
,%20pp.jpg)
.jpg)
,%206.5x4(2),%20trimmed%20distolingual.jpg)




|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Change Trajectory Early
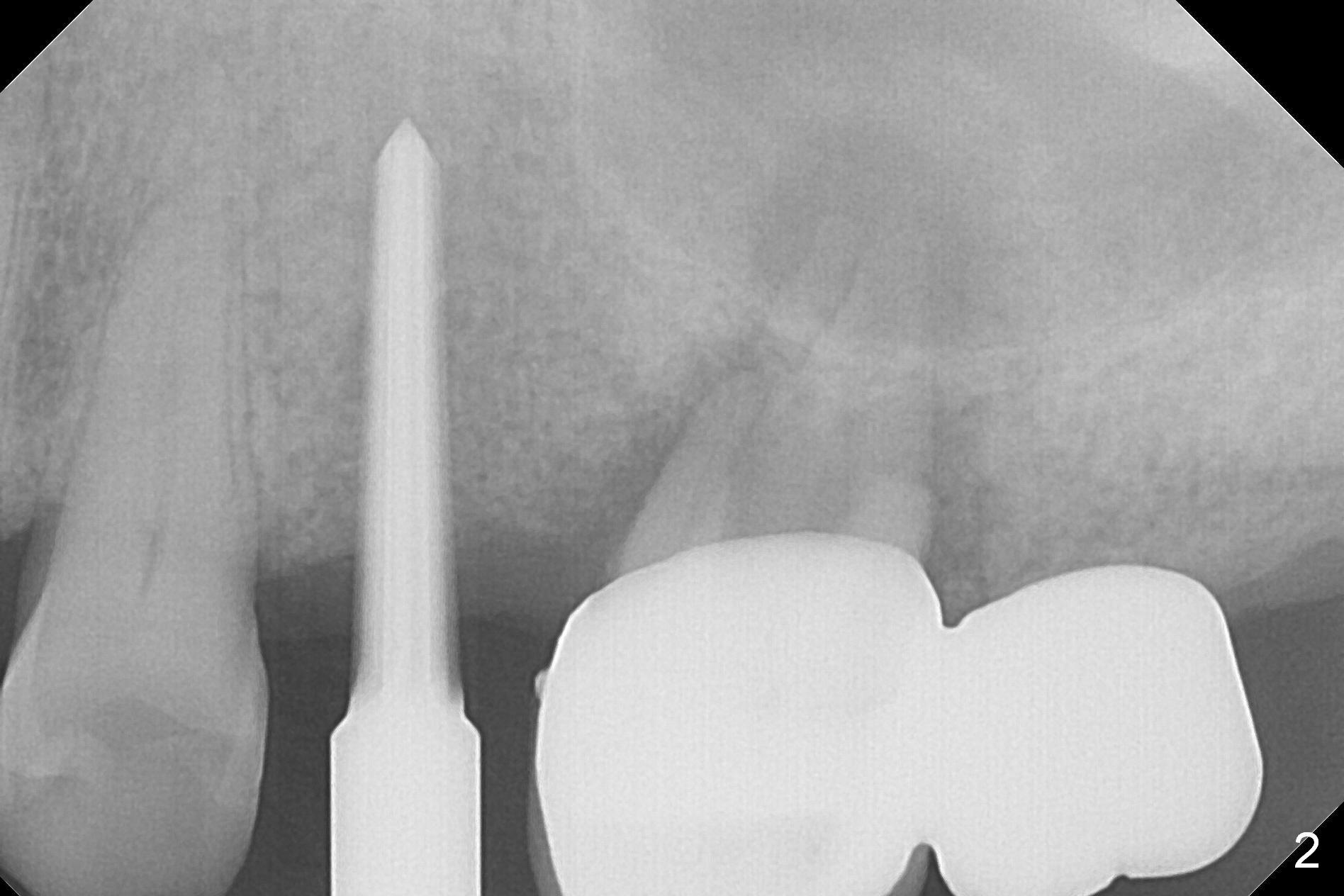
Osteotomy is initiated with Magic Split and a 1.6 mm drill at #13 before #14/15 cantilever bridge is removed (Fig.1). The trajectory is to be corrected (black line) in case an implant is placed at #14. After using Lindamann bur and reusing the 1.6 mm drill, a 3 mm Magic Expander is tapped in for 15 mm with ideal trajectory (Fig.2).
Following placement of a 4.5x13 mm IBS implant (>50 Ncm) and 5x4(3) mm pair abutment, the cantilever bridge is removed. Bone loss at #14 is so severe that an immediate implant seems to be inappropriate. Finance is another factor. Osteotomy is initiated at #15, followed by insertion of a parallel pin (Fig.3).
