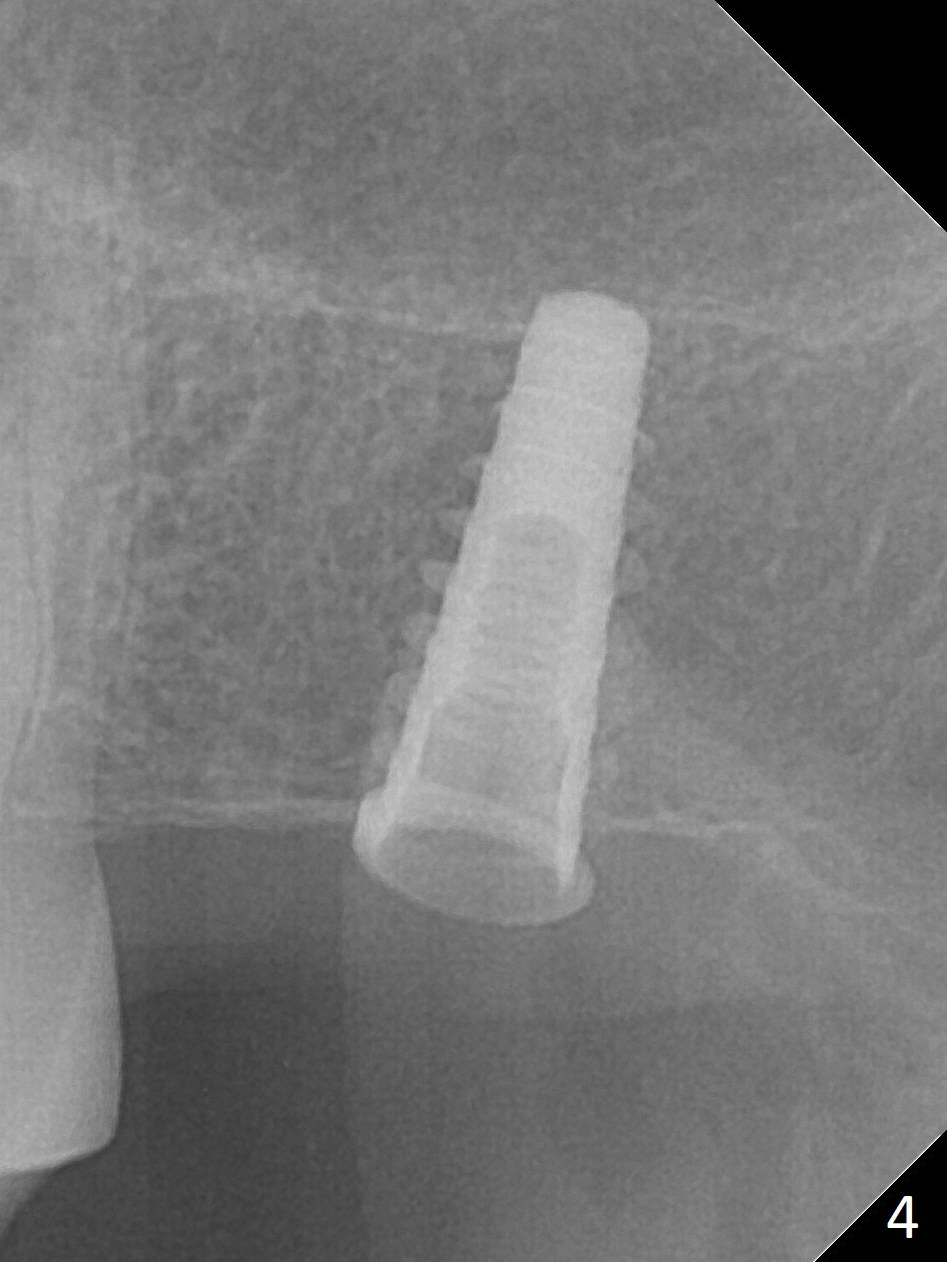
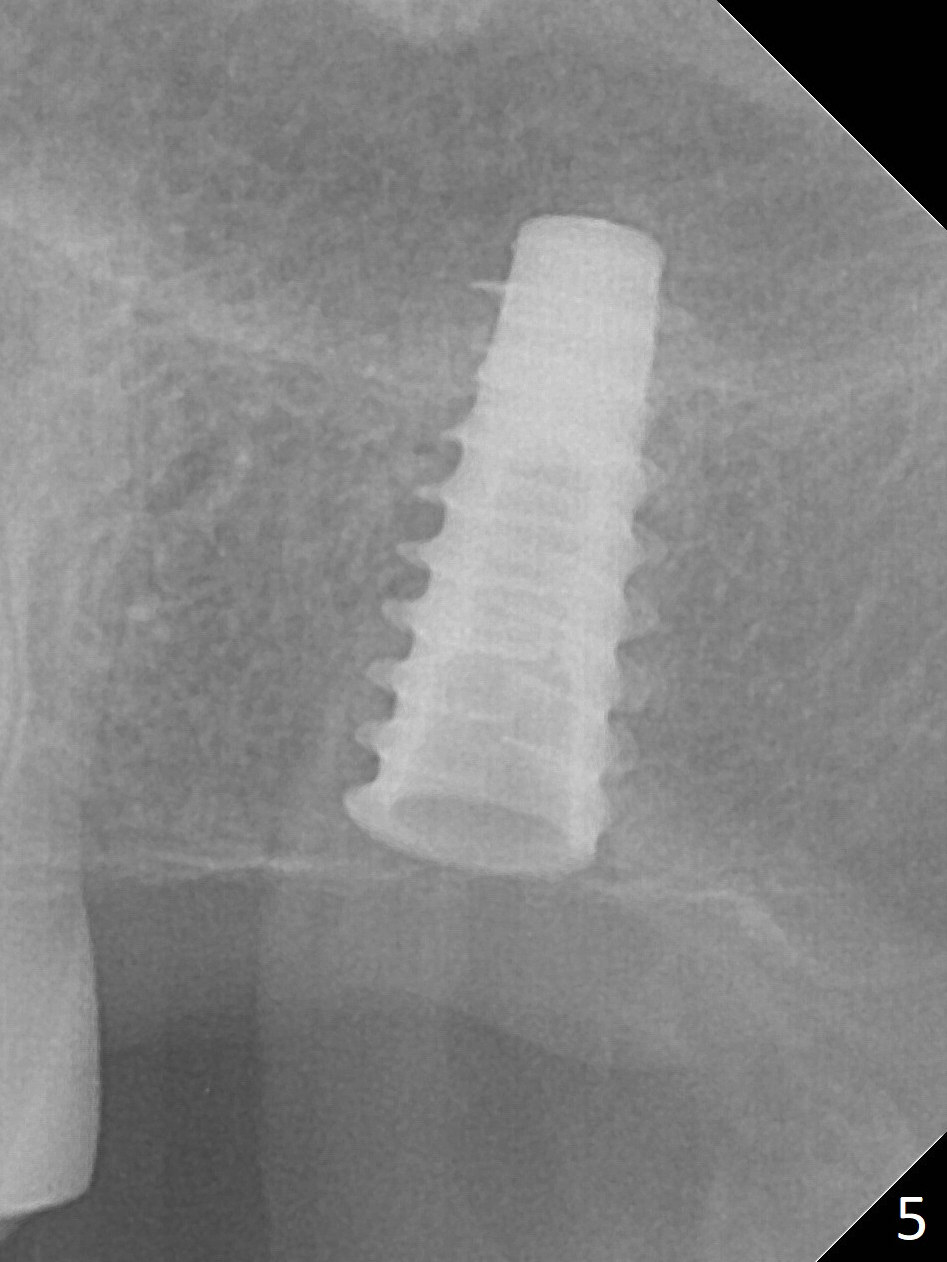
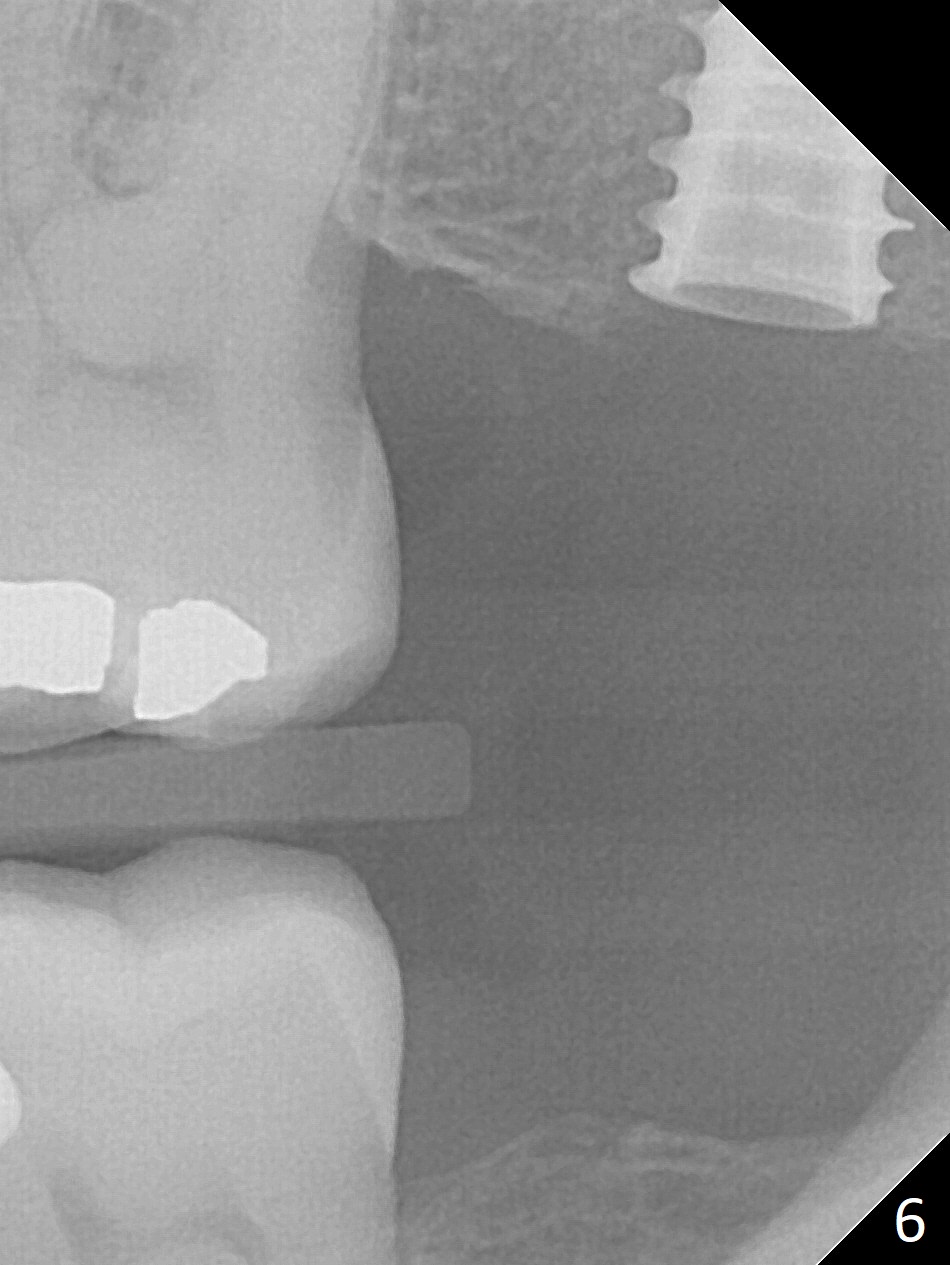
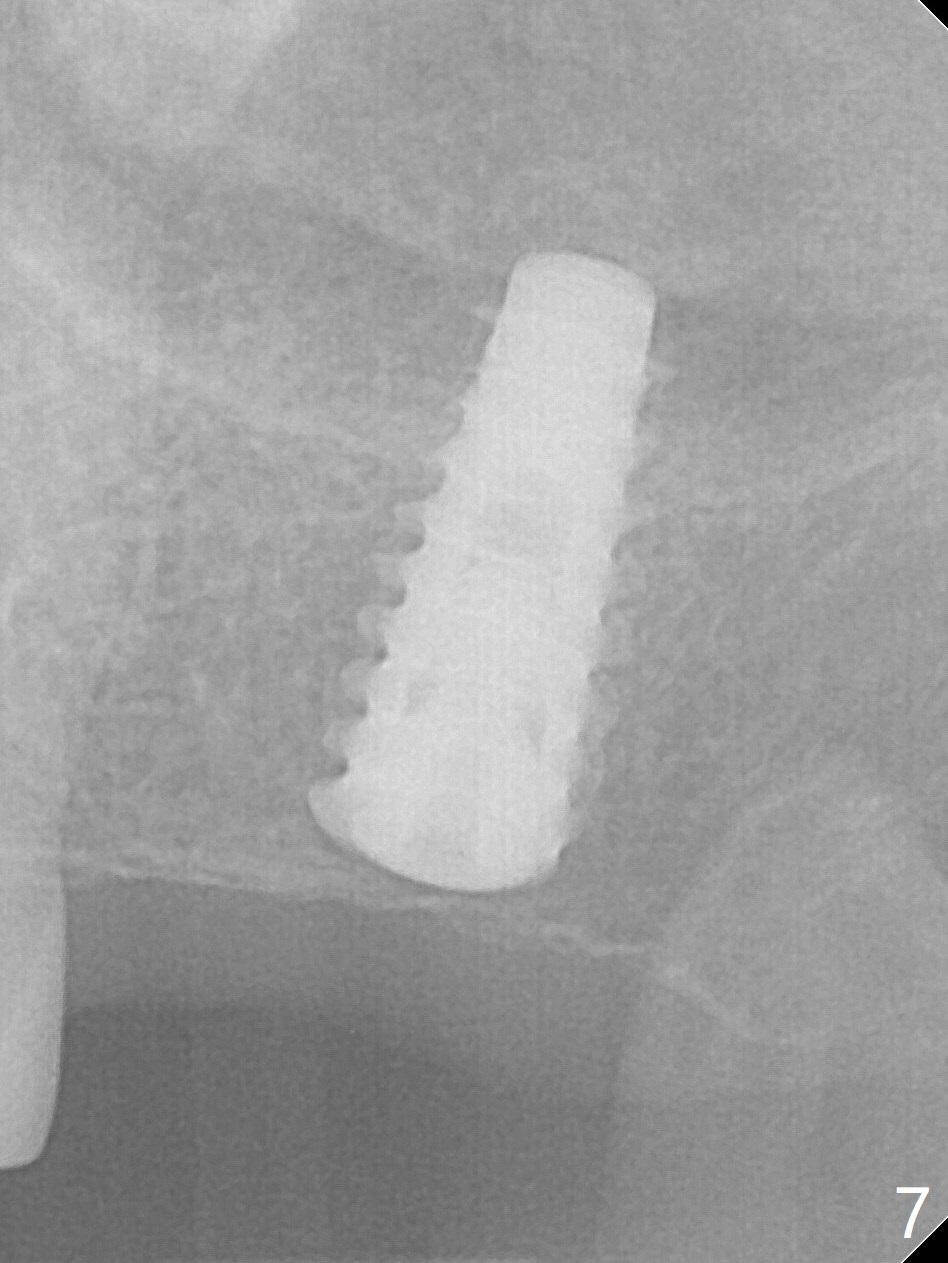
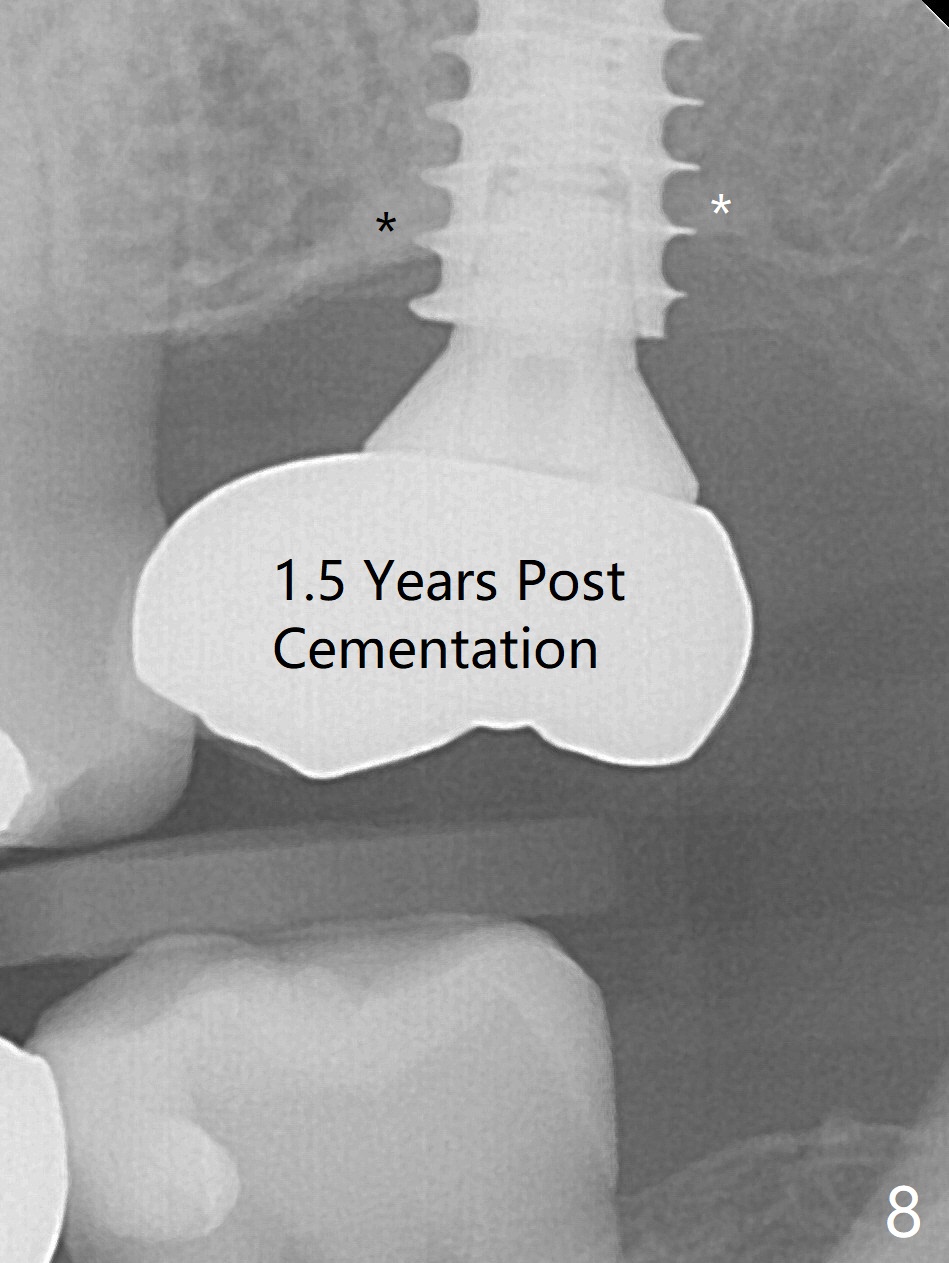
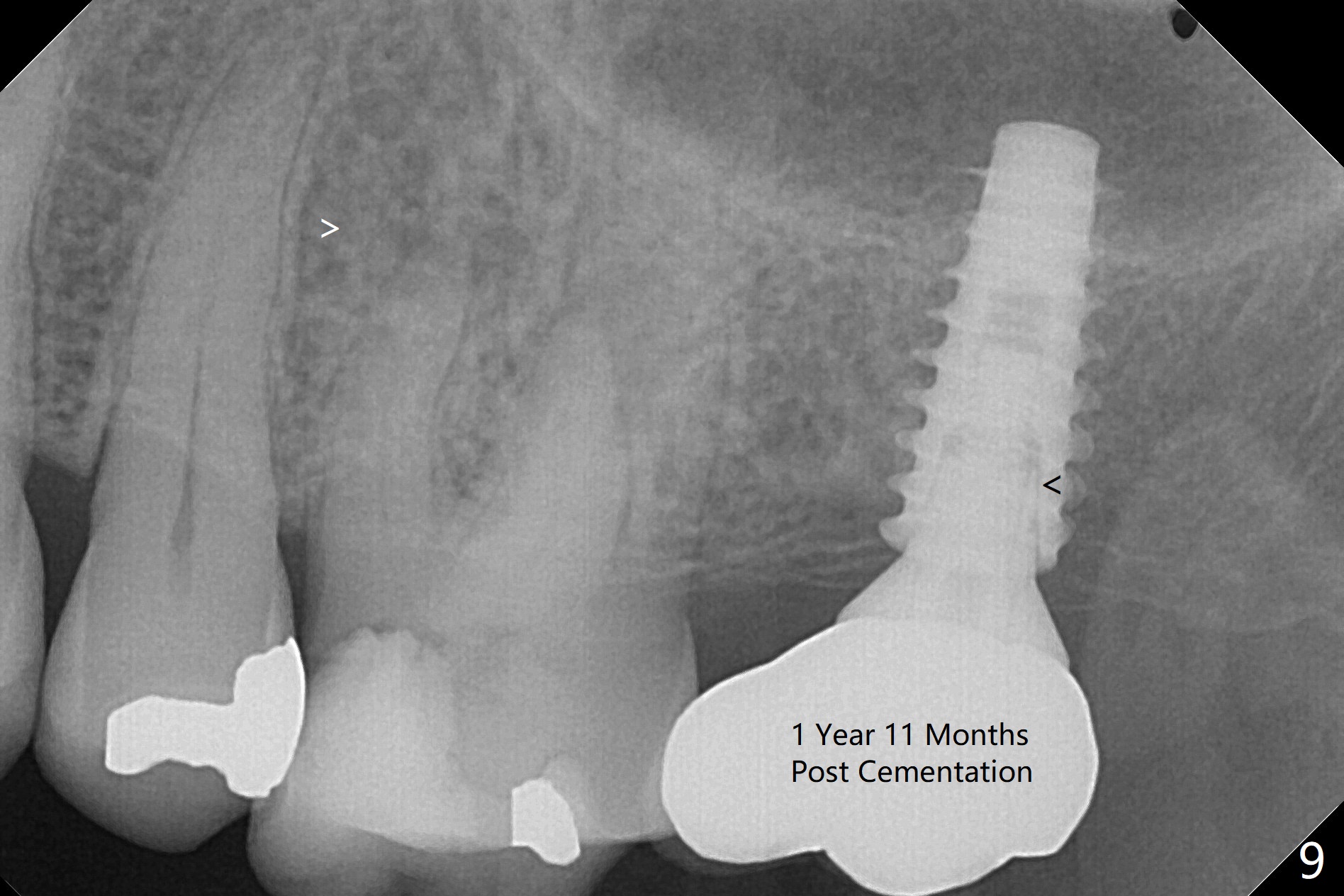
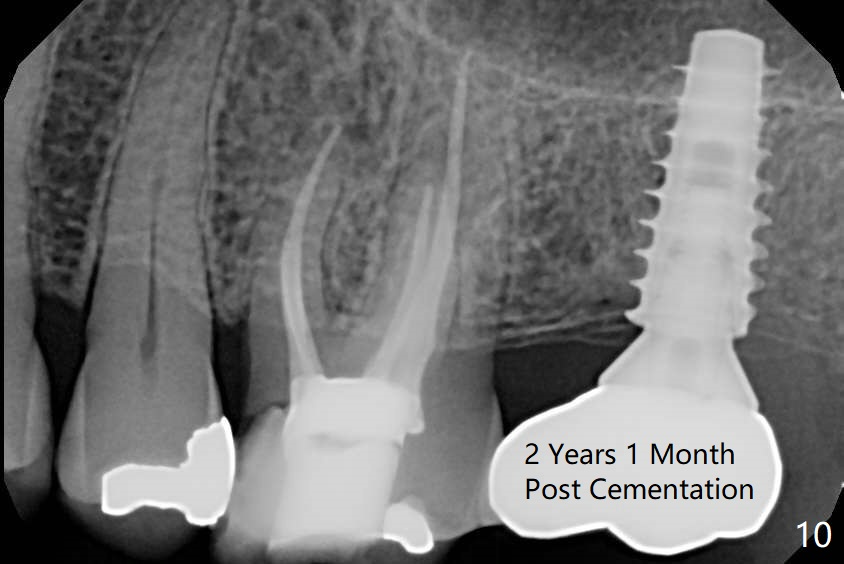
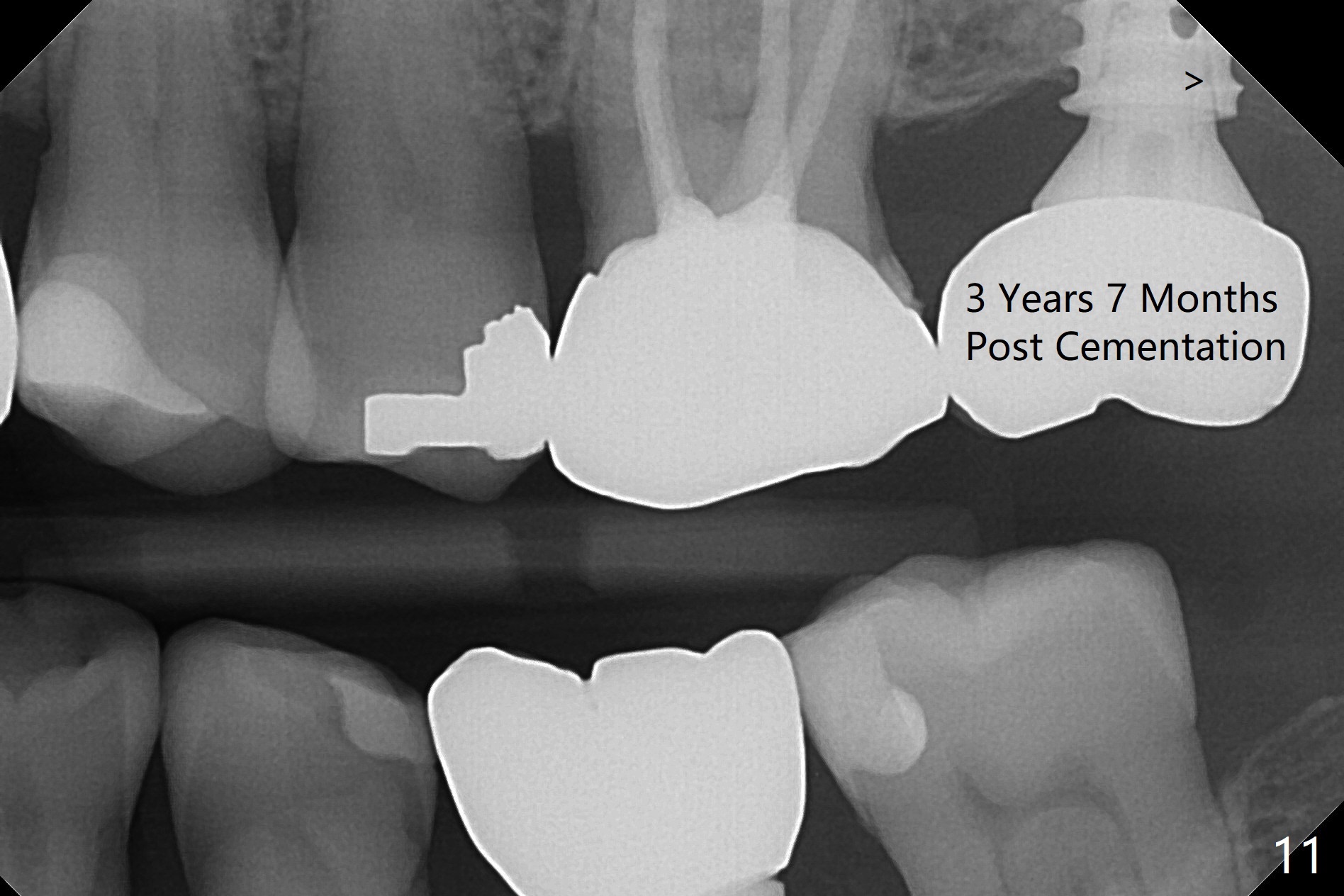
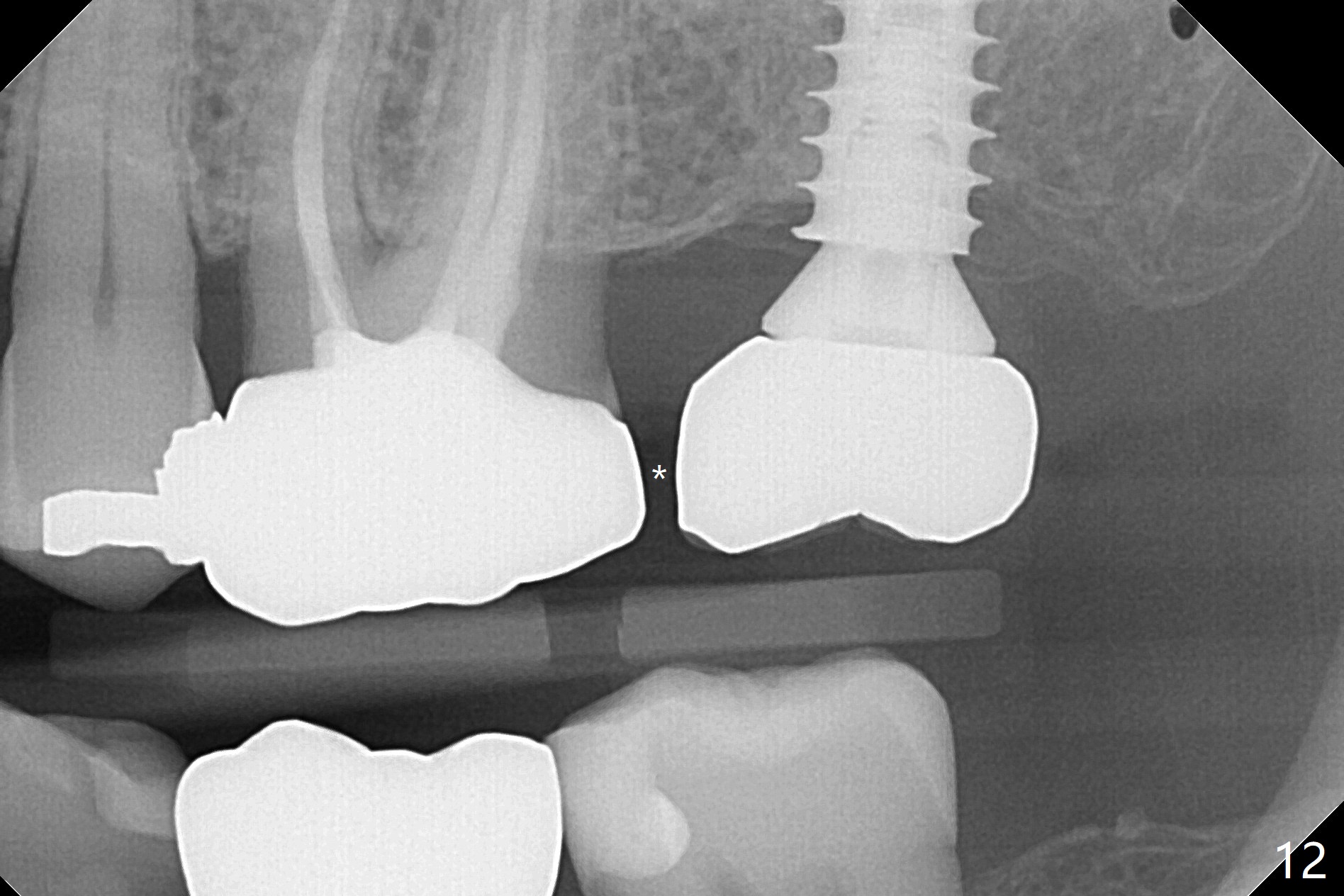
