
.jpg)
.jpg)
.jpg)
,%203x16(4)%20trimmed%20off%203%20mm.jpg)

,%20trimmed%20top.jpg)






,%203.8x10,%204.5x5(2).jpg)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
How to Prevent Perforation in Lower Anterior Region
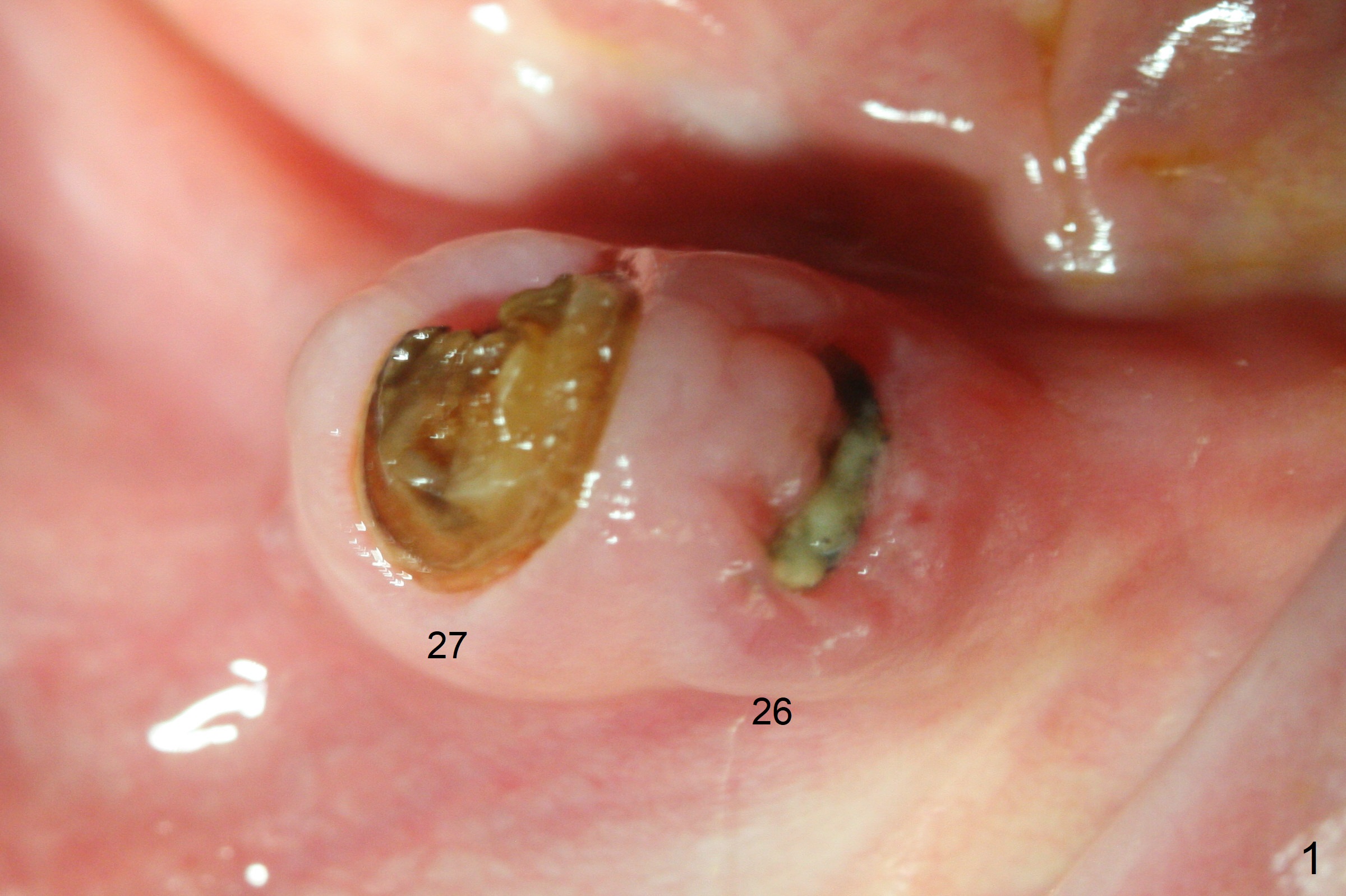
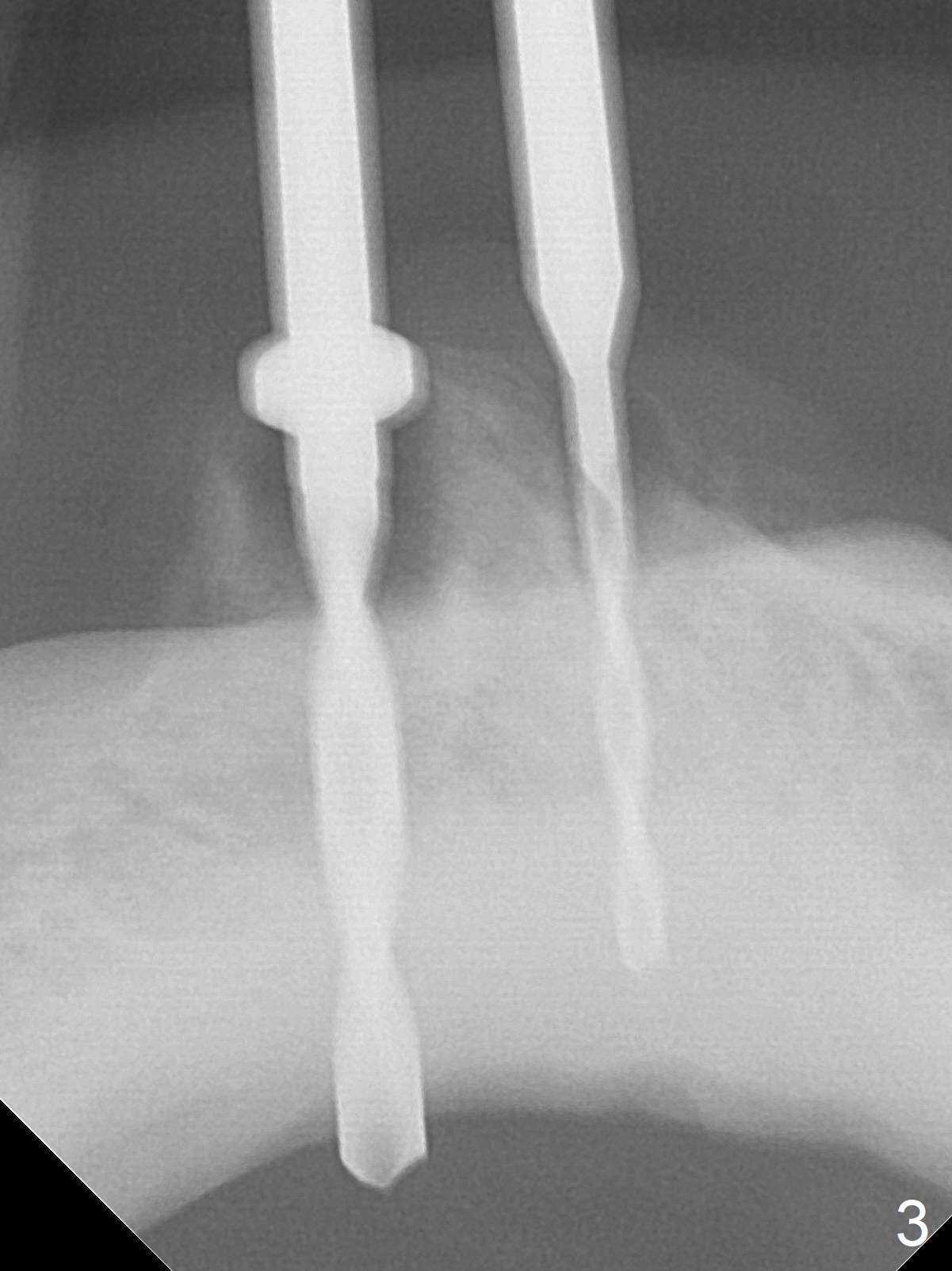
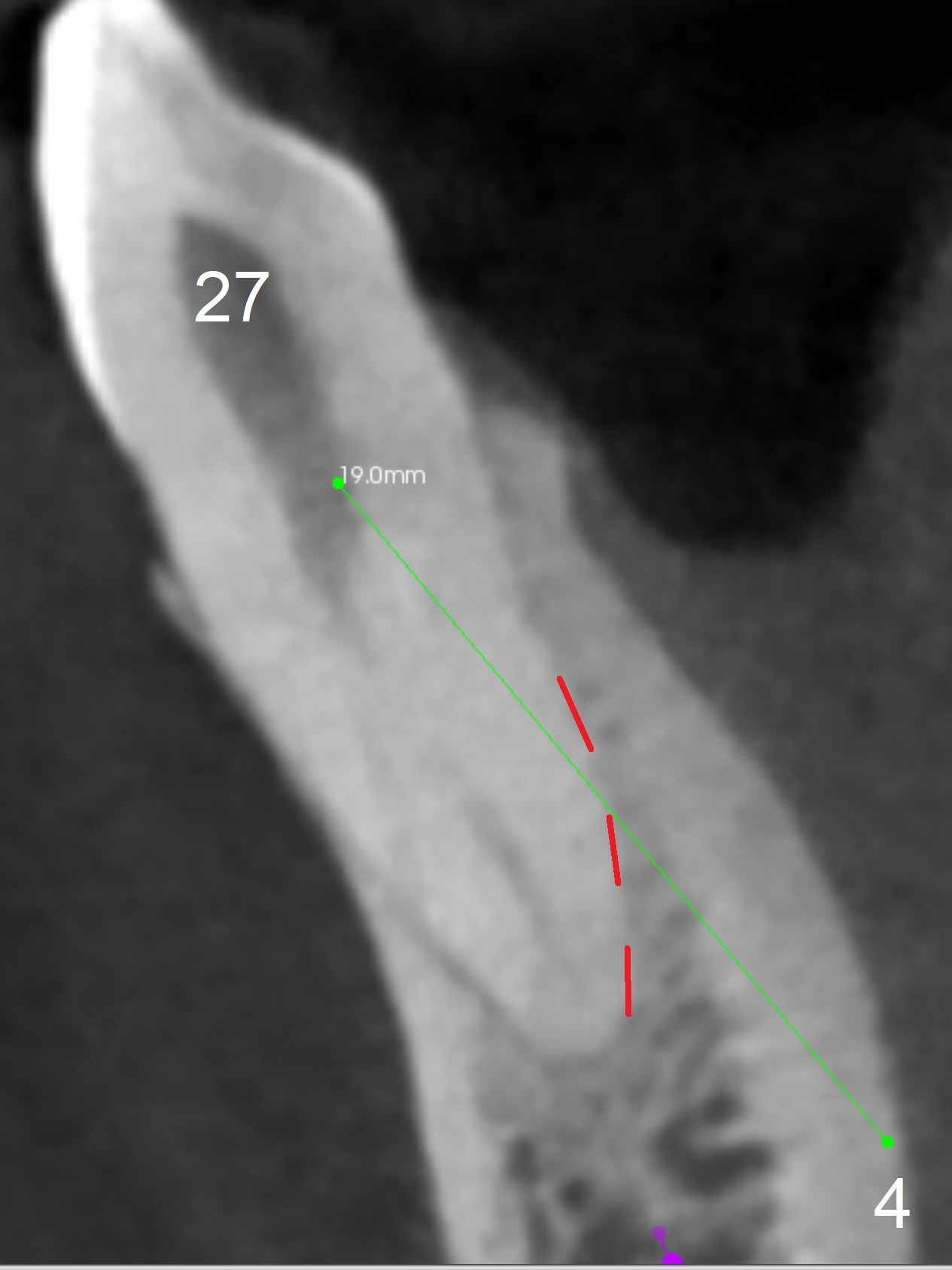
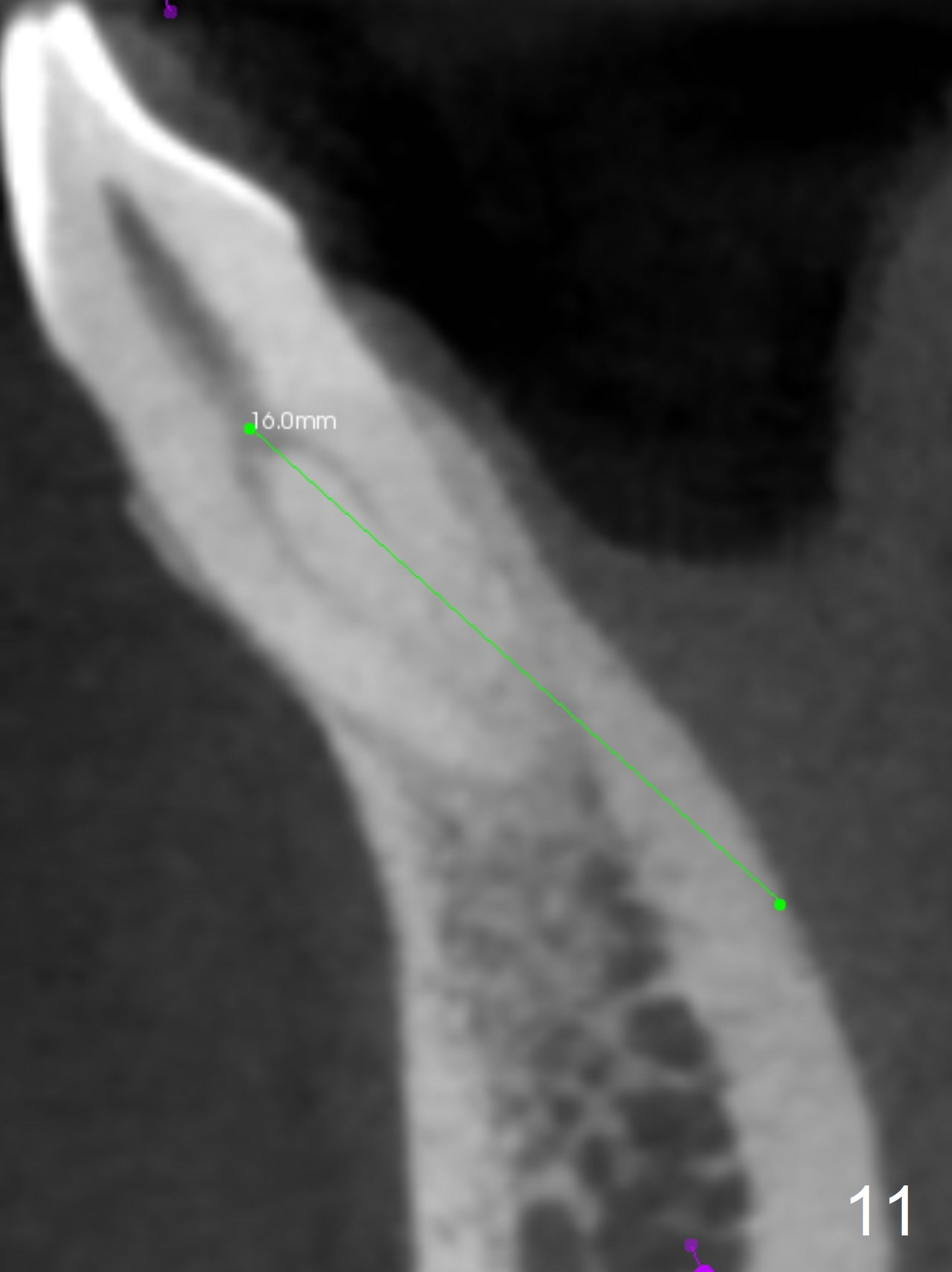
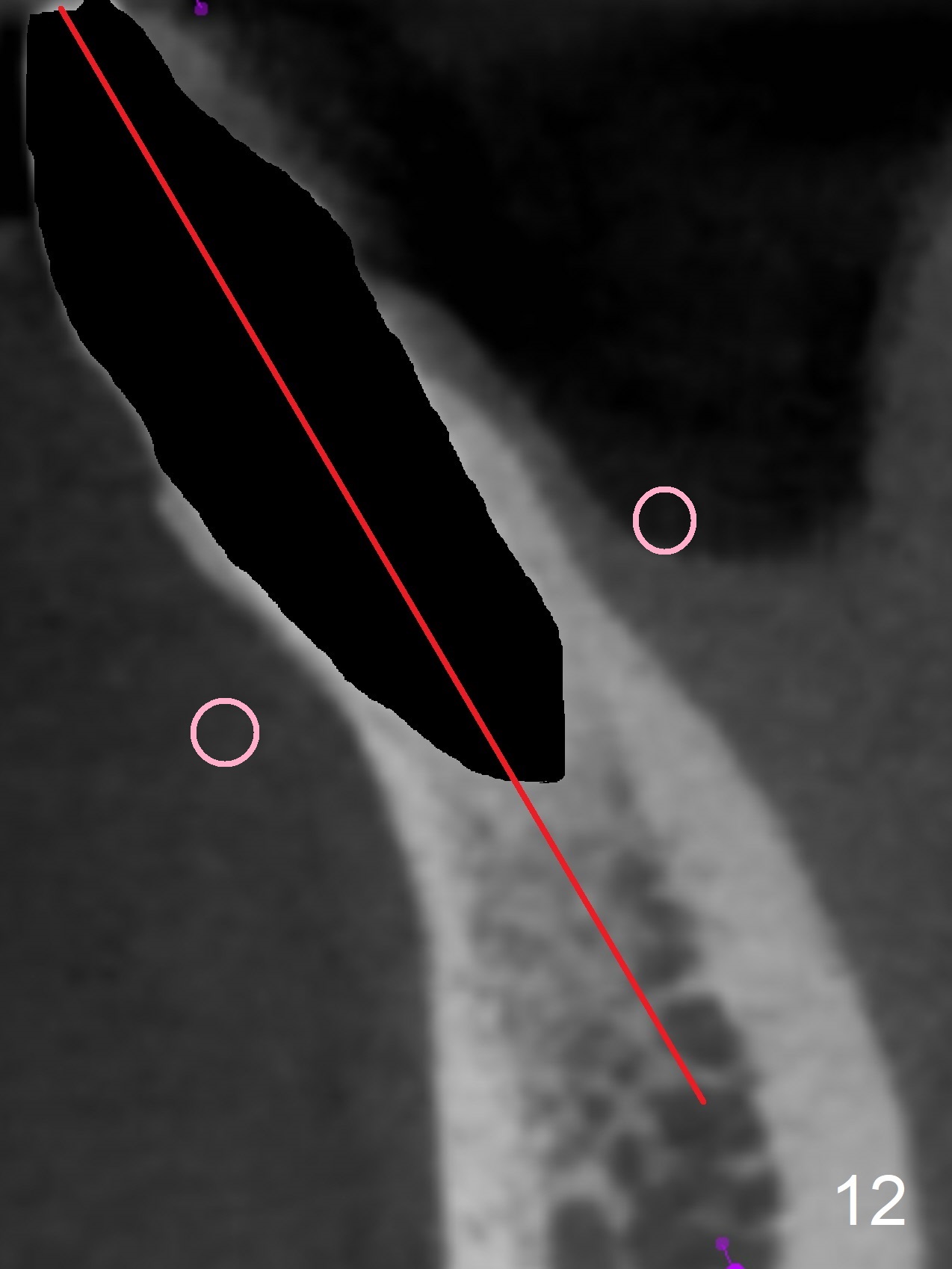
