








|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Small Immediate Implant Placed in the Septum with Large Healing Abutment
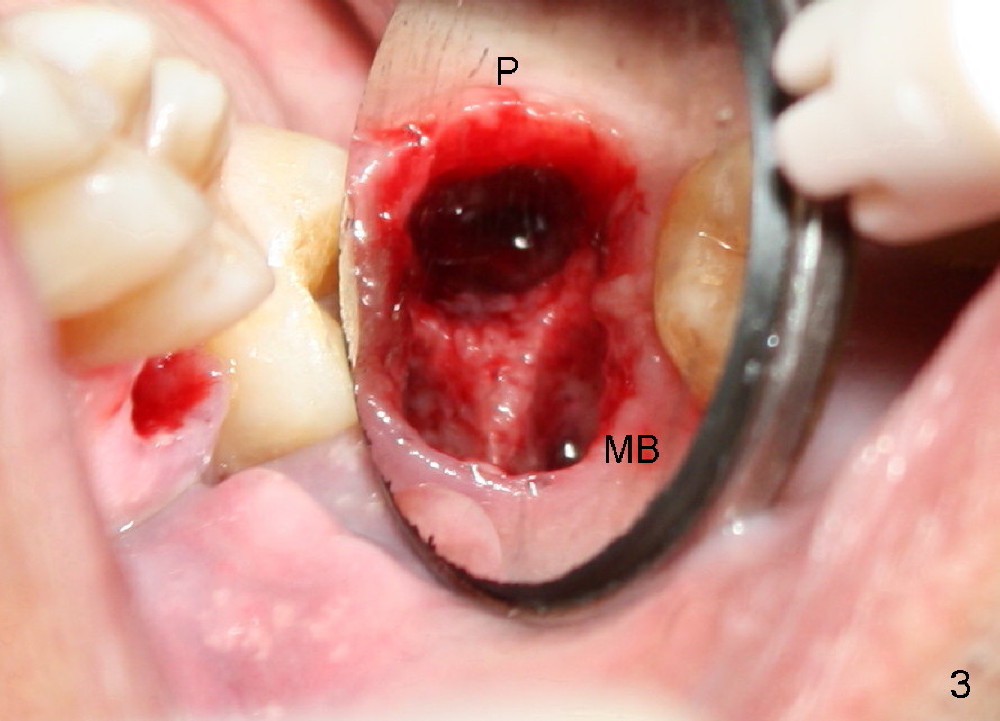
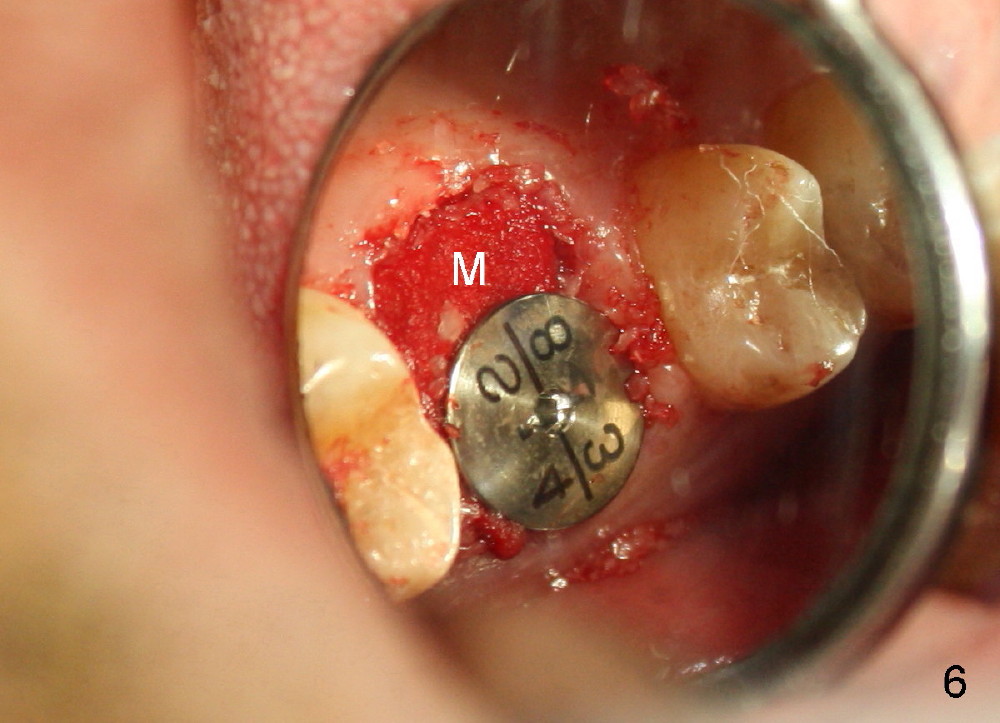
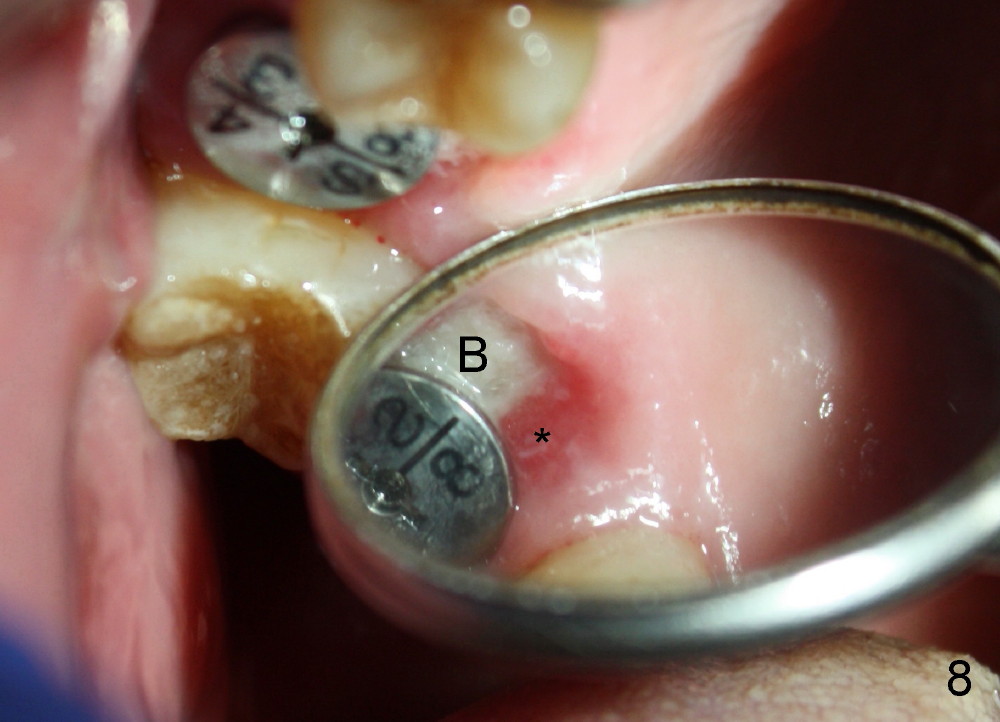
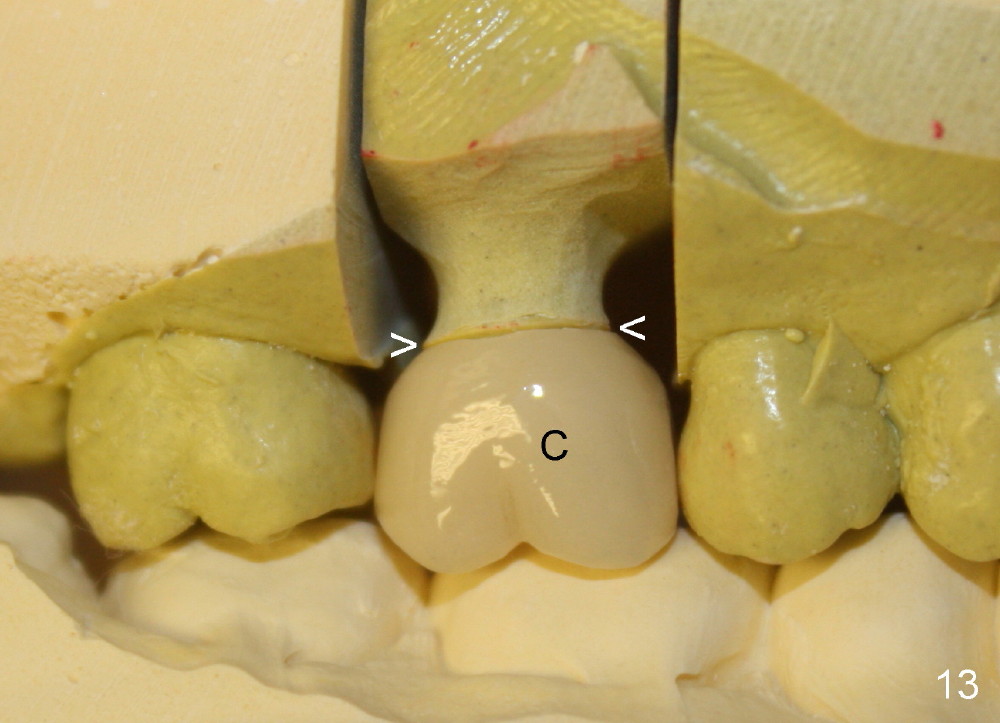
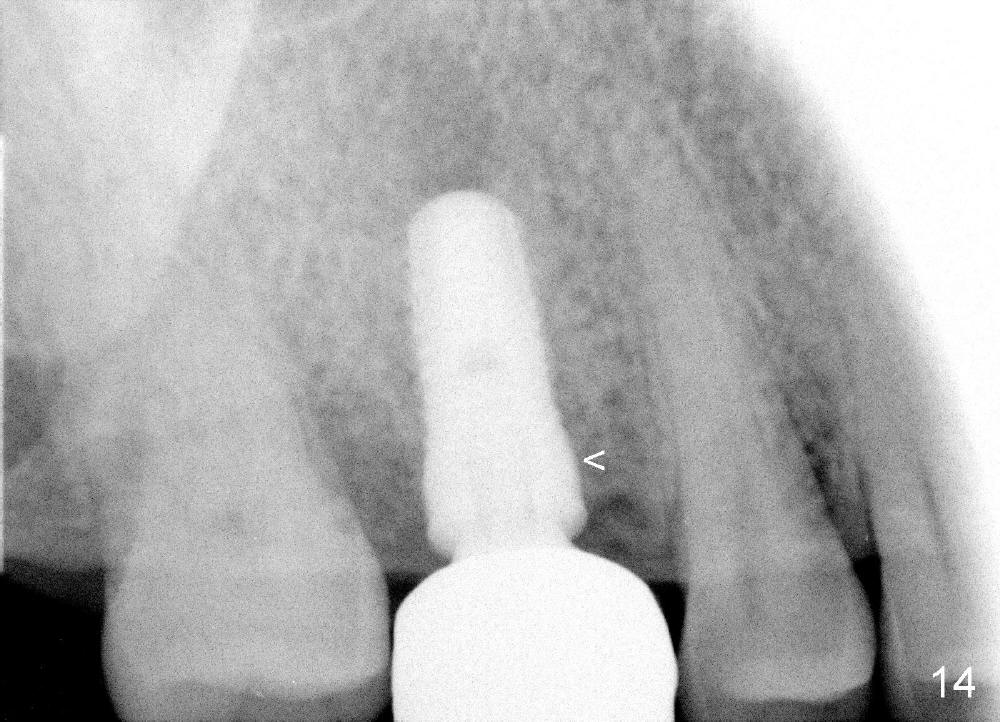
The tooth #3 has a crack line (Fig.1 ^). The septum (Fig.2 S) looks like an inverted pyramid (Fig.3), coronal part being pointed, whereas the apical broad. The shape of the septum is not so favorable to placement of tapered implant. Osteotomy starts with 1.5 mm pilot drill in the middle of the septum, followed by round tapered osteotomes 2 and 3 mm. The osteotomy begins to deviate into the mesiobuccal socket. The same osteotomes are used to re-direct the osteotomy palatally, followed by