
|
|
|
|
|
|
|
|
Immediate Implant (Moderate Size) in the Middle of the Socket
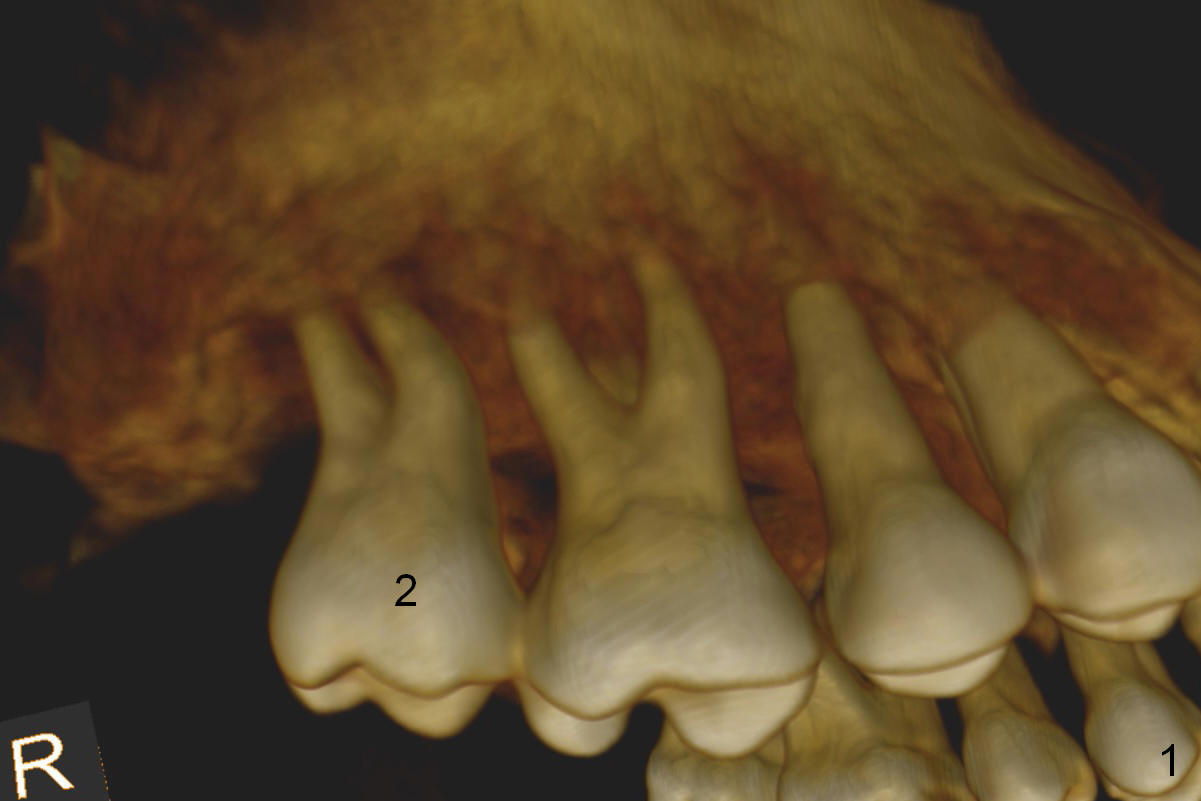
A 46-year-old lady is a typical dental phobic, but she is reasonable. Her chronic periodontitis is generalized and severe (Fig.1 3-D image, taken 1 year ago). An implant has been placed at #6 (healed site). It fails for the first time, probably due to bone loss after extraction. Soon after last periodontal maintenance, the tooth #2 develops pain and swelling. Immediate implant is a must.
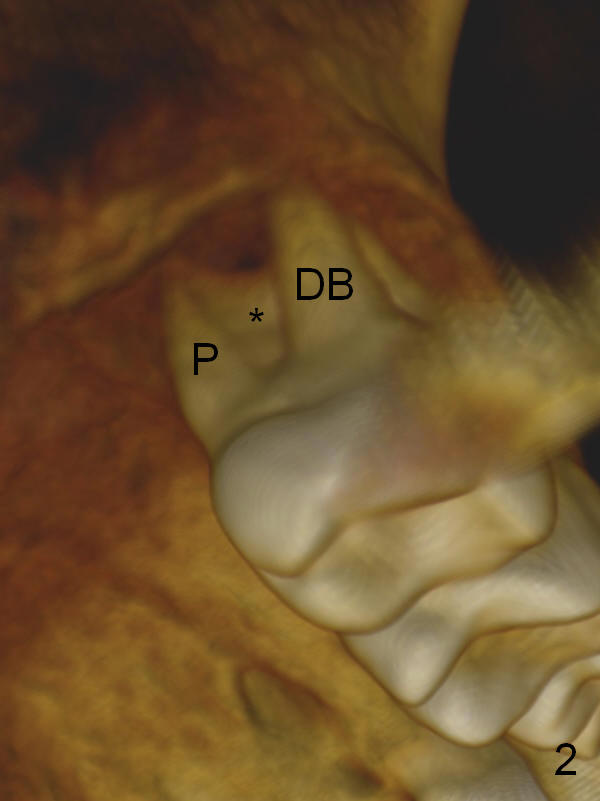
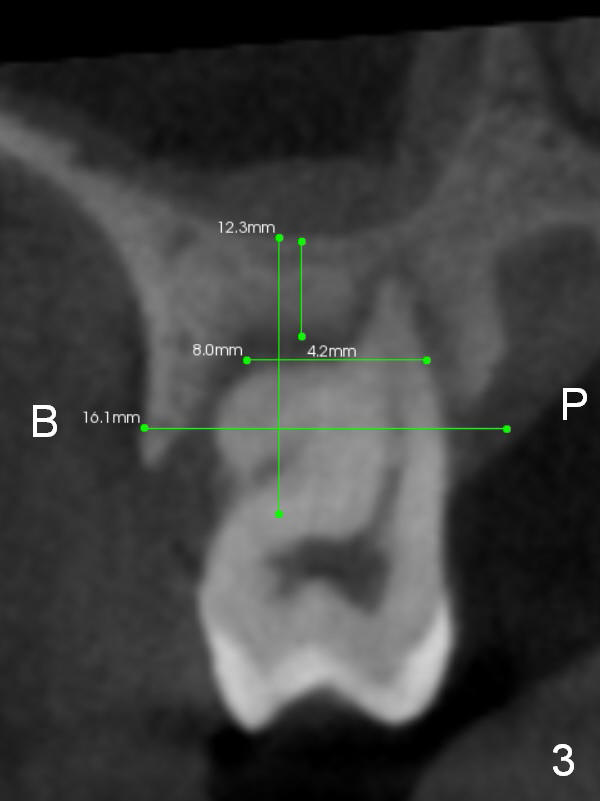
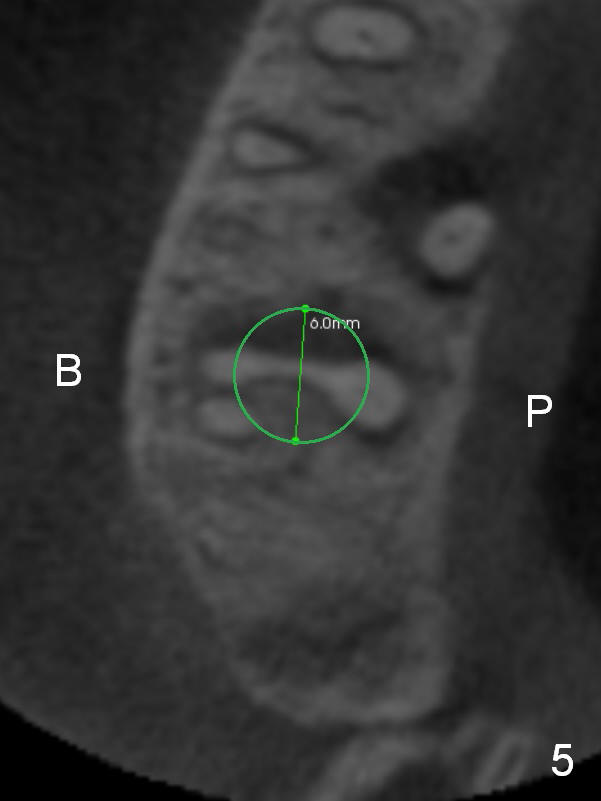
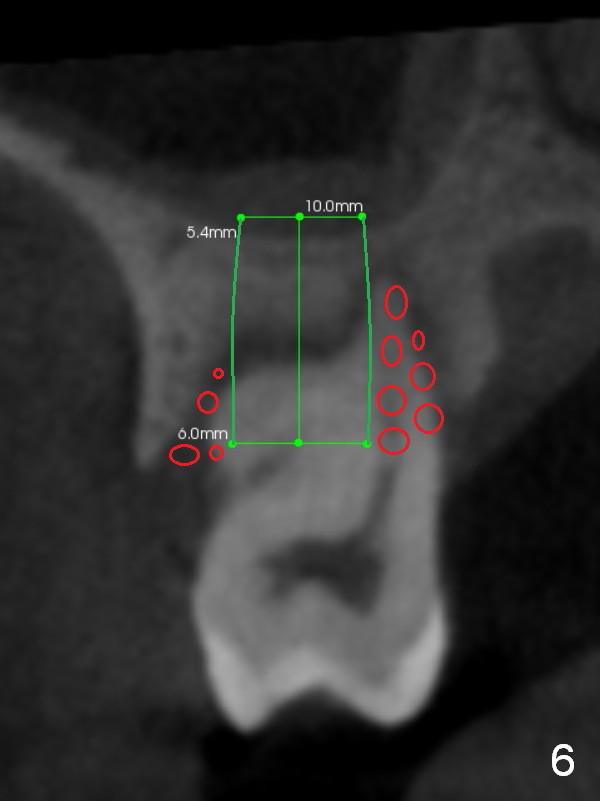
The socket is wider buccopalatally (Fig.2 (3-D disto-occlusal view),3 (coronal section)) than mesiodistally (Fig.1,4 (sagittal section),5 (axial section)). Unless more bone loss has occurred in the last year, a 6x10 mm UF implant is to be placed in the middle of the socket (Fig.6, (soaked with 2% Xylocaine/1:50,000 Epinephrine gauze)) with bone graft to be placed in the buccal and palatal gaps (red circles). Bone density in the middle of the socket is 550-700 Hounsfield units. Use RT2 or 2 mm pilot drill to start osteotomy ~ 3 mm. The largest osteotome is RT4, or largest reamer 4 mm, followed by 4.5x17 mm tap at 14 mm, until 6x17 mm one. Make sure that the sinus floor is penetrated.
Return to Upper Molar Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 12/09/2015, last revision 12/09/2015