When the patient returns for #26 extraction and immediate implant and #27 RCT, it appears that the tooth #27 with subgingival margin distolingually is non-salvageable (Fig.1). She has dry mouth. Osteotomy is initiated in the lingual slope (Fig.4 red dashed line) of each socket with 1.2 and 2 mm drills for 16 and 19 mm at #26 and 27, respectively (Fig.2,3). The depth at #27 is subsequently reduced, while a 3x14(2) mm dummy implant is placed at #26 (Fig.5,6). A 3.8x13 mm implant is placed at #27 smoothly, while insertion of a 3x16(4) mm definitive implant (by mistake) has resistance (Fig.7). When the depth at #26 increases, there is feeling of perforation. The apex of the implant is truncated prior to reinsertion (Fig.8 >).
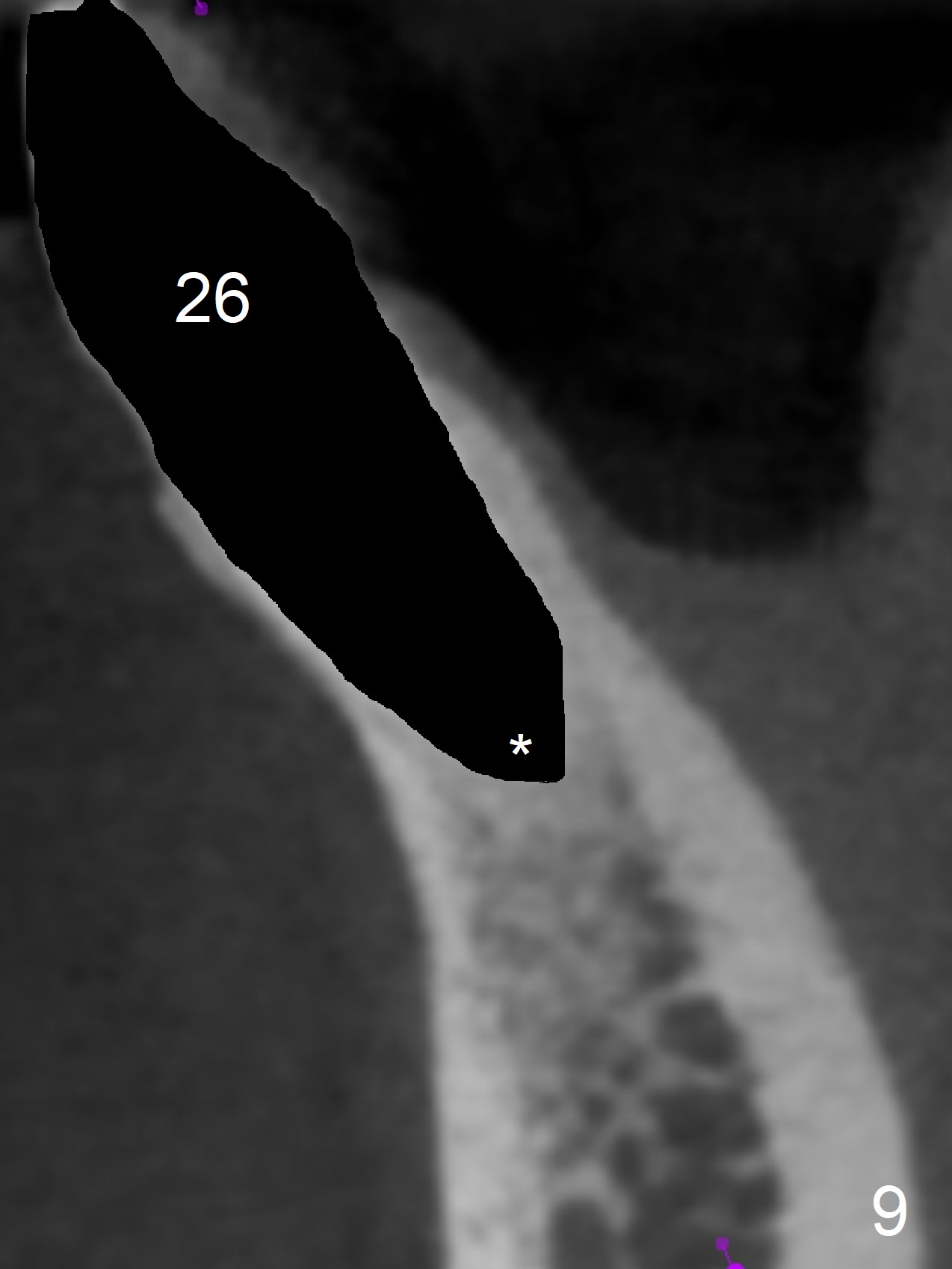
In fact the apex of the lateral incisor is also in the center of the alveolus (Fig.9 *). Osteotomy established