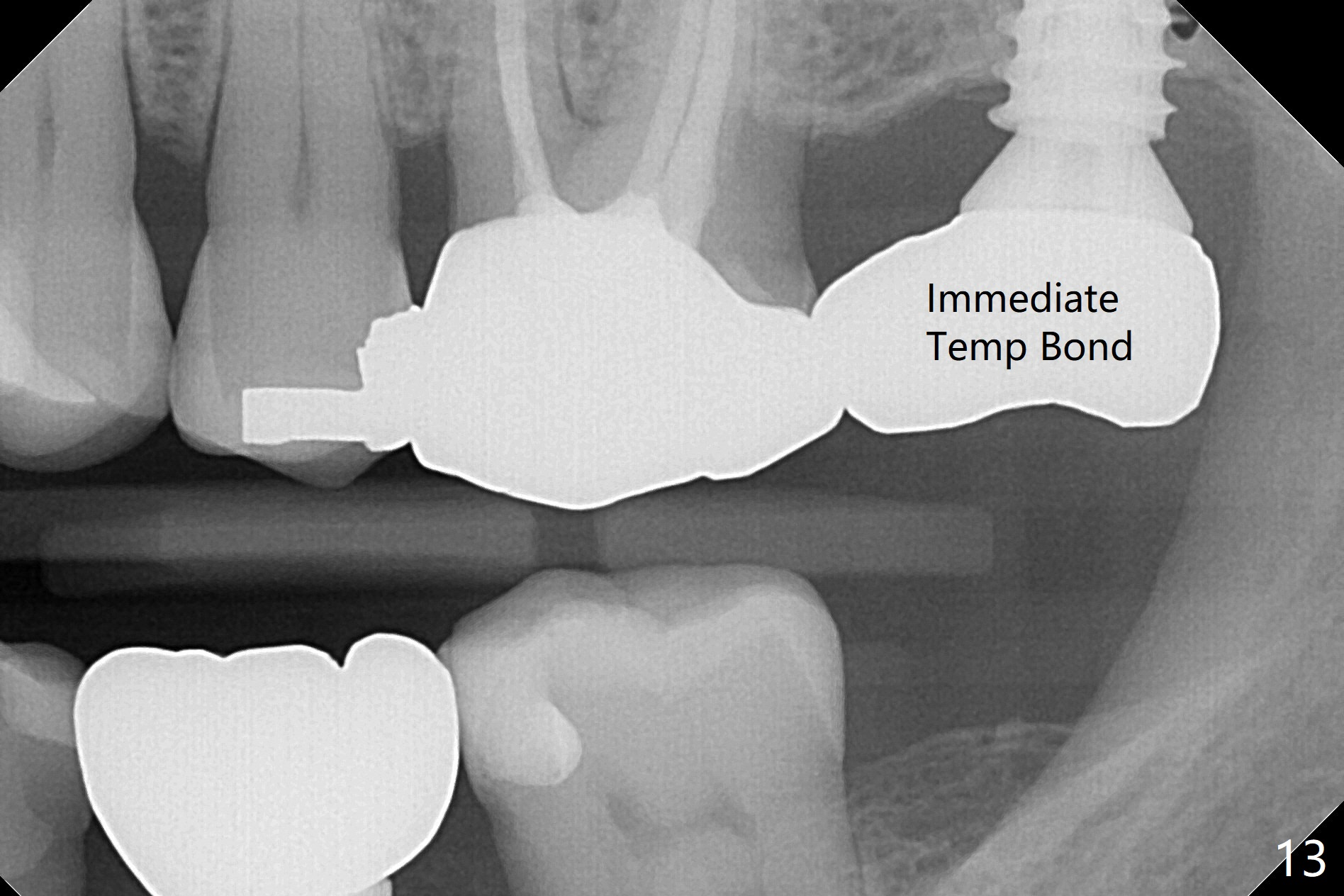
The ridge is pointed at the site of #15 (Fig.1). A 1.2 mm initial drill is used to start osteotomy for 10 mm, followed by an incision over the ridge mesiodistally for ~ 8 mm. After tapping the #15 C blade, the 1st Bone Expander 1.0/1.6 mm) is inserted for ~ 11 mm (Fig.2, 20 Ncm). Bone expansion continues until #4 