tapered drills, trying to move osteotomy palatally. A 4.5x17 mm tap is inserted with stability (Fig.4). Following using 5x17 mm tap at the depth of 12 mm, a 5.3x12 mm bone-level implant is placed ~ 1.5 mm below the crest, 1.5 mm above the septum (Fig.5). Demineralized cortical human allograft is placed in the remaining sockets and around the most coronal aspect of the implant (with a small piece of gauze placed in the implant well). After removal of the gauze, a piece of collagen membrane is pierced and carried by a 8.2x4/3 mm healing abutment and fixed in place (Fig.6 M). The periphery of the membrane is tucked underneath the gingiva. The wound is covered by perio dressing. The patient returns to clinic for follow up 8 days postop. There is no discomfort. In order to protect the collagen membrane (Fig.6), the perio dressing is intentionally not removed (Fig.7). Two weeks postop, the patient remains asymptomatic. After perio dressing removal, the membrane appears to have been resorbed (Fig.8 as compared to Fig.6). The bone graft (B), although exposed, remains in place and condensed, surrounded by healing healthy gingiva (*). The patient returns 2.5 months postop. The implant appears to osteointegrate (Fig.9, as compared to Fig.5). The buccal (Fig.10) and palatal (Fig.11) gingiva adapts to the healing abutment. When the healing abutment is removed for restoration 3 months postop, the gingiva looks healthy (Fig.12). A cemented abutment (5.8x4(2) mm) is placed; a crown is fabricated (Fig.13). The patient returns for recall 5 months post cementation. He reports food impaction distal to the crown. The gap mesial to the implant has closed (Fig.14).