in the lingual slope for a long distance (Fig.10,11) will perforate the lingual plate. The correct method of osteotomy is to set up in the middle of the socket and along the long axis of the alveolus with 2 fingers holding the alveolus (Fig.12 (2 circles)). The problem for this case is to use the lower RPD as a guide. With the RPD in place, the tactile sensation is lost.
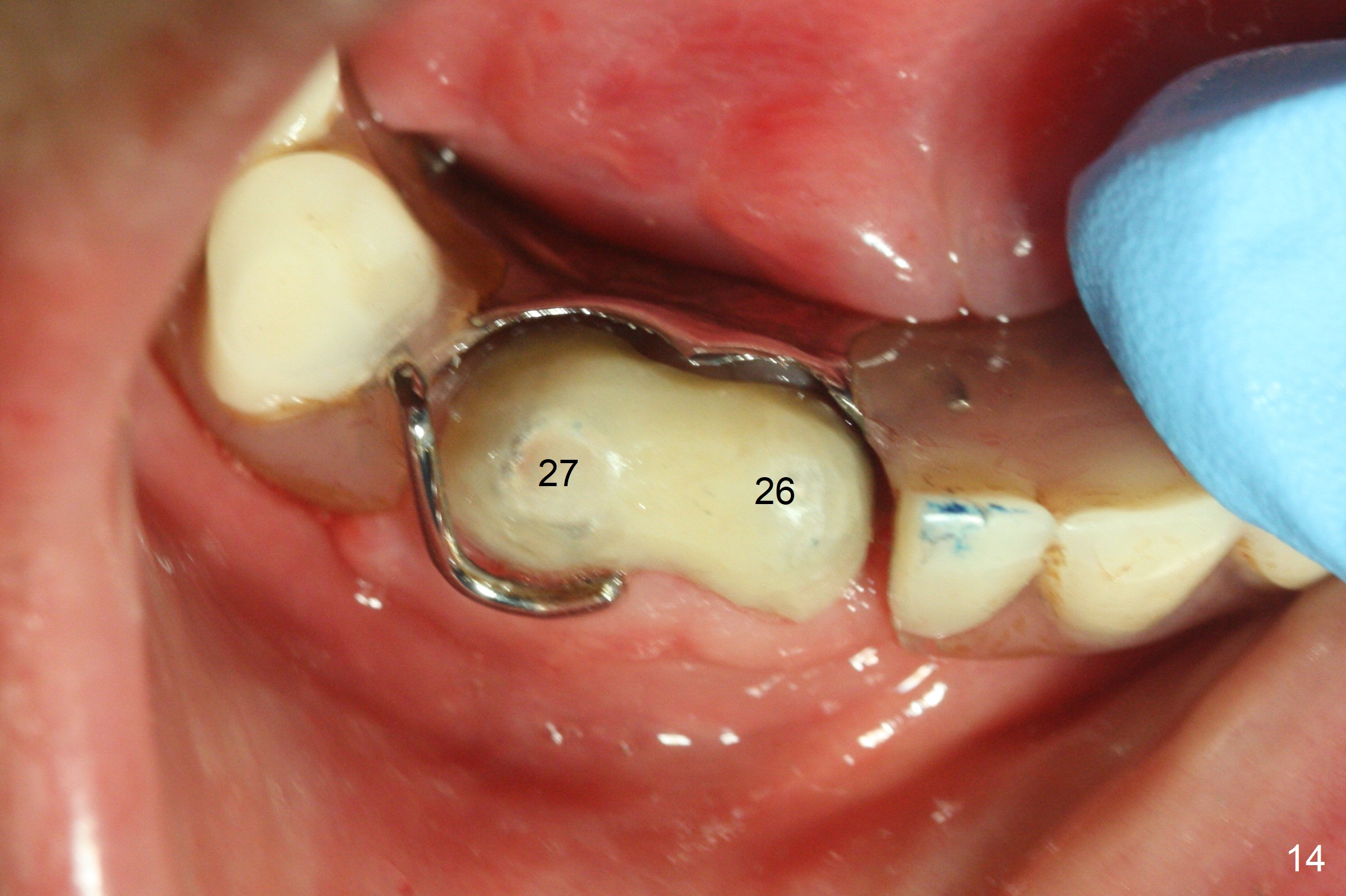