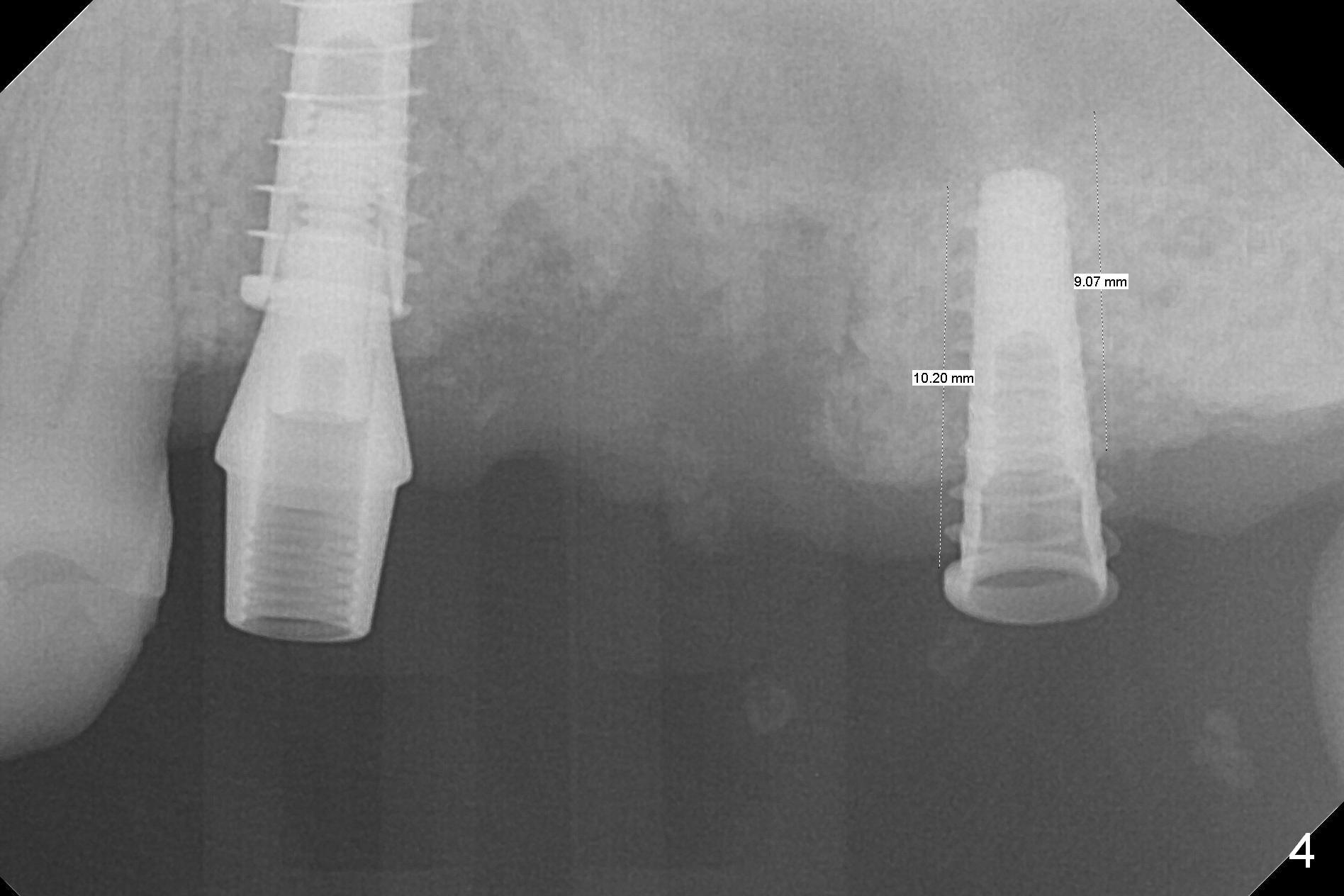
Then 4.3 mm Magic Drill is used at #15. When a 5x9 mm dummy implant is placed mesial to the osteotomy, it slides partially into the palatal socket of #14 (data not shown). When a smaller dummy implant (4.5x11 mm) finds the original osteotomy, the trajectory is acceptable (Fig.4).
To prevent sinus membrane perforation, a piece of PRF membrane is inserted into the osteotomy, followed by mixture of autogenous bone, allograft (.5-1.5 mm) and Osteogen for sinus lift. A 5x9 mm implant is placed with 50 Ncm as well as 6.5x4(3) mm abutment (Fig.5).
