

|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
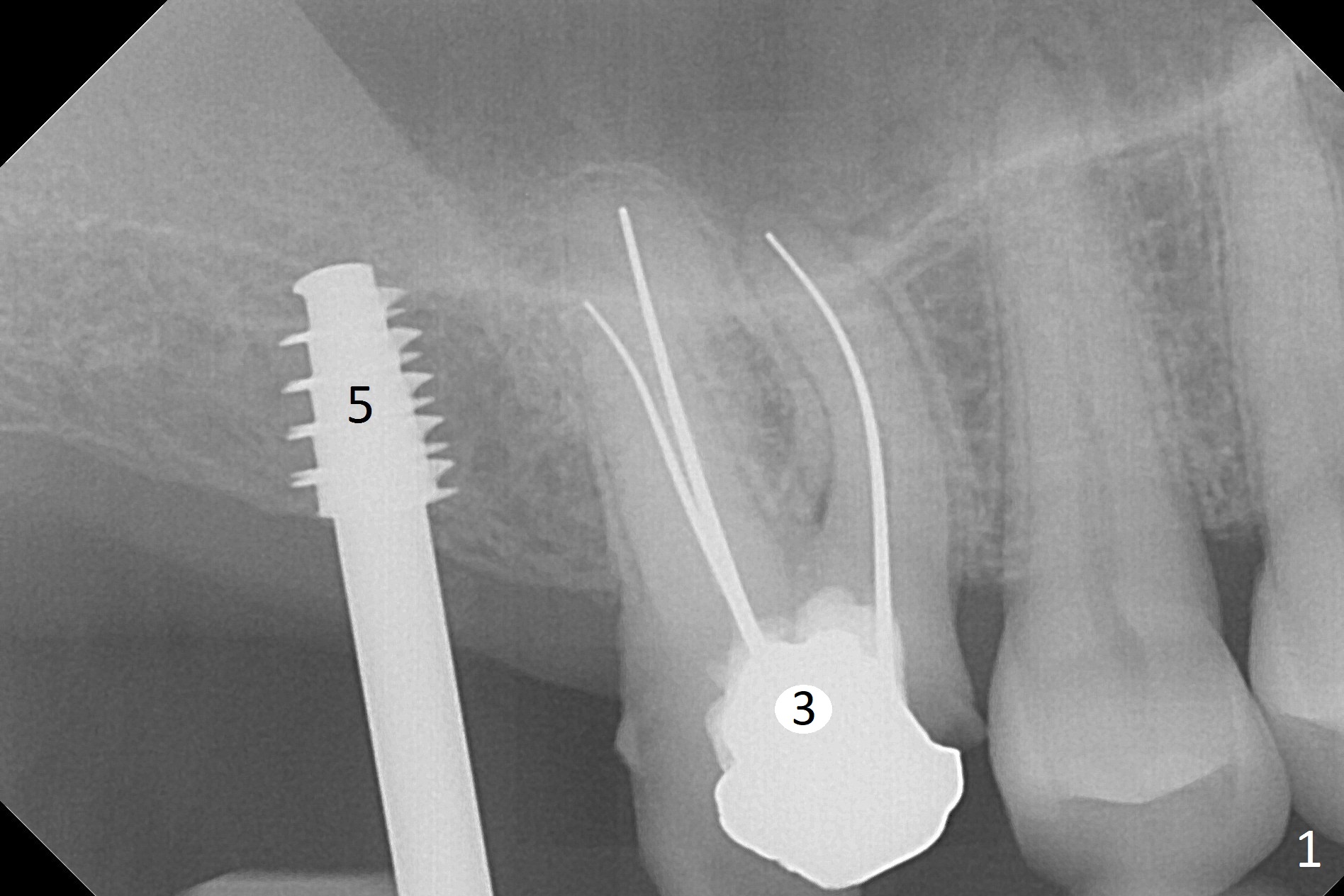
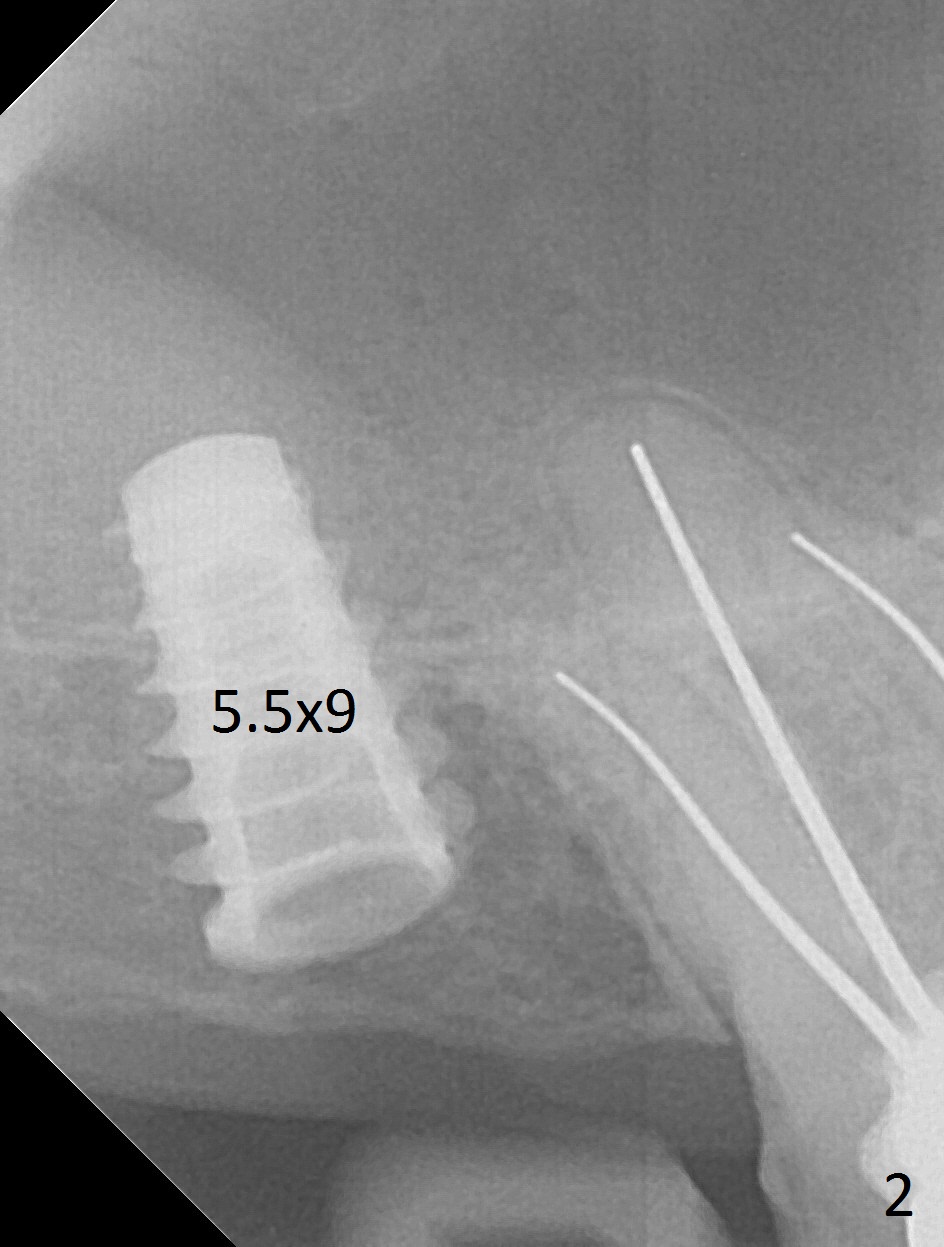
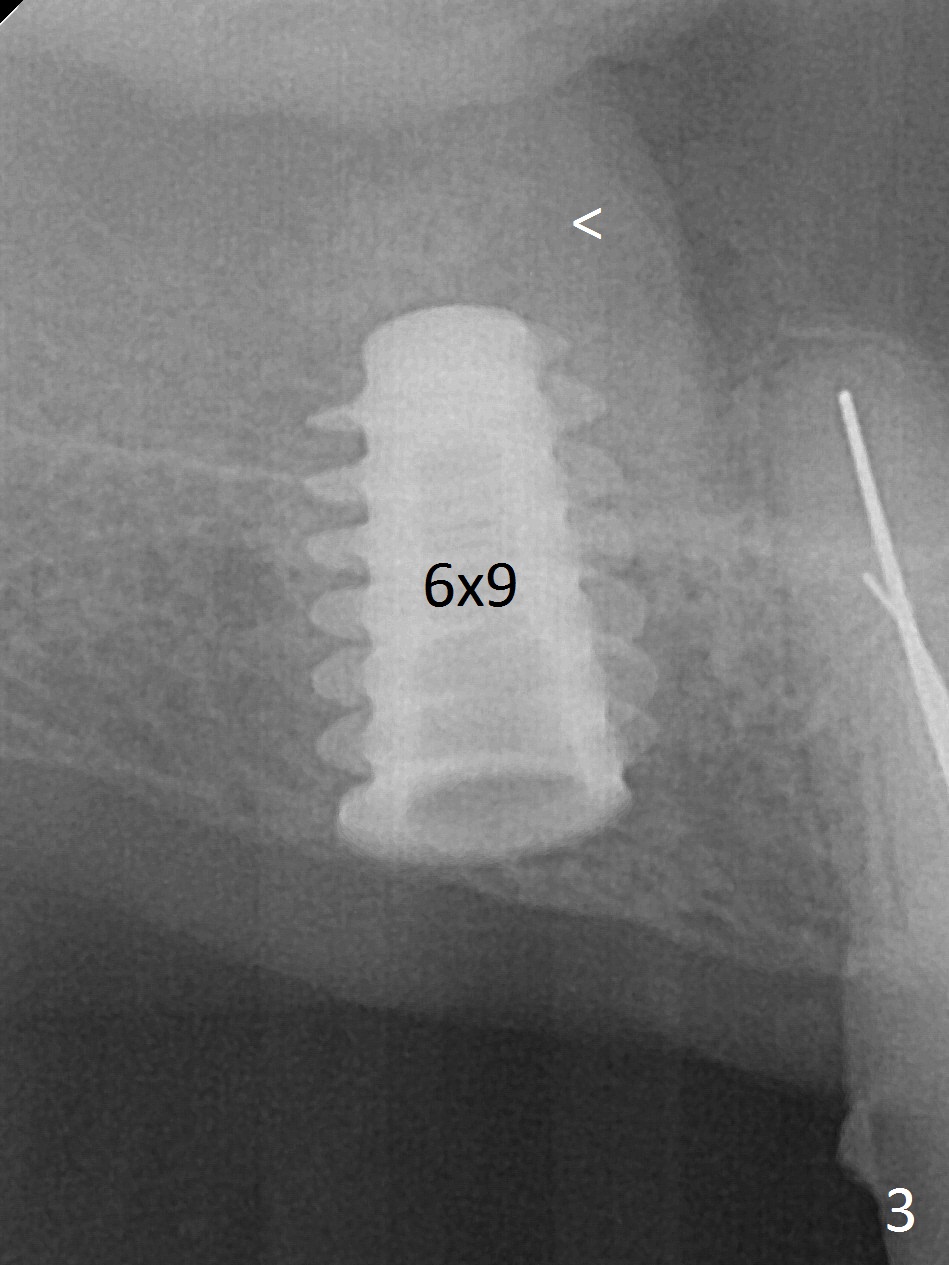
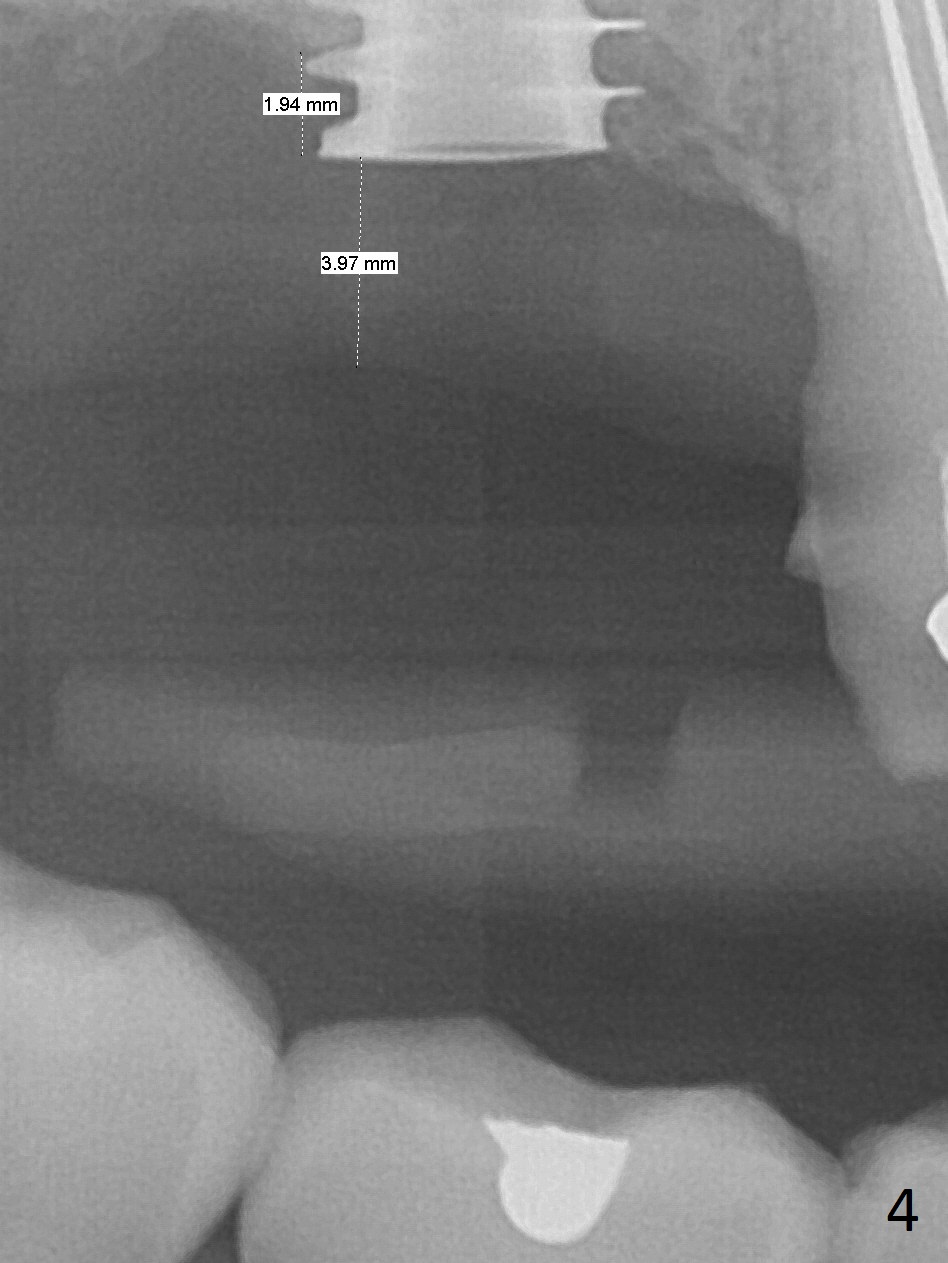
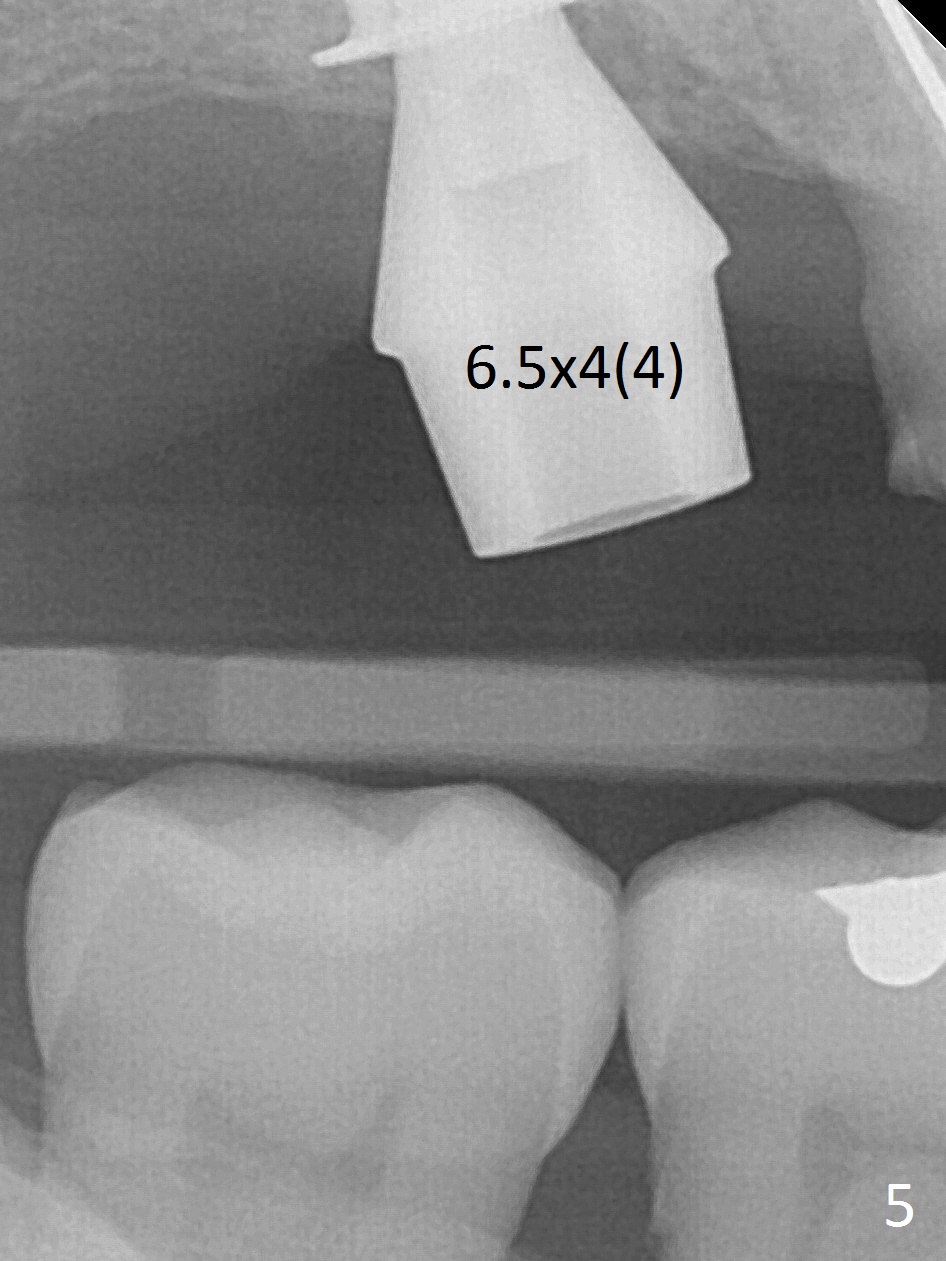
