













|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
||
Over-Lingual Placement
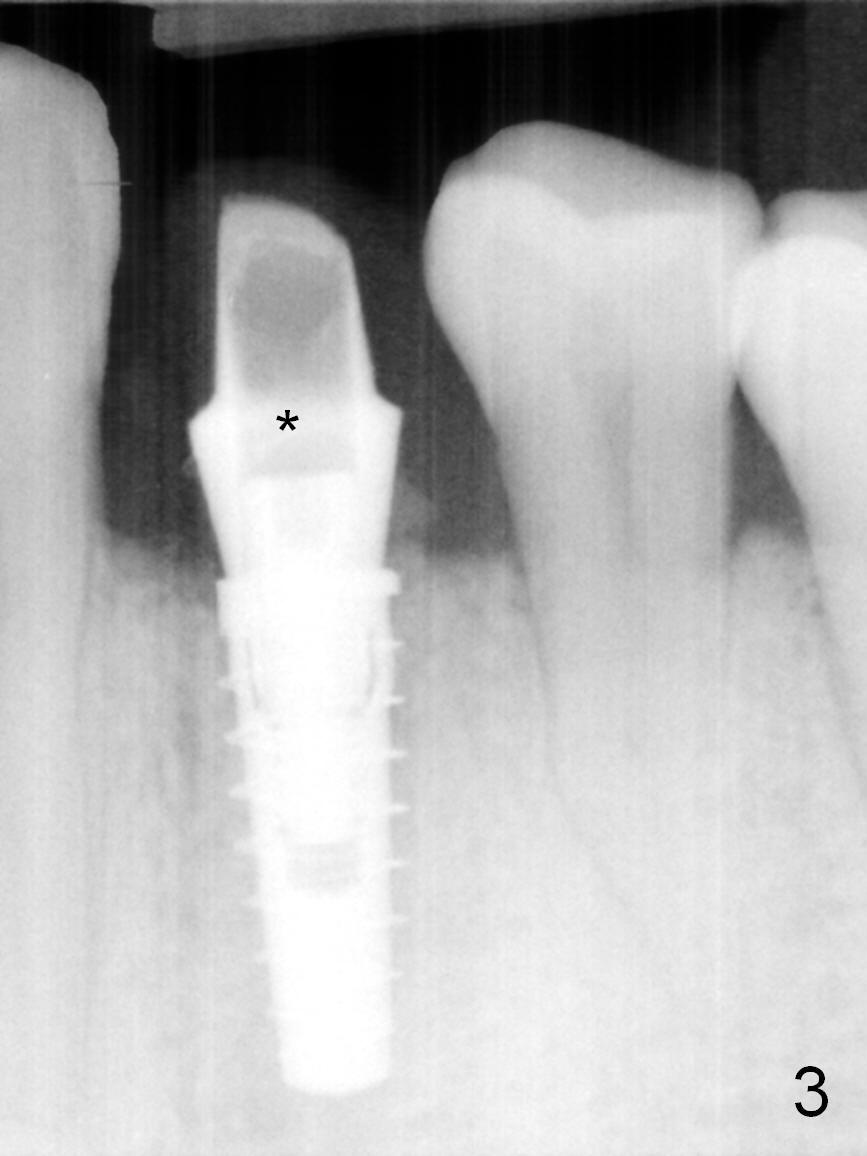
The residual root at #21 seems to be buccally positioned (Fig.1 *). The initial osteotomy is established with the 1.6 mm drill at 11 mm (Fig.2). Later the depth increases to 13 mm. The initial osteotomy is found to be too lingual, but experience shows that as osteotomy increases in diameter, the trajectory would shift buccally due to the thick lingual plate (slope). When 3.3 mm Magic drill reaches 11 mm, the patient feels pain. It is probably due to the dense bone. A 4x11 mm IBS implant cannot be seated due to high torque; it is removed. The osteotomy is increased with 3.8 mm drill. The implant is re-seated with >55 Ncm; it is over-lingually placed. Due to failure to seat the implant driver completely, the implant cannot be un-torqued. A 4.5 mm 15° angled abutment (3 mm cuff) is placed for immediate provisional (Fig.3,4 *).