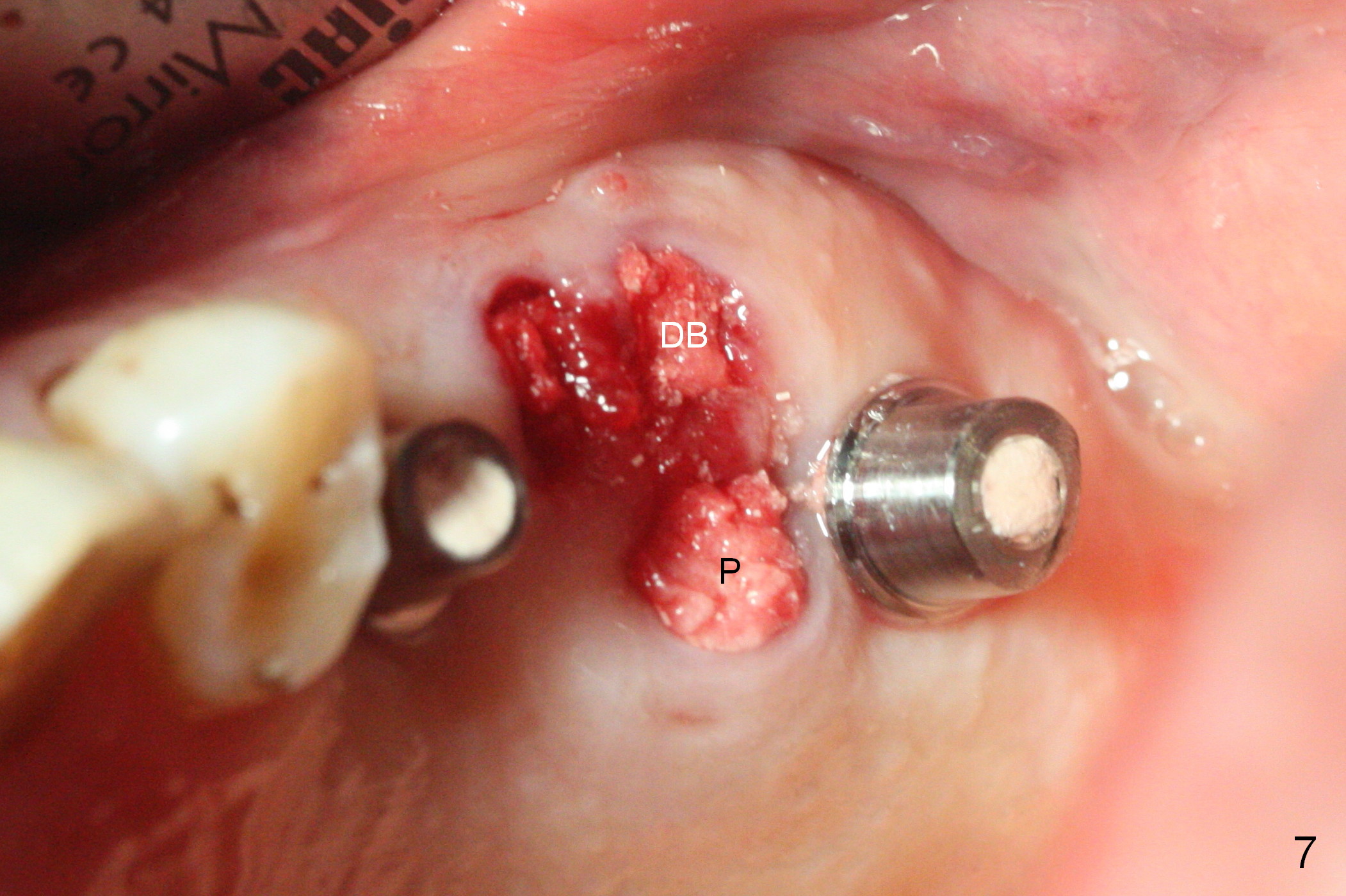
After placement of the remaining graft into the palatal (Fig.6,7 P) and distobuccal (DB) sockets of #14 and collagen plug into the 3 sockets of #14, abutments change to those with cuffs 1 mm shorter. The abutments are used to hold an immediate provisional bridge in place. The latter keeps the collagen plug and graft in place.