Extremely Wide Ridge
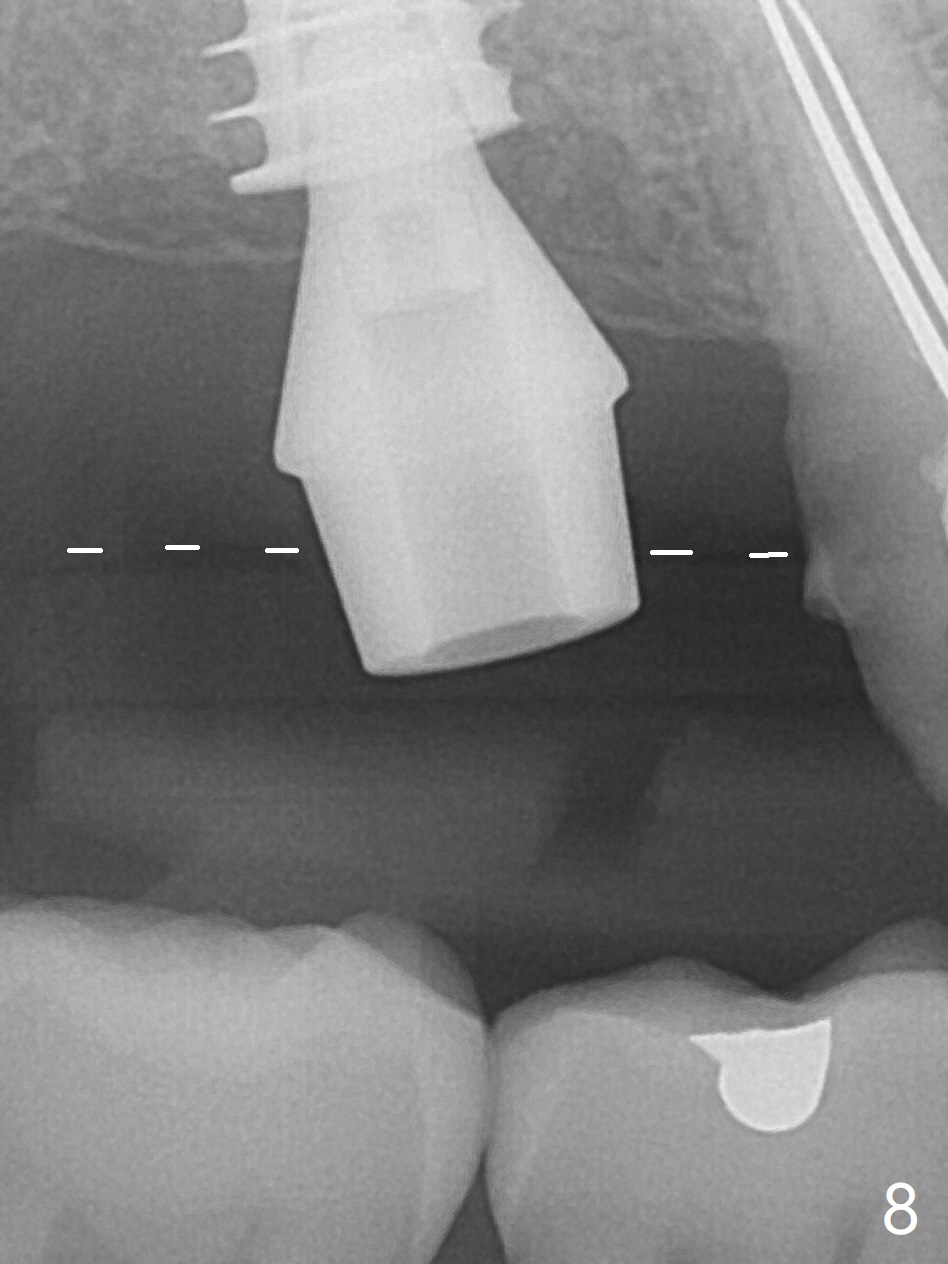
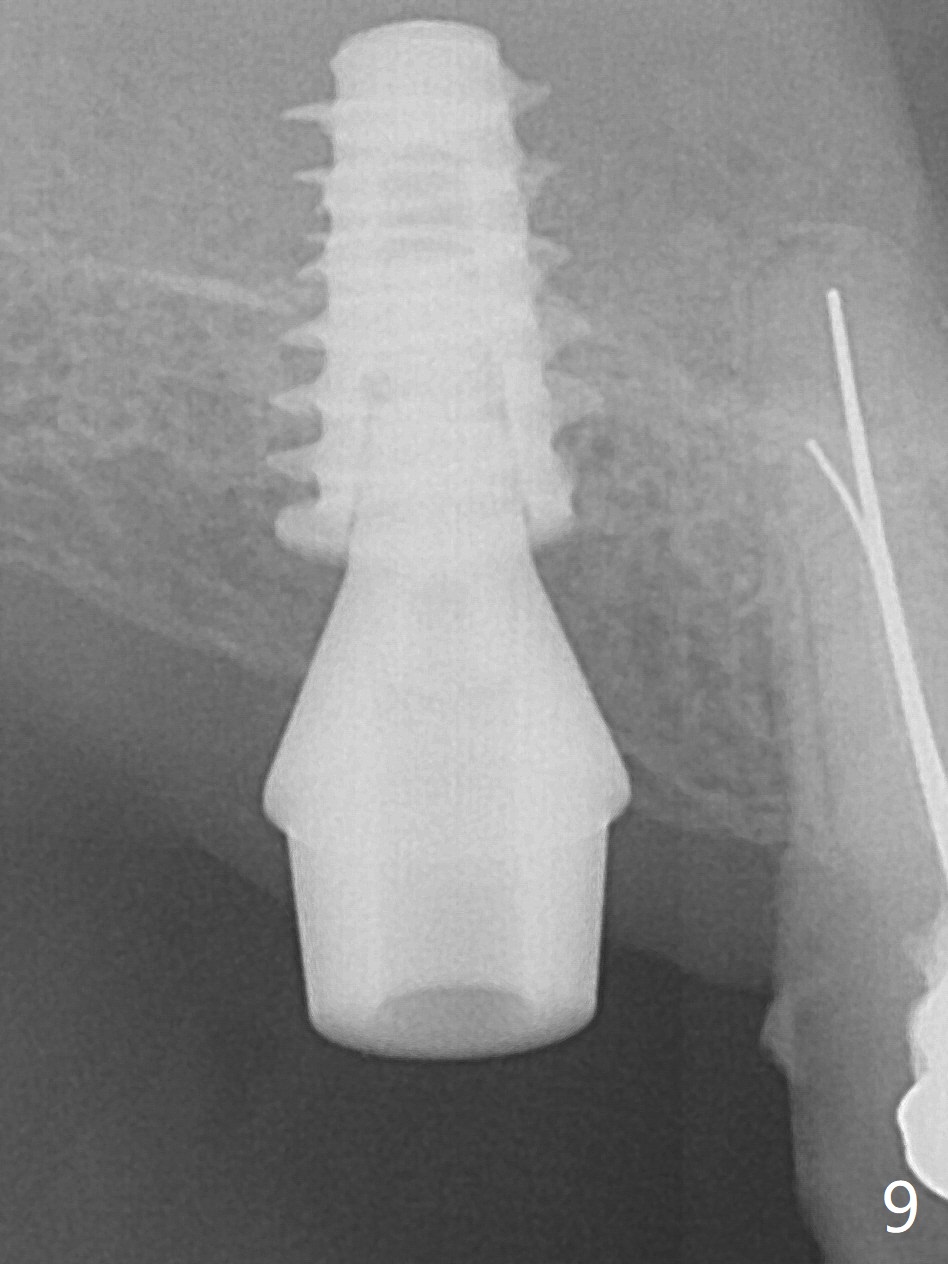
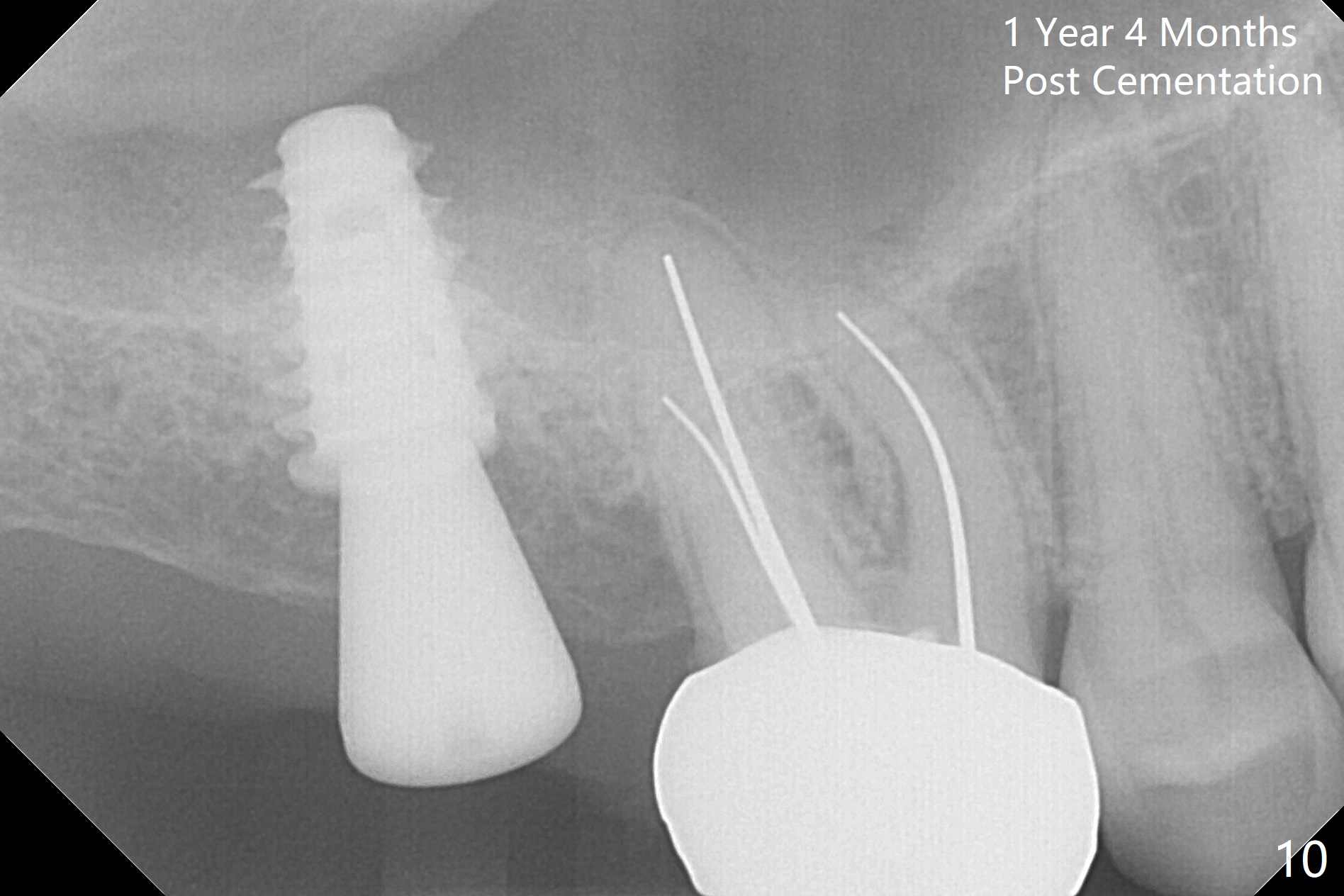
Since the ridge is wide at the site of #2, Magic Split is used for access (flapless) and