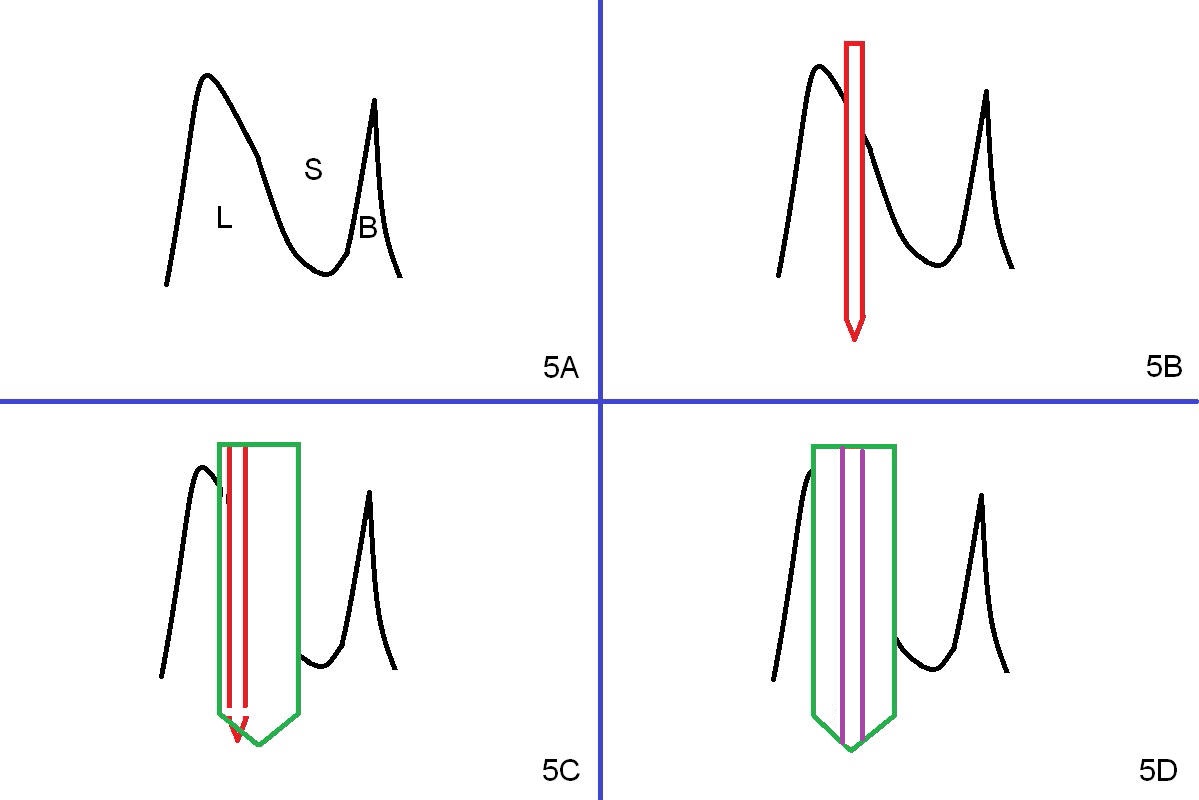
Fig.5A is a cross section of a lower premolar socket (S, illustration). The buccal plate is thin and low (B), whereas the lingual one is thick (L). When the bone density is high, Magic drills do not readily deviate from the intended osteotomy pathway (from Fig.5B to 5D). In contrast, the traditional multiple drill system tends to shift the osteotomy to the least resistant area (Fig.5C). Establish or correct the initial osteotomy early associated with IBS one drill system. When torque is more than 55 Ncm, remove the implant and use the next size drill or drill deeper with the last drill.
The patient returns for provisional revision 2 weeks postop (Fig.6). The bone graft remains in place (Fig.7). The buccal margin of the provisional is reduced (Fig.8).