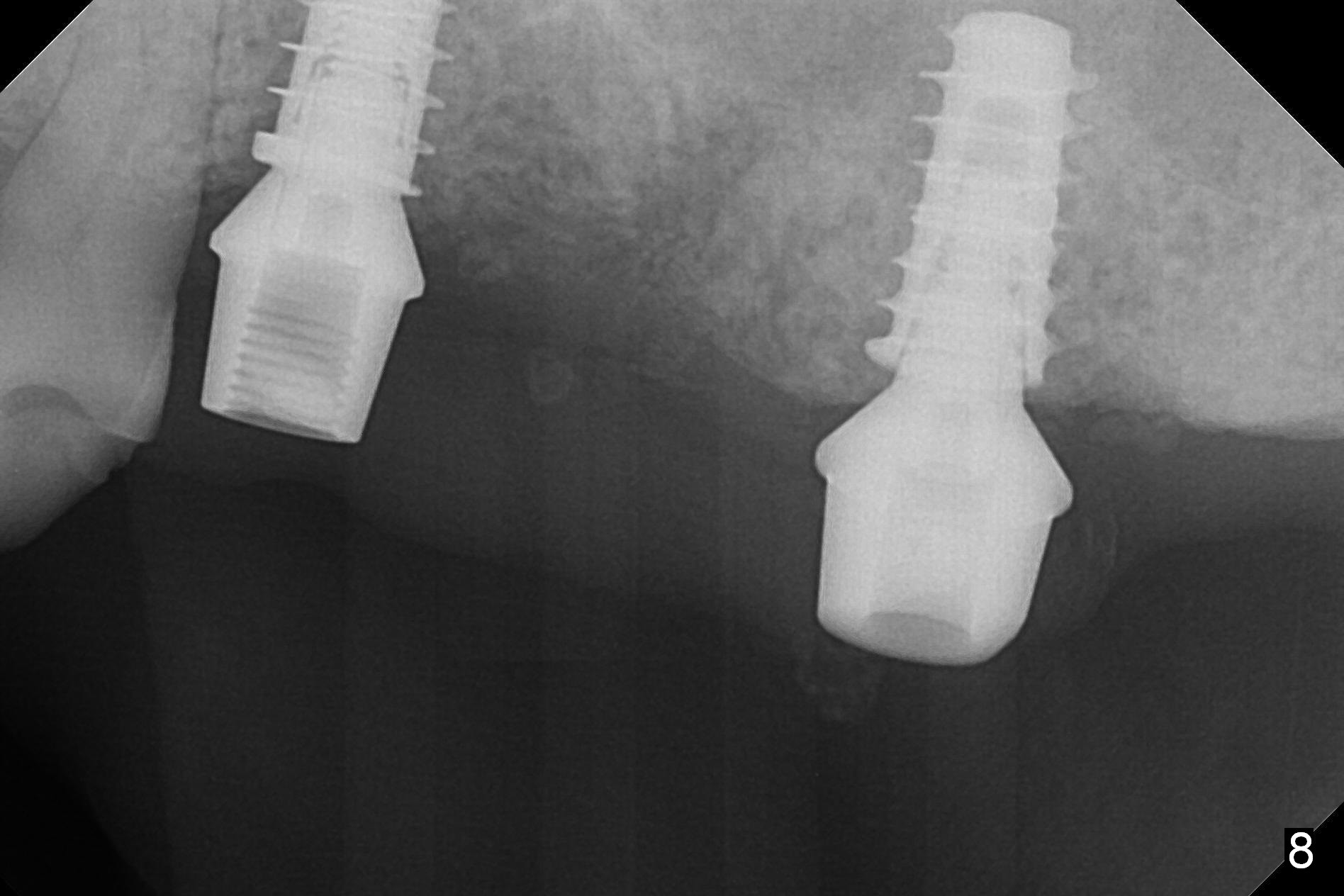
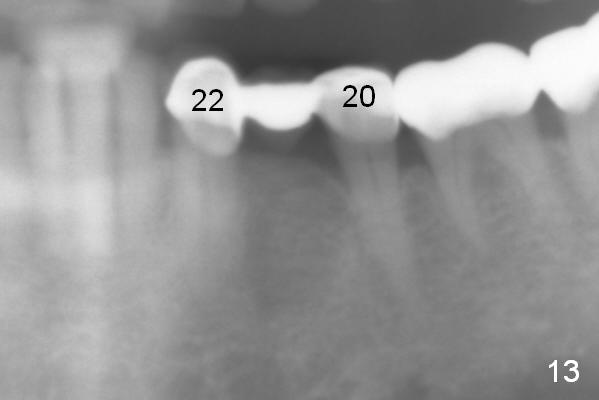
The fistula buccal to #14 remains 1 week postop (Fig.7) and disappears 1 months postop. The fistula does not re-appears 3 months postop with the implants at #13,15 apparently osteointegrated (Fig.8). With relining #13-15 provisional with increased vertical height (Fig.11), the patient has bilateral posterior contact (Fig.9), while the lower incisors do not contact the cinguli of the upper incisors (Fig.10 *). The space between the tooth #12 and the pontic #21 is unfavorable for posterior occlusal stability (Fig.11 *). Porcelain is chipped off the buccal surface of the pontic (Fig.12 *). If the patient does not afford an implant at #21 with redo crowns at #20 and 22 (Fig.13), what else could be done? He will return for #15 implant placement 4 months post socket preservation.
Return to
Upper Molar,
Premolar Immediate Implant,
#2,4,
#28,
Redo
Xin Wei, DDS, PhD, MS 1st edition 12/20/2016, last revision 01/19/2018