bone expansion. The bone is so soft that there is no resistance until 4.3 mm Magic Expander is used for 9 mm (Fig.6). A 5 mm tap drill is stable (Fig.1), so are a 5.5x9 mm dummy implant (Fig.2) and a 6x9 mm IBS implant (Fig.3 (<: sinus lift)). In fact the distal thread is still supracrestal (Fig.4 (BW)). After additional 2 mm placement, the distal thread is subcrestal (Fig.5); the mesial margin of a 6.5x4(4) mm abutment is subgingival. A longer cuff (5 mm instead of 4 mm) is more favorable for future restoration. At present the abutment (Fig.7) as well as the tooth #3 with rugged surfaces is used to hold periodontal dressing in place. The abutment margin is completely subgingival 3 months postop (Fig.8 (white dashed line: gingival margin)). It appears that the implant is placed ~ 1 mm deeper than ideal (Fig.9). Diode laser is used for gingivectomy prior to impression. The abutment screw becomes loose 2 months post cementation. After retightening, occlusal equilibrium is conducted with 3 layers of articulating paper. Night guard is provided. The crown/abutment dislodges 1 year 2 months later. Since the gingiva is erythematous, a 6x7 mm healing abutment is placed (Fig.10). The implant seems to have been placed too deep and palatal. It appears that an abutment driver should be buried to prevent the screw re-loosening. Guided surgery should have been done.
Return to
Upper
Molar Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 06/16/2017, last revision 02/16/2019