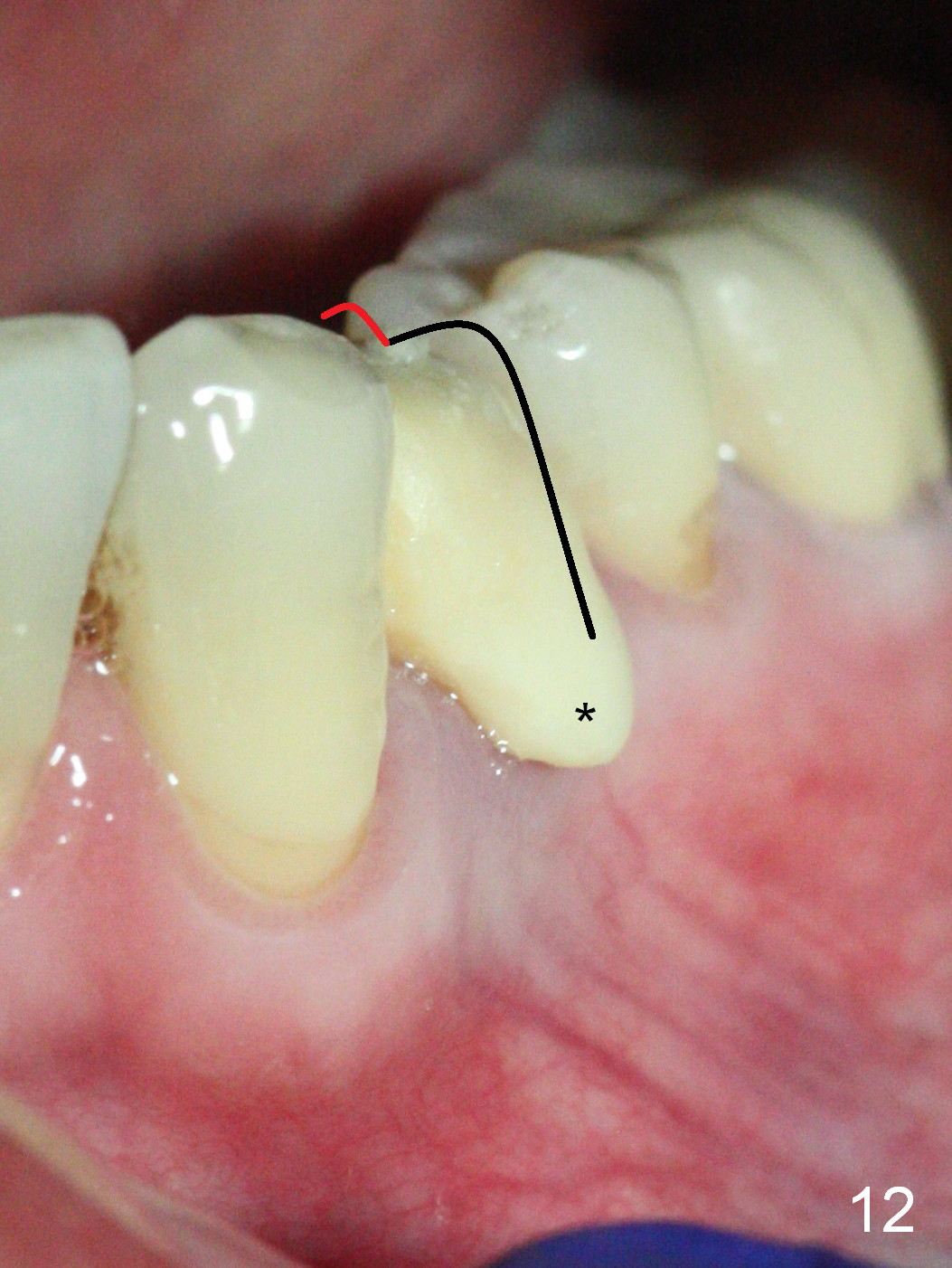
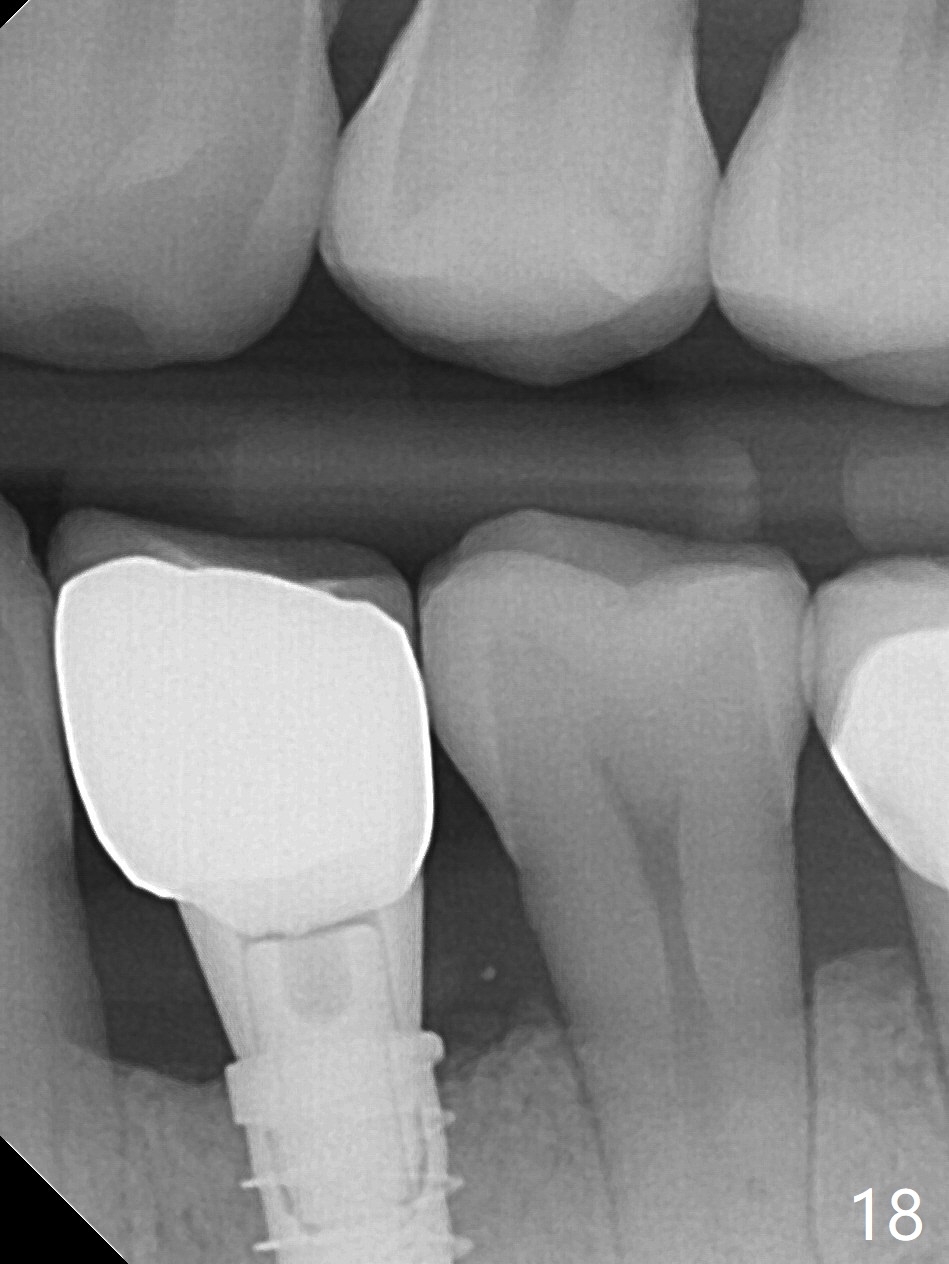
The implant seems to have osteointegrated 4 months postop (Fig.9). When a permanent crown is fabricated, it should have normal occlusal and buccal contour (from Fig.11 (provisional) to 12 red and black curved lines) as well as the buccal cervical extension (Fig.12 to cover the buccal gingiva (Fig.10 *). If the lingual margin of the abutment is too prominent, return the case and the abutment will be changed to the one with 2 mm cuff (existing 3 mm). The lingual margin of the abutment will be trimmed. The patient is not pleased with the short buccal margin of the crown after cementation (Fig.13). In fact the provisional should have been fabricated so that the its buccal margin should be subgingival and within the gingival outline. It may prevent buccal plate collapse. In fact the crown dislodges 1 year post cementation. The lingual margin is prep lower to increase the abutment height. Impression is taken. Although the access hole is unnecessary for cementation, it acts as an escape hole so that there is no excess cement cervically (Fig.14-18).
Return to
Lower Premolar Immediate
Implant
Section 2
Xin Wei, DDS, PhD, MS 1st edition 09/14/2016, last revision 02/07/2018