Expander (2.4/3.7 mm, Fig.3). When 4x11 mm and 4.5x11 mm dummy implants are placed (Fig.4), insertion torque remains 20 Ncm. Following placing allograft with 3-4 amalgam carriers, a 5x11 mm IBS implant is placed with 20 Ncm (Fig.5,6). In fact the implant turns when an abutment is placed. When the implant is re-inserted, torque decreases to 10 Ncm. Instead a healing screw is placed. The low torque value is due to soft bone and failure to underprep. #4 Expander (Fig.3) seems larger than 4.5 mm implant (Fig.4). #3 Expander (1.7/3.1 mm) should have been used prior to definitive implant placement. The implant appears to have osteointegrated 3 months postop (Fig.7); impression is taken. The bone density at the crest increases 1.5 years post cementation (Fig.8 *, as compared to Fig.6), although there is mild bone loss. Implant placement should be deep when bone expansion is carried out. The tooth #14 develops a buccal fistula, corresponding to periapical radiolucency of the mesiobuccal root (Fig.9 white >). The abutment of #15 may be incompletely seated (black <). PA taken when RCT of #14 is finished does not show the incomplete seating of the abutment (Fig.10). Since there appears no history of abutment screw loosening, the abutment is not reseated when #14 is prepared for crown. Recall 3 years 7 months post cementation shows incomplete seating of the abutment (Fig.11 >). After crown proximal reduction (Fig.12 *) and clockwise turn of the crown, the abutment appears to be completely seated. When the case returns from lab, the separate crown and abutment cannot be connected to the fixture because of soft tissue adaptation and change in a month. The abutment is reseated to the fixture analog in the model and the crown is recemented with temp bond (in case of misalignment) while making sure that the crown has the best proximal contact with the neighboring crown. With the abutment and crown in a unit, it is much easier to reseat the abutment with normal proximal contact. The torque is 20 Ncm. The access hole is closed with Cavit.
Return to Upper Molar Immediate Implant Torque
Xin Wei, DDS, PhD, MS 1st edition 06/26/2017, last revision 07/21/2021