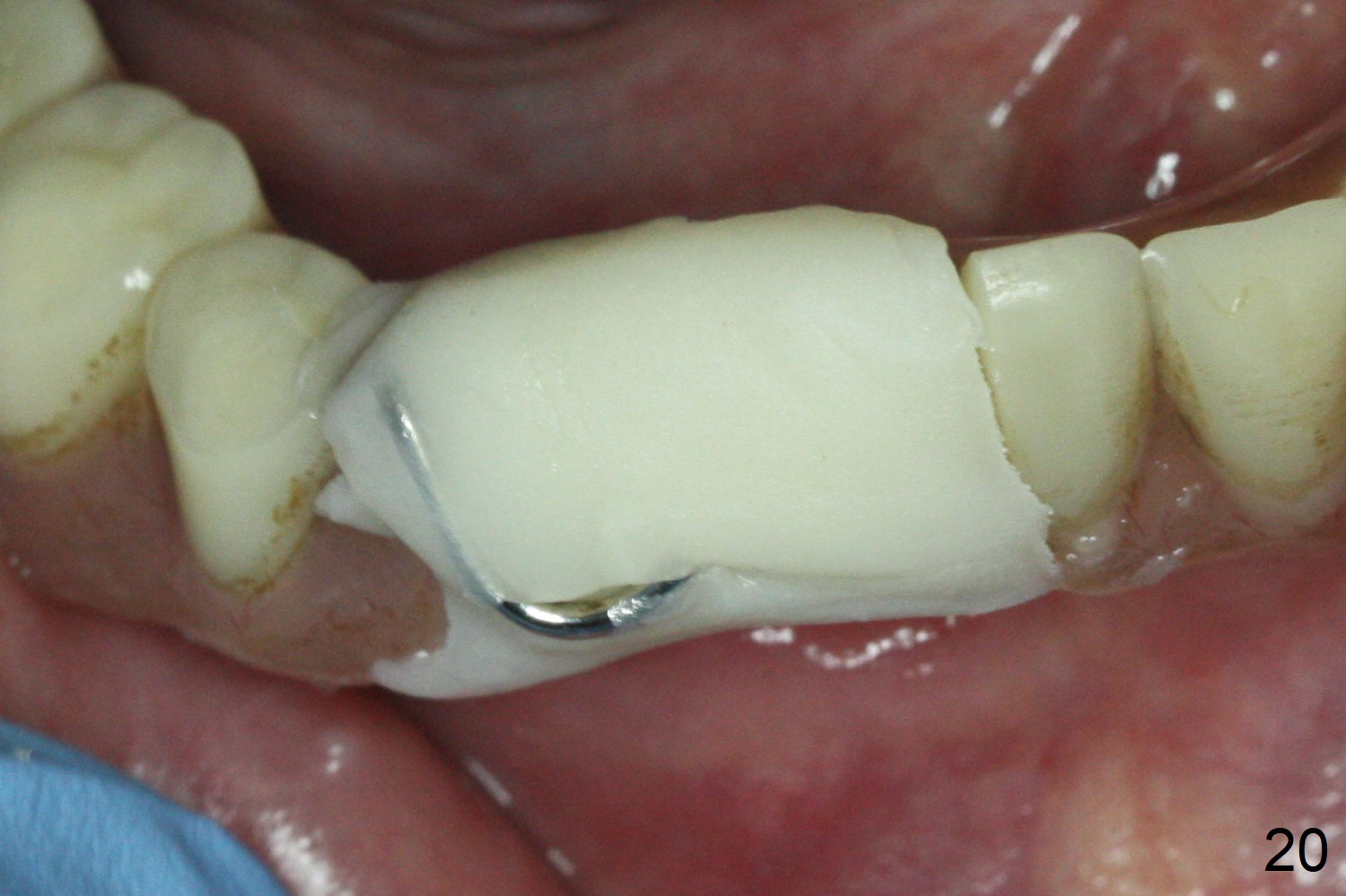
After change in abutment at #27 and abutment height adjustment at #26 and 27 (Fig.13), splinted provisional is fabricated with clearance from the RPD (Fig.14) and seal of the sockets (Fig.15). Acute submandibular and submental cellulitis develops with sublingual purulent discharge 1 month 10 days postop (Fig.16). CT confirms lingual plate perforation at both sites (Fig.17,18; red line: original socket). With block anesthesia, removal of these implants causes mild discomfort. With Hydrogen Peroxide and normal saline copious irrigation, pain reduces when anesthesia subsides. Bone graft will be placed at the sites approximately in 2 weeks. In fact the infection is not controlled until 2 weeks later (Fig.19). The clasp has to be covered with acrylic for comfort (Fig.20). The previous implant sites heal 1.5 months post implant removal (Fig.22).