Placement of a relatively small implant (~5 mm) may not damage the coronal aspect of the septum as much as a large one (6-8 mm). The socket can be closed for the most part by using a large healing abutment (8, 9 mm). Since the socket is oval in shape (Fig.3), collagen membrane (Fig.6 M) or released flap is supplemented to close the socket completely. A potentially more secure method to close the socket opening is to place a wide temporary abutment (ø 5.8 mm) and fabricate an immediate provisional, which is infraocclusal.
It appears a little harder to place an immediate implant in a lower molar septum, since the latter is relatively smaller.
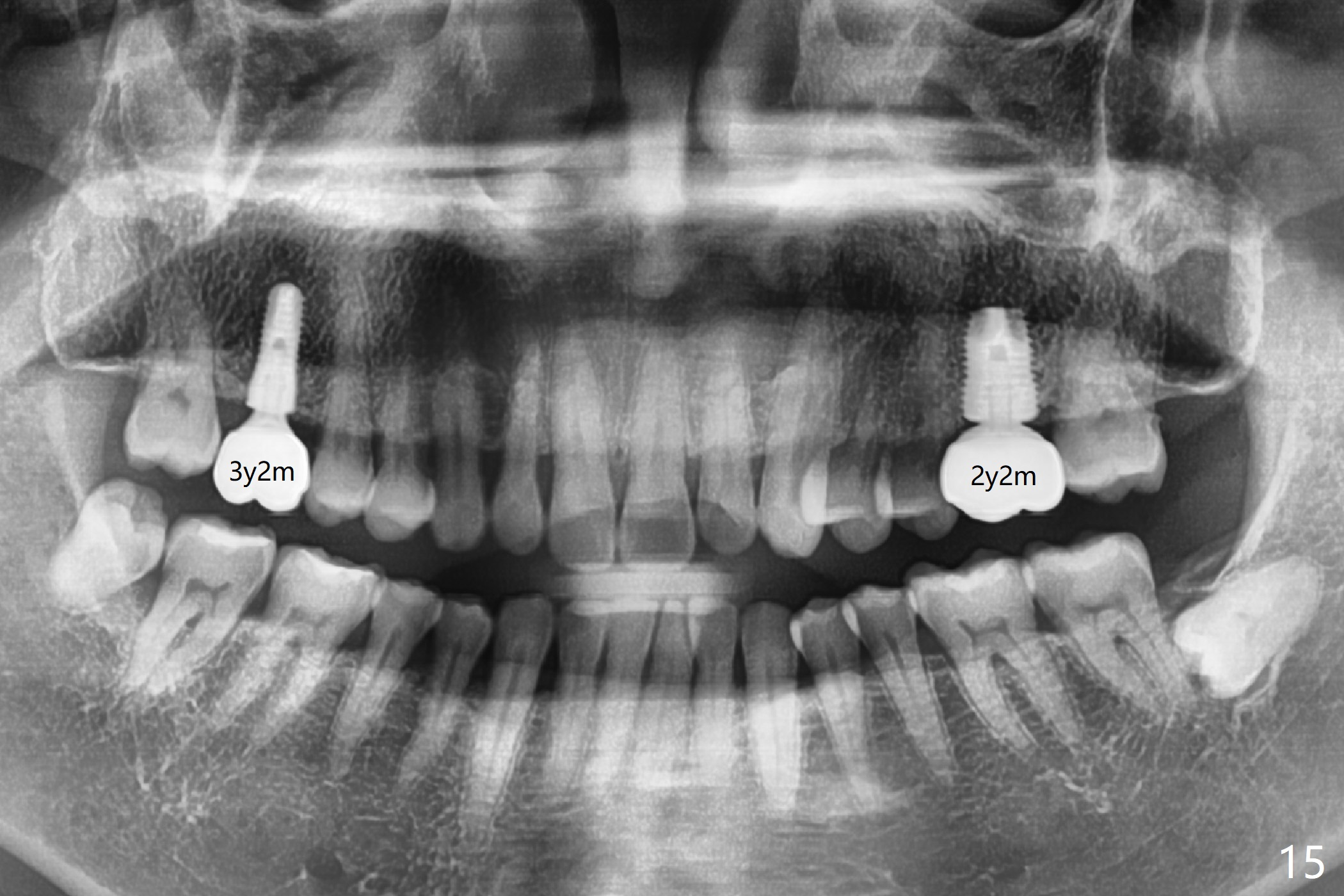
The crowns at #3 and 14 have been cemented for 3 years 2 months and 2 years 2 months, respectively (Fig.15).
Upper Molar Immediate Implant,
Professionals
Xin Wei, DDS, PhD, MS 1st edition 01/22/2014, last revision 07/14/2018