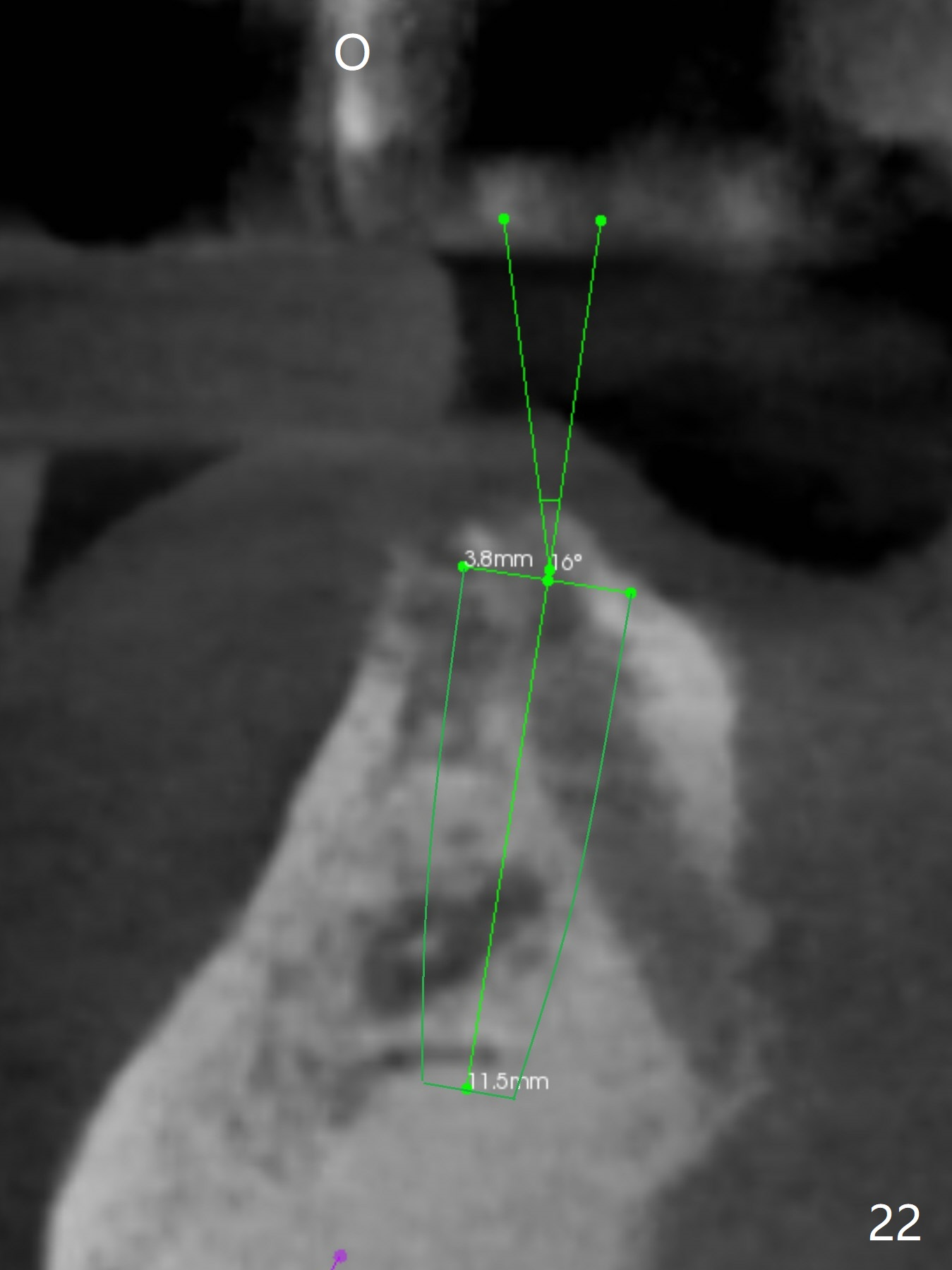
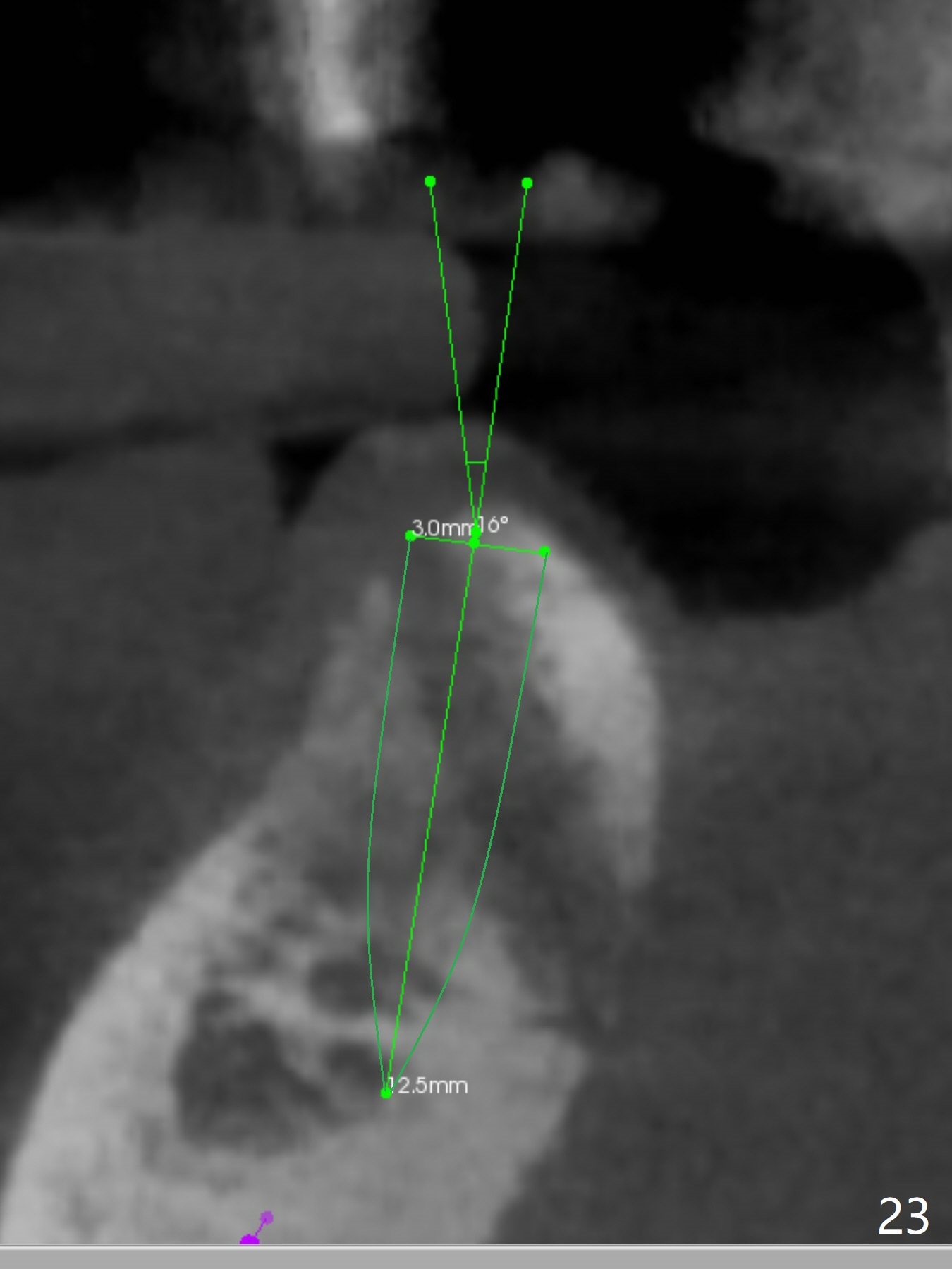
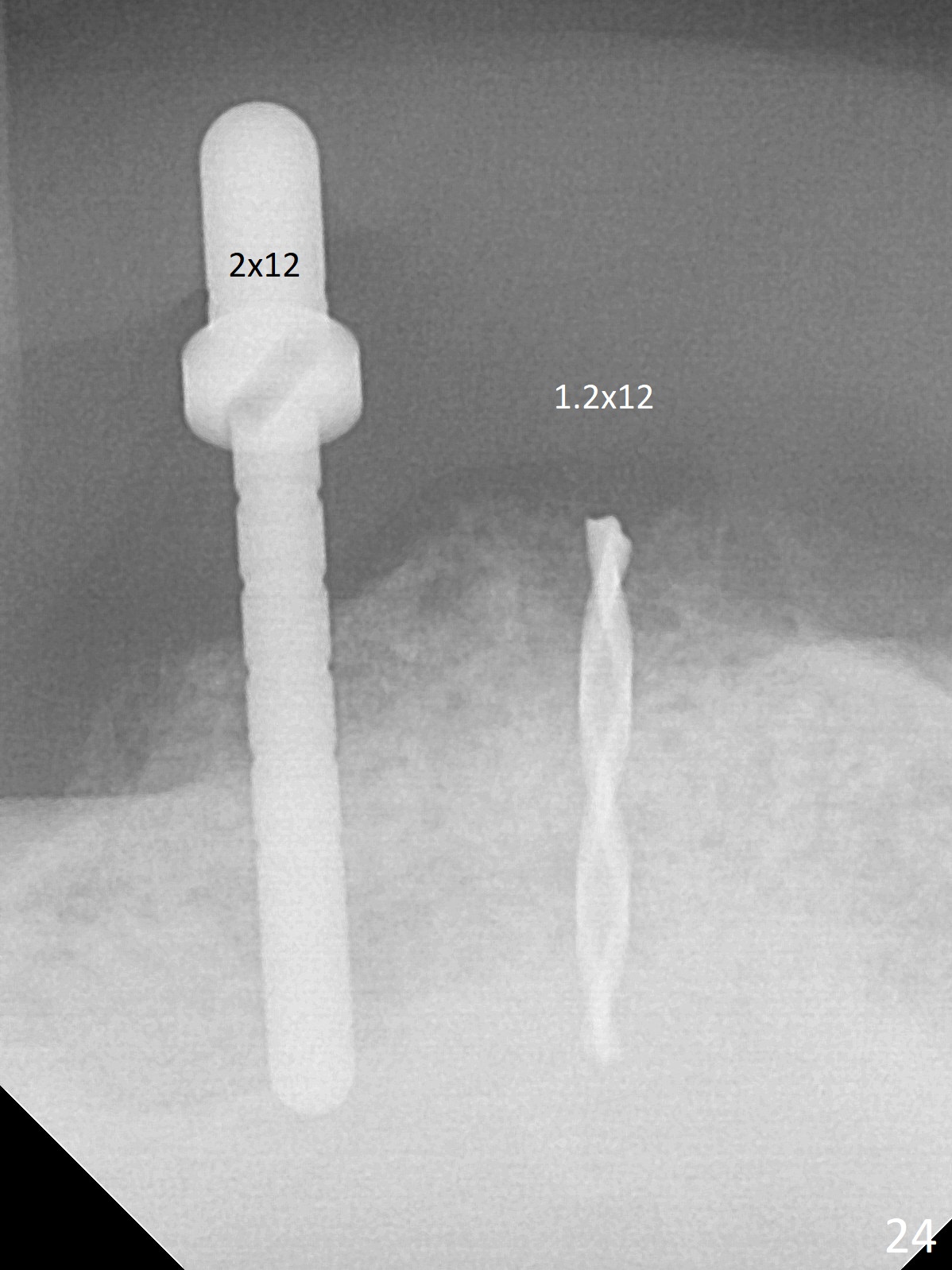
When the bone height seems to be limited in the lower anterior region, use short implants. CT is retaken nearly 2 months post implant removal (Fig.22,23 (O: opposing tooth)). It seems possible to re-place a smallest 2-piece implant where the bone is relatively wide (Fig.22) and a 3-mm 15 degree angled 1-piece implant where the bone is narrow (Fig.23) by simply changing trajectory. New implants are placed nearly 3 months post implant removal (Fig.24,25). In fact the site of #27 re-perforates; a shorter implant is placed with bone graft apically. Immediate provisional is fabricated so that the clasp is not irritating. There is moderate edema and pain lingual to #27 site postop. Augmentin is taken for 3 weeks with alleviation of the symptoms. The implant at #27 is loose 1 month postop and removed.
Return to
Lower
Incisor,
Canine Immediate Implant,
IBS,
Armaments,
Metronidazole,
9/11,
1-Piece,
Avoid Complication,
#20,21,28
Xin Wei, DDS, PhD, MS 1st edition 07/15/2017, last revision 01/19/2018